
Abstract
A 58 year old female patient underwent an intervention of phlebectomy below the knee. The patient gradually developed a severe neurological event and the Glasgow Coma Score decreased dramatically. After two and a half hours from onset, general conditions gradually improved and recovered completely. Lidocaine neurotoxicity was excluded. A right side motor deficit strongly suggests a transient ischaemic attack. As to invasivity, phlebectomy can be compared with liquid and foam sclerotherapy so that the simple question arises of also comparing their adverse effects. We have the strong conviction that this case may only be a co-incidental association.
Introduction
A 58 year-old Ecuadorian female patient affected by chronic neck pain and non-insulin-dependent diabetes underwent an intervention of phlebectomy for varices of the left lower limb. She had no prior history of neurological events, venous thromboembolism, migraine headache and surgical interventions. She assumed only antidiabetic drugs.
Diagnostics
Clinical, aetiological, anatomical and pathological (CEAP) classification C2,S, Ep, AS2, Pr. Compression ultrasound (CUS) was negative for a deep vein thrombosis (DVT). The saphenofemoral junction terminal valve was incompetent. The preterminal valve and the great saphenous vein (GSV) trunk below showed a reflux less than 0.5 seconds. There was a functionally predominating type III shunt, 1 so that an anterior accessory great saphenous vein (AAGSV) phlebectomy with flush ligation of the GSV-AAGSV confluence was planned (Figure 1).
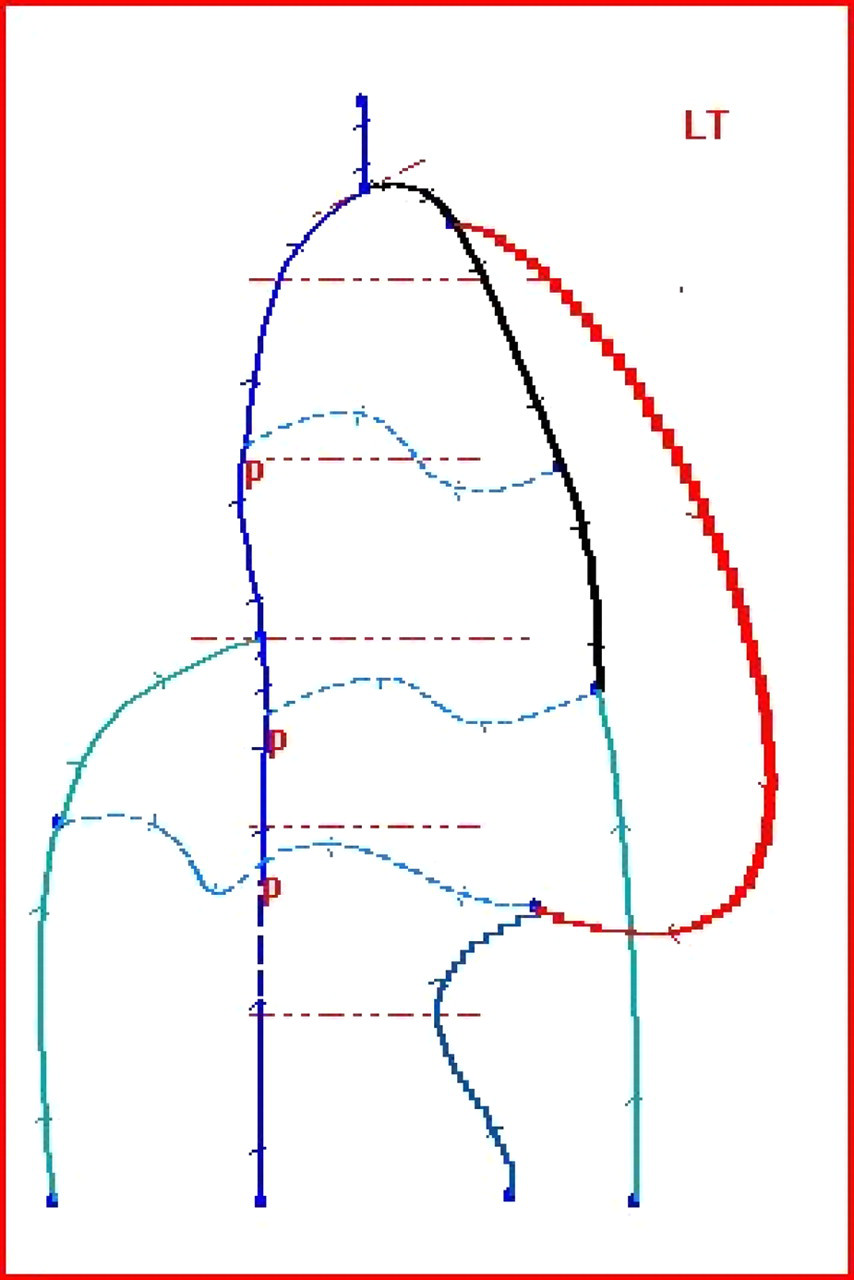
Computerized haemodynamic venous map (MEVc). Great saphenous vein and anterior accessory great saphenous vein incompetence. Two small thigh re-entry perforators. Functionally predominating type III shunt
Intervention
The patient received and signed an informed consent. Omeral arterial tension (OAT) was 110/70 mmHg and glucose 130 mg/dL, and general conditions were satisfying. The intervention was performed under local anaesthesia, injecting subcutaneously less than 10 mL of lidocaine 1% without epinephrine and starting with the phlebectomy of the below knee varices.
Neurological adverse effects
Ten minutes later, the patient suddenly noted a general discomfort and her conscious state changed progressively with a gradual decrease in the mobility and strength of the right arm.
The intervention was soon suspended and clinical assistance was organized by our intensive care unit (ICU) personnel.
Fifteen minutes later the clinical state was as follows: closed eyes with no change on stimulation, equal pupils, no verbal response, no localization and palpebral reflex still present. Babinski sign was absent on both sides, while a right side motor deficit with a light carpal spasm and an extrapyramidal cogwheel sign were present. The Glasgow Coma Score (GCS) 2 decreased from 15 to almost 3–6 (some reflex activity, difficult to classify). Pulmonary function was not affected and breath was spontaneous. In air (FiO2 21%) SpO2 was 93%, while it reached 99% with an ordinary oxygen mask (FiO2 23%), showing no oxygenation problem. OAT raised slightly to 140/70 mmHg and glucose was 121 mg/dL. D-Dimer measurement was not available. The electrocardiogram showed a sinus rhythm, an incomplete right bundle branch block and a 1 mm (chronic) ST depression.
The assistance was suddenly organized with a intravenous line, infusion of NaCl, atropine 1 fL and desametazone 1 fL. Spontaneous breath was still effective so that only breath surveillance was organized.
Brain computed tomography (CT) performed before the second hour was reported without ischaemia. Supra-aortic trunks EchoDoppler was negative, the peak systolic velocity was almost 60 cm/s on both sides and no minimal parietal lesions were detected.
After two hours from the onset, general conditions gradually improved. Right upper limb retraction to stimulation and spontaneous movements appeared, and the conscious state was gradually reached half an hour later, with complete symptoms recovery and a GCS 15.
The day after, a trans-thoracic echocardiogram (TTE) failed to reveal any cardiac anomaly, being also negative for a patent foramen ovale (PFO). No bubble test (BT) and no trans-cranial Doppler (TCD) were performed, although they were available.
After one day of hospitalization, the patient was discharged from the Medicine Department of the Military Hospital in complete neurological recovery and transferred to a neurological department for further assistance. Follow-up at 90 days, performed by Ecuadorian health personnel, showed that general conditions were satisfying.
Diagnosis
The intravenous injection of local anaesthetics effected by chance during a subcutaneous procedure was soon excluded, as it was performed in a few punctures, with no blood detection during aspiration. In addition, the dose was appropriate (almost 1 mL per puncture, for a total of less than 10 mL). Neurological adverse effects (NAE) with a right side motor deficit strongly suggest a transient ischaemic attack (TIA). 3 The cogwheel, however, is an extrapyramidal sign, which could arise from ischaemia of contralateral basal nuclei. Surely, it appeared perioperatively, as it suddenly disappeared.
A normal brain CT scan excludes a cerebral haemorrhage, while ischaemia can often be undetected within two hours. A small PFO can often be TTE negative (sensitivity is 68%), while BT and TCD in emergency were postponed and then not performed at all. However, bubble production is never reported in phlebectomy, being a PFO embolism considered only a remote hypothesis.
There is also the possibility of a PFO embolism from a venous thrombus. A concomitant pulmonary embolism and PFO mediated to the brain from a sudden thrombosis was soon excluded as oxygenation was adequate and quickly improved with an ordinary oxygen mask.
Considering that the patient was CUS negative and mapped completely in all her lower limbs venous system, thrombosis could have developed and embolized just in 10 minutes.
Discussion
Central nervous system (CNS) toxicity to lidocaine is a well-known adverse effect during spinal anaesthesia, being a cause of transient/permanent neurological deficit. However, local anaesthesia can also give transient neurological symptoms, in case of high dose, inappropriate site of injection (intravenously) or rapid reabsorbment. 4 In the present case the dose and the site were appropriate, while a rapidly reabsorbed ‘normal’ dose could be an eligible cause, being the clinical presentation similar.
When assisting this patient, we were helped by an ICU team with two anaesthesiologists. Considering the clinical presentation and the lateral expression of symptoms (right arm), we all were convinced we were treating a neurological event, as unilateral symptoms are difficultly related to a generalized neurological toxicity while no shivering, no seizures and no exciting phase were present. In addition, a respiratory or cardiac involvement was not observed, although often described in CNS toxicity by local anaesthetics.
Severe ischaemic as haemorrhagic NAE occur at the rate of 0.07–0.20% during general surgery interventions. 5,6 In selected kinds of interventions the rate can be higher, i.e. 8% in coronary artery bypass grafting 7 and 18% in re-operative and emergent abdominal aortic reconstruction.
Diabetes can also be a cause of increased risk.
A case of early postoperative stroke was reported in a patient with atrial septal aneurysm (ASA), operated for a resection of a retroperitoneal tumor. 8 Although not documented, there is a reasonable expectation that less invasive procedures have a much smaller rate, compared with more invasive ones, especially when performed in local instead of general anaesthesia. In these cases, diabetes should reasonably increase the risk as it does in general surgery.
As to invasiveness, phlebectomy can be compared with other actually well-spread methods used in phlebology, such as liquid and foam sclerotherapy, so that the simple question arises of comparing their adverse effects. In the last years several cases of differently-graded NAE were reported to be associated as to liquid 9 as to foam sclerotherapy. 10–12
Paradoxical embolism of foam or bubbles through a PFO or ASA or its functional analogues (A–V anastomoses in chronic obstructive pulmonary disease) 13–17 is hypothesized to be the cause of the NAE and bubbles can be effectively visualized, and tracked from veins to central and cerebral circulation. 18
The only procedures at low additional risk of NAE in phlebology are the surgical ones and, excluding this case report, between these there is also phlebectomy.
We have the strong conviction that this case may be only a coincidental association and no practical suggestion can then derive for the surgeon from this clinical experience.
Footnotes
Acknowledgements
Thanks to the ICU personnel of the North-American Surgical Team, working all together at the Riobamba Military Hospital ‘HB-11 Galapagos’, Ecuador, helped by the ‘Fundacion E1 Cielo para los Ninos de Ecuador.