
Abstract
Objectives
To assess efficacy and safety of polidocanol (POL) versus placebo in the treatment of C1 and C2 non-saphenous varicose veins in Chinese patients.
Methods
Patients were randomly assigned to POL or placebo. POL 0.5%, 1% and 3% were administered depending on varicose vein type. Response after 12 weeks was defined as Grade 4 or 5 on a digital imaging-based five-point scale (C1 veins) or occlusion and/or absence of reflux >0.5 second (C2 veins). Safety was evaluated with a five-point scale and standard safety assessments.
Results
Two hundred and eighty-five patients were treated. POL 0.5%, 1% and 3% were each superior to placebo (P < 0.001); response rates: 87.1% versus 13.6%, 86.4% versus 12.5% and 88.6% versus 4.3%, respectively. Significantly more POL than placebo patients were satisfied/very satisfied with treatment. POL was well tolerated, with mostly symptoms at the injection site reported.
Conclusions
Sclerotherapy with POL 0.5%, 1% and 3% was efficacious and safe in Chinese patients.
Introduction
Varicose veins are a common phenomenon in the Western population. Epidemiological studies such as the Bonn Vein Study, the American Venous Forum Screening Program or the Edinburgh Vein Study provide valuable information on the prevalence of varicose veins, patient age distribution and the degree of severity. 1–3 In an epidemiological study conducted between 1988 and 1989 in Shanghai, 30,712 subjects were examined for the presence of peripheral vascular diseases. 4 Varicosities of superficial veins were found in 2577 subjects (8.4%). In a study of chronic venous insufficiency in the Chinese population 5 , conducted 10 years later, 50% of limbs were diagnosed with C1-2 veins and 27.5% with C3-6 veins according to the clinical state, aetiology, anatomy, pathophysiology (CEAP) classification. 6
Sclerotherapy is recognized in many parts of the world as an efficient, low-risk and cost-effective treatment of lower-extremity varicose veins of all sizes. It is the treatment of choice for spider veins and reticular veins, and is commonly used for small- and medium-sized varicose veins. Furthermore, it has become a suitable treatment option for larger veins when used as foam.
Before this study was conducted, no ‘sclerotherapy tradition’ had existed in China to treat venous diseases. Up to now, no officially approved sclerosing agents (conforming to Good Manufacturing Practice requirements) are available in this country. However, surgical intervention techniques and thermal ablation therapy for varicose veins are well established.
The aim of this study was to show that sclerotherapy with Aethoxysklerol® (polidocanol [POL]) in Chinese patients with C1 veins and C2 non-saphenous veins is also an efficacious and safe treatment method. Due to the lack of experience with sclerotherapy, physicians were trained in the use of POL prior to the study.
Treatment success in large C2 veins can be determined by duplex examination or measurement of the venous diameter. Conversely, successful treatment of C1 veins is measured by improvement in appearance.
Methods
This was a prospective, multicentre, randomized, double-blind, comparative study conducted in China according to Good Clinical Practice (GCP) standards, approved by the State Food and Drug Administration and the ethics committees of the three participating hospitals. The objectives of the study were to assess the efficacy and safety of POL administered to three different patient groups defined by varicose vein type:
Group A: C1 spider veins of <1 mm; treatment: POL 0.5% or corresponding placebo (same solution but without the active ingredient); Group B: C1 reticular veins and/or small-sized veins of 1–5 mm; treatment: POL 1% or corresponding placebo; Group C: C2 medium-sized and/or large non-saphenous subcutaneous varicose veins of >5 mm with reflux of >0.5 second; treatment: POL 3% or corresponding placebo.
Study medication was manufactured by Kreussler in identical ampoules. Ninety-six patients were enrolled to each group. Patients were randomly assigned to POL or placebo in a ratio of 3:1. Each POL-treated group was compared with the corresponding placebo-treated group. The primary efficacy variable was the assessment of the efficacy of the study treatment at three months after the last injection as follows.
For Groups A and B, the same equipment and study procedures were used as in the ‘EASI-Study’ that was conducted to achieve marketing authorization in the USA. 7 The efficacy of the treatment was rated according to the following five-grade scale: 1 = ‘worse than before’ (more veins in the treatment area are observable than before or veins are more dilated or look worse than before), 0% disappearance but worsening; 2 = ‘same as before’ (no improvement but also no worsening observable), from 0% up to 25% disappearance; 3 = ‘moderate improvement’ (improvement observable but not yet satisfactory, needs to be treated again), from 26% up to 50% disappearance; 4 = ‘good improvement’ (satisfactory treatment success, only slight improvement still possible), from 51% up to 75% disappearance; 5 = ‘complete treatment success’ (no improvement necessary), ≥75% disappearance. Patients who had Grade 4 or 5 were counted as responders. For Group C, the efficacy of treatment was evaluated by duplex assessment, in which the vein was checked for occlusion and its reflux was measured. Responders were defined as patients with occlusion of the vein and/or absence of reflux >0.5 second and non-responders as patients who had neither an occlusion nor absence of reflux >0.5 second.
Secondary efficacy variables were the investigators’ and patients’ assessments of treatment satisfaction at the final examination according to a five-point verbal rating scale: 1 = ‘very unsatisfied’; 2 = ‘somewhat unsatisfied’; 3 = ‘slightly satisfied’; 4 = ‘satisfied’; 5 = ‘very satisfied’.
Overall safety was rated by a physician on a five-point scale: 1 = ‘one or more serious adverse drug reactions’; 2 = ‘treatment caused problems, more than three non-serious adverse drug reactions per treatment, daily life activity was impaired’; 3 = ‘treatment slightly tolerated, less than three non-serious adverse drug reactions per treatment, slight impairment of daily life activity’; 4 = ‘treatment well tolerated, less than three non-serious adverse drug reactions per treatment, no impairment of daily life activity’; 5 = ‘treatment very well tolerated, no adverse drug reactions’. Other safety variables were changes in vital signs, physical examination, electrocardiogram (ECG) and clinical laboratory measures.
Patients
Male and female patients between 18 and 75 years of age with C1 or C2 non-saphenous varicose veins of the lower legs and a normal deep venous system were eligible for the study after having given informed consent. The following conditions led to exclusion of the patient: history of deep vein thrombosis or high risk of thrombosis; arterial occlusive disease; thromboembolic diseases; acute severe systemic diseases or very poor general health; known hypercoagulability or current anticoagulation therapy; major leg oedema; febrile states; symptoms of microangiopathy or neuropathy or inflammatory skin disease in the treatment area; or predisposition to allergies.
Procedures
A maximum of three treatment sessions were allowed depending on the degree and extent of varicose veins, with treatment intervals of 2–4 weeks between sessions. If, according to the investigator, a complete improvement after the first or second injection was achieved and the patient was judged as a responder, then no further treatment session was necessary. The final examination occurred 12 weeks after the last treatment session.
To allow an unmistakable follow-up of the exact location of the treatment area and to maintain the same quality of photos during the study, a digital imaging system was used. Identical computer-driven cameras, with a black veil surrounding the camera and leg to exclude other light sources, were installed at each centre. Additionally, a section retrieval tool was developed that contains a base plate with grid co-ordinates to guarantee exact positioning of the patients’ leg, a vertical measure in centimeters and a spacer to standardize the distance between lens and leg (Figure 1). Each investigator also described and marked the area treated on a diagram. For both C1 vein groups (Groups A and B), digital photographs of the treatment area and the leg were taken at screening, immediately before the first injection and 12 weeks after the last injection (Figure 2). The images taken at Week 12 were compared with the images taken before first treatment, and the treated area was rated by the investigator using the five-grade scale to assess the efficacy, as described above.
Camera system (a–f): Images of spider veins (a, b), reticular veins (c, d) and C2 non-saphenous varicose veins (e, f), before (left) and after (right) treatment with polidocanol. (a) Patient 2081 (female, 49 years), two injection visits, total injected: 1.0 mL; (b) patient 1023 (male, 58 years), two injection visits, total injected: 1.3 mL; (c) patient 2091 (female, 36 years), two injection visits, total injected: 2.0 mL; (d) patient 2002 (female, 45 years), one injection visit, total injected: 4.6 mL; (e) patient 1055 (female, 71 years), one injection visit, total injected: 4.5 mL; (f) patient 1057 (male, 40 years), one injection visit, total injected: 2.2 mL

In addition, patients were instructed to wear a class II compression stocking on the treated leg during waking hours. The compression stocking was removed 24 hours before the next assessment to minimize compression marks.
Statistical analyses
Statistical Analysis System (SAS [SAS Institute Inc., SAS Campus Drive, Cary, North Carolina 27513, USA]) version 9.1.3 was used for all analyses. The hypothesis of superiority of POL over placebo in the primary and secondary efficacy variables was evaluated by Cochran–Mantel–Haenszel chi-squared test at a two-sided significance level of 0.05. Safety variables were summarized descriptively. Results of the overall safety assessment on the five-point scale were compared between treatments by the Cochran–Mantel–Haenszel chi-squared test and the incidence of adverse events (AEs) by Fisher's exact test.
Results
A total of 288 patients were randomized, 216 to receive POL (72 patients in each group) and 72 patients to receive placebo (Figure 3). Two patients assigned to POL 1% and one patient assigned to placebo did not receive any study medication and were therefore excluded from the safety population (n = 285). The full analysis set (FAS) included 206 patients treated with POL and 69 patients treated with placebo who had an efficacy assessment after treatment (Figure 3). The number of treatment days was 1.93 (POL) versus 2.91 (placebo) in Group A, 1.74 (POL) versus 2.70 (placebo) in Group B and 1.44 (POL) versus 2.70 (placebo) in Group C. The total injected volume was always lower with 1.97 mL (POL) versus 2.62 mL (placebo) in Group A, 2.11 mL (POL) versus 5.49 mL (placebo) in Group B and 2.21 mL (POL) versus 4.58 mL (placebo) in Group C. Twenty-four randomized patients (8.3%) in the POL group and nine (3.1%) in the placebo group discontinued the study. The most frequent reasons for discontinuation were loss to follow-up and AE. The per protocol set (PPS) included 185 patients randomized to POL and 62 patients randomized to placebo. Most frequent protocol violations were discontinuation of the study and not having an efficacy evaluation after treatment. The results of the PPS fully supported the results of the FAS presented below.
Distribution of patients. FAS, full analysis set; n, number of patients; POL, polidocanol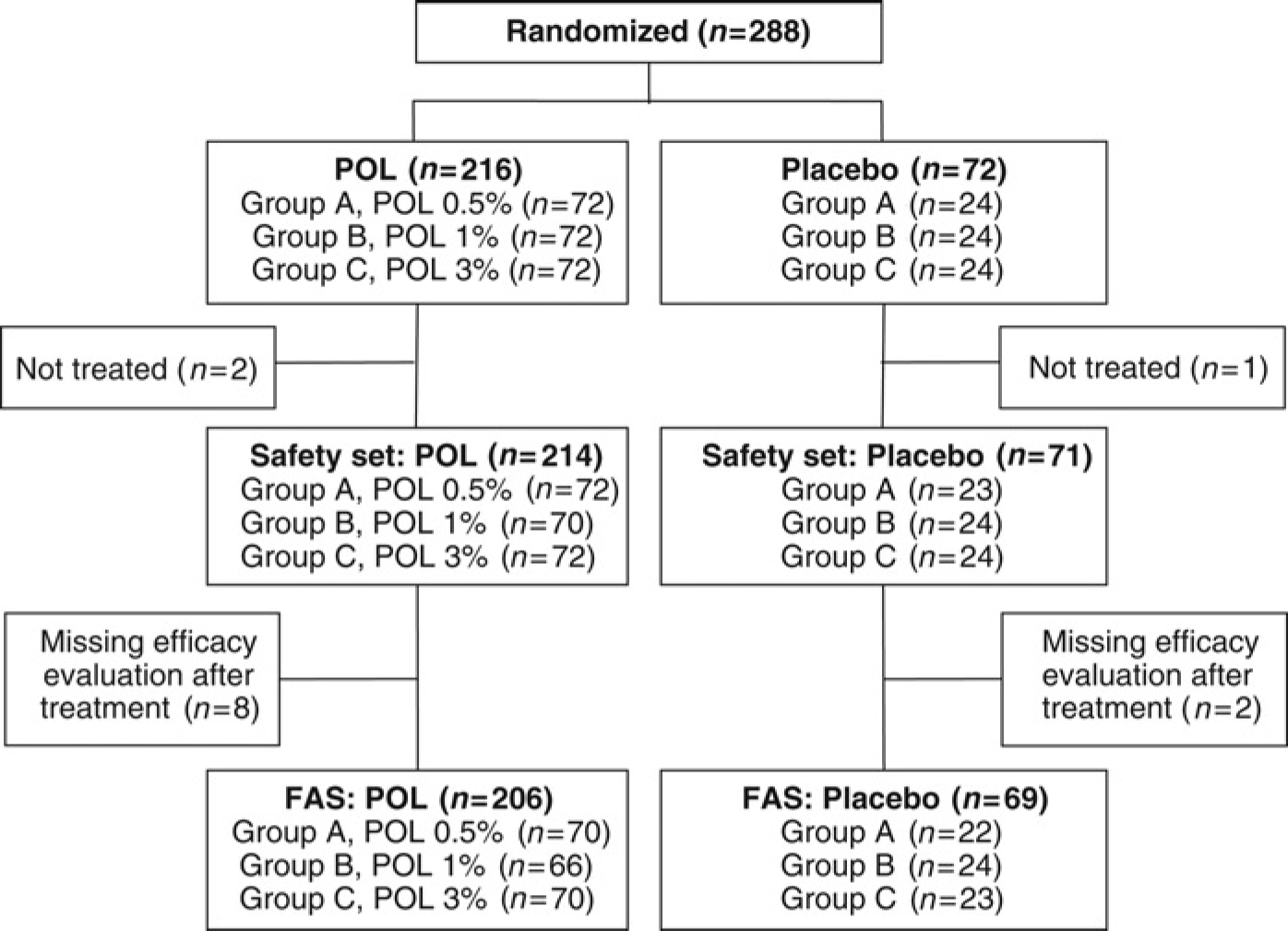
Demographic and baseline characteristics (full analysis set)

N, total number of patients; n, number of patients with characteristic; POL, polidocanol; SD, standard deviation
Treatment response
At Week 12, the number of responders in the FAS was significantly higher (P < 0.001; Cochran–Mantel–Haenszel test stratified by study centre) with POL than with placebo in each of the vein-type groups (Groups A, B and C; Figure 4), and thus superiority of POL over placebo was shown. Differences in the responder rates were even more pronounced in the PPS.
Percentage of responders at Week 12 (full analysis set). Group A: Polidocanol (POL) 0.5% versus placebo (spider veins of <1 mm); Group B: POL 1% versus placebo (reticular veins and/or small-sized veins of 1–5 mm); Group C: POL 3% versus placebo (medium-sized and/or large non-saphenous subcutaneous varicose veins of >5 mm with reflux of >0.5 second). Responders to treatment are those patients who were rated Grade 4 (‘good improvement’) or 5 (‘complete treatment success’) on a five-point scale
Patients’ and investigators’ satisfaction
In each vein-type group, both investigators’ satisfaction and patients’ satisfaction were significantly higher with POL than with placebo (P < 0.001 for each comparison; Figure 5). The majority (>60% in each vein type group) of investigators and POL-treated patients were ‘very satisfied’ with the POL treatment. In contrast, the majority (>60% in each vein type group) of investigators and placebo-treated patients were ‘very unsatisfied’ or ‘somewhat unsatisfied’ with placebo.
Percentage of satisfied or very satisfied patients at Week 12 (full analysis set): investigators’ assessment (left) and patients’ assessment (right) Group A: Polidocanol (POL) 0.5% versus placebo (spider veins of <1 mm); Group B: POL 1% versus placebo (reticular veins and/or small-sized veins of 1–5 mm); Group C: POL 3% versus placebo (medium-sized and/or large non-saphenous subcutaneous varicose veins of >5 mm with reflux of >0.5 second). Responders are those patients for whom satisfaction with treatment was assessed as ‘very satisfied’ or ‘satisfied’ on a five-point scale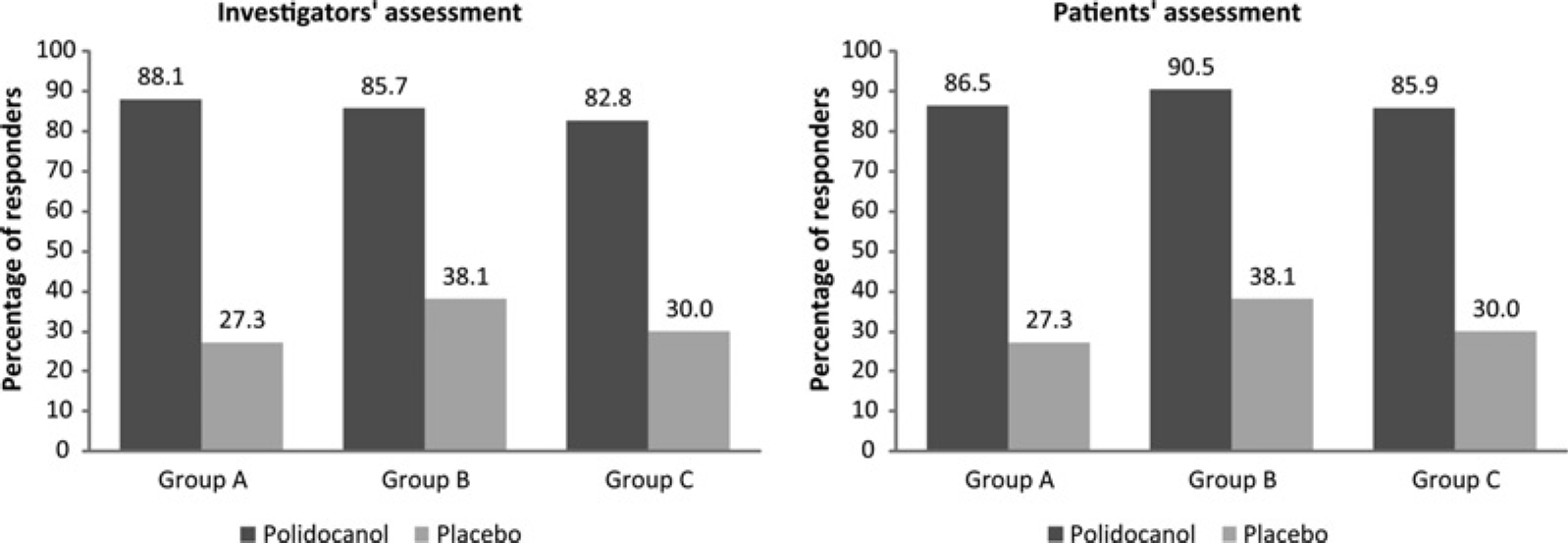
Safety
Treatment with POL 0.5%, POL 1% and POL 3% was safe and, apart from local symptoms at the injection site, well tolerated. According to the assessment of overall safety on a five-point scale, the treatment was ‘well tolerated’ (less than three non-serious adverse drug reactions per treatment) or ‘very well tolerated’ (no adverse drug reactions) for all treated patients except for two patients treated with POL 3%, whose treatment was ‘slightly tolerated’ (less than three non-serious adverse drug reactions per treatment, slight impairment of daily life activity).
Treatment-related adverse events during the study (by MedDRA system organ class, preferred term) – preferred terms reported by least 1% of all patients (safety set)
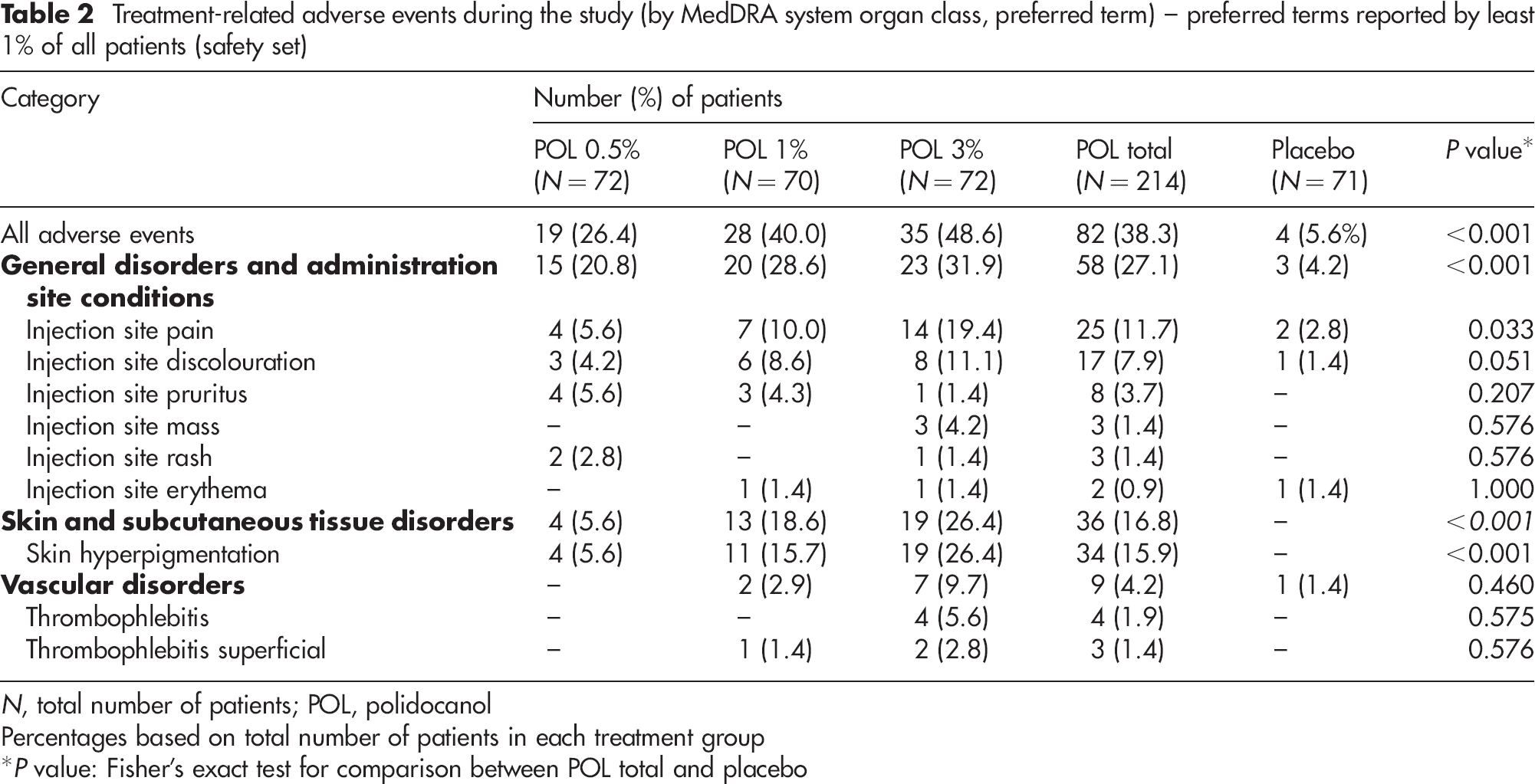
N, total number of patients; POL, polidocanol
Percentages based on total number of patients in each treatment group
*P value: Fisher's exact test for comparison between POL total and placebo
No clinically significant abnormalities were seen post-treatment in the ECG recordings, vital signs and clinical laboratory results (routine haematology, blood chemistry, urinalysis, blood coagulation).
Discussion
To our knowledge, this is the first controlled clinical study to demonstrate safety and efficacy of sclerotherapy with Aethoxysklerol® (POL) in the Han Chinese ethnic group. Sclerotherapy of Asian patients has already been successfully performed during the last couple of years, demonstrating that ethnic factors do not have an influence on the reliability of this treatment method. 8–10 The results of Groups A and B in this ESA-China Study clearly confirmed the findings from a multicentre study in Caucasian patients conducted in Germany (EASI Study). 7 In both studies, superiority of POL over placebo in the treatment of spider veins and reticular veins was demonstrated.
In addition to C1 varicose veins, C2 non-saphenous veins were also treated in our study. Despite the high success rates in the past of treating 3–6 mm varicose veins with classic liquid sclerotherapy, 11,12 the use of foam for non-C1 veins seems to be the preferred choice of treatment today. However, our study reiterates that classic liquid sclerotherapy remains a reliable treatment option, at least for non-saphenous veins.
In our study, 68% of the patients were ‘very satisfied’ and 20% ‘satisfied’ with their POL treatment. Similarly, high satisfaction rates were also reported in the EASI Study, where 84% of patients were at least satisfied with POL treatment, which was significantly higher than satisfaction rates for the active comparator sodium tetradecyl sulphate used in that study. 7
Most adverse reactions reported in our study were related to the injection site and are known non-serious side-effects of sclerotherapy. 13,14 Concerning both C1 vein groups, this is in agreement with the findings in the EASI Study, where treatment with POL was safe and, apart from local symptoms at the injection site, well tolerated. 7
An obvious weakness of this study is the length of follow-up, but for studies conducted for regulatory purposes under strict GCP conditions an observation period of one or more years is almost not realizable in comparison with open clinical trials or clinical series.
In conclusion, this multicentre ESA-China Study showed that treatment with POL (Aethoxysklerol®) 0.5%, 1% and 3% was highly effective and well tolerated in varicose vein patients of the Han Chinese ethnicity.
Footnotes
Acknowledgements
We gratefully acknowledge all co-workers in each study centre whose support was so important to the success of this study. All investigators appreciate the kind donation by Sigvaris, Switzerland, in providing each patient with compression stockings class II and the necessary support. We also thank Excel Pharma Studies (Beijing, People's Republic of China) for helping to conduct the study. Trilogy Writing and Consulting GmbH (Frankfurt, Germany) provided medical writing support on behalf of Kreussler.