
Abstract
Background
Visual disturbances (VDs) are reported with an average rate of 1.4% after foam sclerotherapy (FS). Some clinical clues indicate that they could correspond to migraine with aura (MA).
Aims
To validate the hypothesis that VDs occurring after FS correspond to MA and are not transient ischaemic cerebro-vascular events.
Method
A prospective multicentre study was carried out by the French Society of Phlebology in collaboration with the Neurology Department of the Marseille University Hospital (France). We included prospectively and consecutively all patients who experienced VDs after FS using air to make the foam. The patients were assessed (1) clinically with a specific form describing procedures of FS and recording neurological symptoms, later analysed by a neurologist specialized in migraine; and (2) by a brain diffusion-weighted magnetic resonance imaging (MRI) (T1, T2, T2*, diffusion) carried out within two weeks and analysed by a neuroradiologist.
Results
Twenty patients, 16 women and four men, were included in 11 phlebology clinics. All kinds of veins were treated. VDs occurred in average seven minutes after FS. Clinical assessment showed that VDs presented characteristics of MA in all patients, with headache in 10 and without in 10. Paresthesia was observed in five patients and dysphasic speech disturbance in one. Fifteen patients (75%) had a personal history of migraine. Fifteen MRIs were performed within two weeks (mean: 8 days) and three were late (26 days). All of them were normal. MRI was not performed in two patients.
Conclusion
These results show that VDs occurring after FS correspond to MA and are not transient ischaemic cerebro-vascular events. We suggest a pathophysiological hypothesis resting on the release of endothelin that would reach the cerebral cortex through a paten foramen ovale.
Introduction
Visual disturbances (VDs) described after injection of sclerosing agent in the liquid form 1 appear to be more frequent after foam sclerotherapy (FS). 2 A meta-analysis 3 has revealed a frequency of 1.4%. The pathophysiology of this disturbance is not established. Some clues, based on clinical analysis, 3–6 indicate that they could correspond to migraine with aura (MA) and that they should not be confused with cerebro-vascular accidents.
The objective of this study was to validate the hypothesis that VDs occurring after FS correspond to MA and are not transient cerebro-vascular events.
Method
A prospective multicentre study was carried out by the French Society of Phlebology in collaboration with the Neurology Department of the Marseille University Hospital (France). We included prospectively and consecutively all patients who experienced VDs after FS. VDs could be isolated or combined with another disorder except for a motor weakness.
The gas used to make the foam was always air. Patients presenting a VD occurring after sclerotherapy with liquid were not included. The patients received information according to the French legislation and their informed consent for participation in the survey was recorded. Patients were asked to contact the practitioner if a VD occurred after they had left the phlebology clinic. Patients were assessed both clinically and with a brain magnetic resonance imaging (MRI).
A reporting form (Figure 1) was established to collect the patient's features, the FS features and a detailed description of the neurological symptoms. The patient's history of migraine, with or without aura, was also noted. The neurological description was set up and analysed by a neurologist (AD) specialized in migraine. The patient could be contacted by the neurologist if further details were necessary.

English translation of the reporting form
The diagnostic criteria of MA according to the International Headache Society 7 are presented in Figure 2.
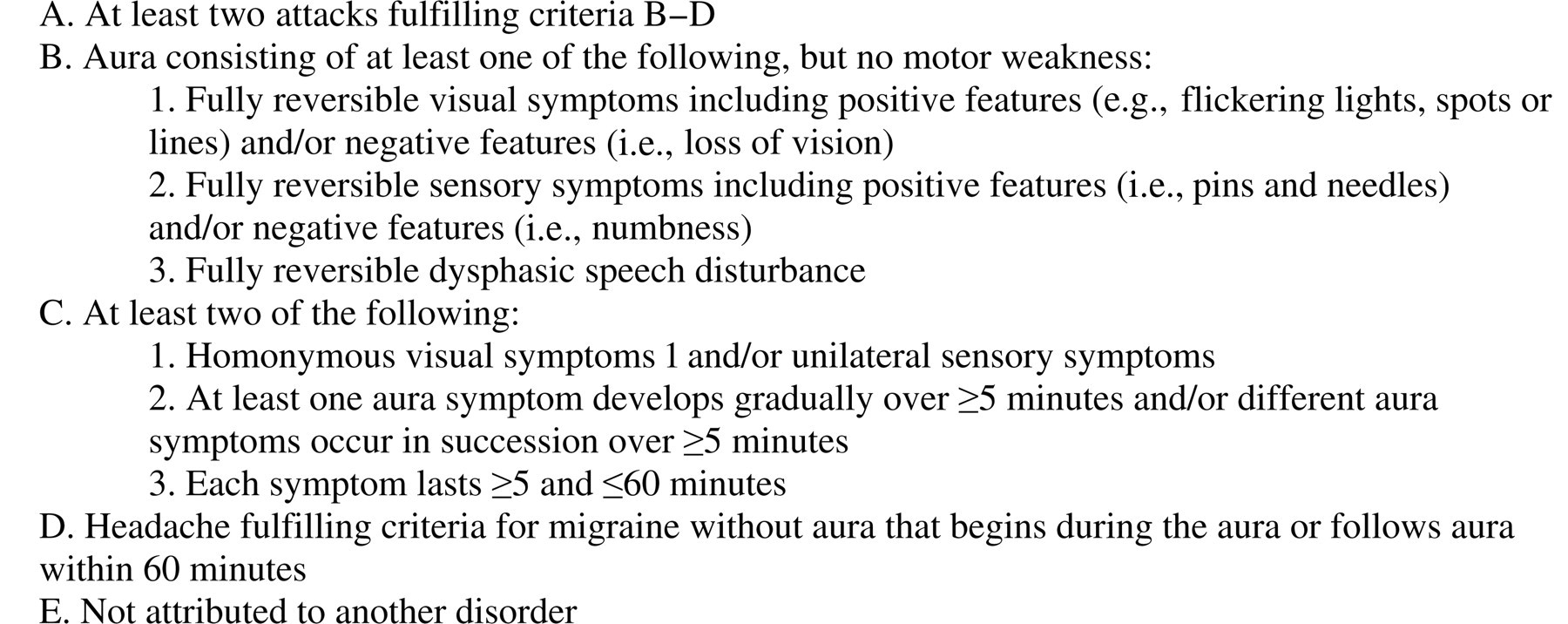
Diagnosis criteria of migraine with aura according to the International Headache Society
A brain diffusion-weighted MRI (T1, T2, T2*, diffusion) had to be performed within 14 days following FS. All MRIs were analysed with a double interpretation, firstly performed by the radiologist and then by a neuroradiologist (PL).
Patients were contacted between two and four weeks after the FS session by the practitioner who had treated them to assess the clinical outcome.
Data analysis was performed using the SAS 8.2 software (SAS Institute, Cary, NC, USA). Quantitative variables were expressed as mean ± standard deviation.
Results
Population
Twenty patients, 16 women and four men, were included in 11 French phlebology outpatient clinics. The average age was 46.75 ± 10.90 years (median: 44.50; range: 24–62 years). The clinical class was C2 in 16 patients (80%) and C3 in four. Seventeen patients were symptomatic suffering from symptoms secondary to venous disorders.
Various kinds of veins were treated including great saphenous vein trunk (n = 7), small saphenous vein trunk (n = 2), non-saphenous vein including recurrence after surgery (n = 7), accessory great saphenous vein at the thigh (n = 4), accessory saphenous vein at the calf (n = 3), perforating vein (n = 1) and telangiectasies or reticular veins (n = 5). FS was performed in the right leg in two patients, in the left leg in seven and in both legs in 11.
FS features
A double-syringe system 8 was used to prepare the foam in 17 patients and the Steriven® device 9 in three. The sclerosing agent was polidocanol in 19 patients and sodium tetradecyl sulphate in one. In accordance with the protocol, the gas used to prepare the foam in all patients was air. The concentration of the sclerosing agent ranged from 0.25% to 3%. The distribution of the concentration is described in Table 1.
Distribution of the concentration of the sclerosing agent
The total number is 24 because two different concentrations of sclerosing agent were used in four patients
The ratio of liquid to gas was 1:4 (one part of liquid plus four parts of gas) in 15 patients (75%), 1:5 in one, 1:6 in one and 1:8 in three. The average volume of foam injected was 5.60 ± 2.77 mL (median: 5.00; range: 1.5–10 mL). Direct puncture, or closed needle technique, was used in 18 patients (90%) and a short catheter or a butterfly in two.
The diameter of the needle used to inject the foam was 26G in five patients, 25G in nine, 23G in three, 22G in two and 20G in two (2 needles with different size were used in 2 patients). The average interval of time between the end of the preparation of the foam and the end of the injection was 60.50 ± 39.53 seconds (median: 50.00; range: 10–120 seconds).
Clinical assessment
All clinical forms were analysed by the neurologist (AD). Ten patients were contacted for supplementary information. VDs occurred in average 7.38 ± 6.48 minutes (median: 5.00; range: 0.5–30 minutes) after the end of the injections. In the majority of patients (11 = 55%), VDs lasted less than 30 minutes. The longest duration of VD was three hours. VD was a ‘positive’ trouble (e.g. flickering lights, spots or lines) in 12 patients and a ‘negative’ disturbance (i.e. loss of vision) in 13 (Figure 2). Five patients experienced both ‘positive’ and ‘negative’ disturbances. VDs involved one eye in seven patients (the right eye in 2 and the left eye in 4; for 1 patient the eye involved was not specified) and two eyes in 13 patients. Five patients (25%) presented paresthesia of the upper legs, associated with paresthesia of the tongue in two patients. One patient presented a dysphasic speech disturbance that lasted two hours.
Ten patients (50%) experienced a headache. It occurred after the beginning of the VD in 9 patients and at the same time in one. It lasted less than four hours in six patients, between four and 12 hours in one patient and more than 24 hours in two. The duration was not specified for one patient who experienced a slight headache. Thirteen patients presented other disturbances associated with aura. These were nausea (n = 10), photophobia (n = 6), phonophobia (n = 5) and chest pressure (n = 3).
Fifteen patients (75%) had a personal history of migraine: 13 (65%) with aura, and two without aura. All of the 13 patients with a history of MA stated that the VD was similar to the trouble they had previously experienced. Three of the five patients without personal history of migraine had a family history of migraine.
To sum up, clinical assessment showed that VDs presented clinical features of MA in all patients, with headache in 10 and without in 10. Paresthesia was observed in five patients and a dysphasic speech disturbance in one. All of the patients were contacted between two and four weeks. They reported that the disturbance had been transient and that no new symptoms had occurred.
MRI assessment
In accordance with the protocol, 15 MRIs were performed within two weeks following FS, with an average time of 8.07 ± 3.49 days (median: 8.00; range: 1–14 days). Three MRIs were performed 26 days after FS. The diffusion sequence was not carried out in one patient. MRI was not performed in two patients. All MRIs were normal. In particular, the analysis of the diffusion sequence showed no abnormality indicating an ischaemic lesion. White matter lesions were identified in five patients but these lesions are not specific. Three of these patients had a personal history of migraine.
Discussion
The frequencies of occurrence of VDs, as mentioned in the literature, vary from 0% to 14% 2,5,10–21 with a median rate of VD and headache of 1.4 and 4.2%, respectively. 3 Our data show that VDs can occur after FS in any kind of veins, any concentration of sclerosing agent and any diameter of needle. We observed a small percentage of telangiectasias in this cohort, which could be related to the decreasing use of foam in this indication. 2 The injected volume of foam was moderate (mean volume: 5.6 mL) and the average interval of time between the end of the preparation of the foam and the end of the injection was short (1 minute).
In France polidocanol is widely used as sclerosing agent, more commonly than sodium tetradecyl sulphate. 2,20 That probably explains why, in this series, VDs occurred mainly (95%) after injections of foam made with polidocanol. The type of gas (air or more physiological gas) to prepare foam is a controversial topic. In a recent work, Morrison et al. 21 did not find a significant difference of frequency of occurrence of VD by substituting CO2 for air even using a large volume of foam. In his series, the average air and CO2-based foam volumes injected were 27 ± 10 mL and 25 ± 12 mL, respectively. VDs seem to be more frequent if large volumes of foam are injected. In Morrison's et al study, 21 all patients who experienced VD had been treated with 15 mL or more of foam, except for one patient who had been treated with foam made with CO2. In his study including 808 patients treated with FS, Coleridge Smith 5 identified 14% of VDs. He injected up to 20 mL of foam. In our previous study about complications of FS including 1025 patients with incompetent great or small saphenous vein trunks, 20 we observed 1.5% of VDs; the average volume of foam injected was 4.5 mL.
Several authors have suggested that VDs could correspond to MA. Ratinahira et al. 4 reported a series of four patients presenting VDs after FS and suggested, with a clinical assessment, that this disturbance could be a MA. Coleridge Smith 5 noted that ‘patients with a previous history of MA were especially at risk of this problem’. In our previous study, 20 a relationship between VD and MA was established in some patients by the neurologist who analysed our data.
Demonstrating that VD corresponds to MA and is not a cerebro-vascular event is a crucial issue in the assessment of the safety of FS. This demonstration needed a clinical assessment carried out by a neurologist specialized in migraine, combined with a brain diffusion-weighted MRI analysed by a neuroradiologist. Diffusion-weighted MRI is the most sensitive tool for the detection of cerebral ischaemia. 22,23 It is a technique in which image contrast is determined by the motion of water molecules within tissues. In this series, MRI was performed in patients in whom the diagnosis of MA had been clinically suggested. The maximum period of time between FS and MRI has been discussed and set up by the neurologists. They considered that, in patients with a clinical diagnosis of migraine, the normality of a diffusion-weighted MRI performed within two weeks after FS eliminated a cerebral ischaemia. 22
All MRIs were normal. White matter lesions were identified in five patients but these lesions are not specific. Three of these patients had a personal history of migraine. Analysis of the literature 23,24 shows that white matter lesions are more frequently identified in patients with migraine.
According to neurologists, cortical spreading depression (CSD) is the pathophysiological correlate of MA. 25 CSD is a depolarization wave that -propagates at a rate of 2–6 mm per minute in the cerebral cortex. It starts in the occipital cortex and spreads towards the front. If it is limited at the occipital cortex, it only induces a visual aura; if it involves the parietal cortex, it causes paresthesia; if it reaches the temporal cortex, it leads to dysphasic speech disturbance.
The hypothesis that endothelin could be a triggering factor of CSD is supported by clinical observations and especially that angiography frequently provokes MA. 26,27 That suggests that endothelial irritation may somehow initiate one of the pathways resulting in MA. This hypothesis has been demonstrated in vivo in rats by Dreier et al. 28 He superfused the cortex of rats with endothelin-1. At a concentration range between 10 nmol/L and 1 µmol/L, all animals developed one to five CSDs. Endothelin-1, in contrast to K+, did not induce CSD in rat brain slices, suggesting indirectly that endothelin-1 may require intact perfusion to exert its effects. Endothelin-1 is a very potent vasoconstrictor.
On the basis of observational studies, a link between migraine and paten foramen ovale (PFO) is often suggested. Subjects with MA have a two-fold risk of being a carrier of PFO compared with the general population. 29–31 We suggest the following pathophysiological hypothesis of VDs occurring after FS. The endothelial irritation by the bubbles would release endothelin. In patients with PFO, or another right-to-left shunt, the pulmonary filter is short-circuited and endothelin reaches the cerebral cortex activating a CSD that induces MA. To validate this hypothesis, we should demonstrate that patients with VDs have a PFO. The results of Raymond-Martimbeau's study, 32 in which the presence of a PFO was detected in most of patients (5/7 = 71.4%) who experienced adverse events like VDs, MA or chest pressure after FS, reinforce our hypothesis, but it needs to be confirmed by further studies.
Conclusion
This study, based on clinical and MRI assessments, shows that visual disturbances occurring after FS correspond to MA and are not transient cerebro-vascular events. VDs presented characteristics of MA in all patients and all MRIs were normal. We suggest a pathophysiological hypothesis resting on the release of endothelin that would reach the cerebral cortex through a PFO. Endothelin has been demonstrated as being a trigger factor for MA. One logical step for investigation of endothelin-medicated neurologic events would be to demonstrate endothelin elevation in patients following FS.
Footnotes
Acknowledgements
We thank Drs F A Allaert, M Aurouet, F Bucci, J P Camuzet, G Gachet, J M Guedes, M Lausecker, J M Lecocq, B Marabelle, P Ouvry, C Poulain, H Skolka and C Zarca for participating in this survey, and the French Society of Phlebology for its support.
Disclosure
No potential conflict of interest to this article was reported.
Sclerosing agents used in this study may not be licensed in all countries; it is the responsibility of physicians to comply with local regulations.