
Abstract
Aim
To compare the efficacy of compression stockings and inelastic, high-pressure bandages concerning leg volume reduction in patients with chronic leg oedema.
Material and methods
Forty-two legs of 30 patients with chronic leg oedema caused by venous stasis were randomized to receive a strong inelastic bandage (IB) or an elastic stocking (ES) exerting a pressure of 23–32 mmHg. Changes in leg oedema were assessed after two and seven days by water displacement volumetry, measurements of leg circumferences and of skin thickness by using Duplex ultrasound. Interface pressure was registered under the compression devices for seven days.
Results
There was no significant difference between stockings and bandages, which both produced a significant reduction in leg volume after two days (−9.6% [95% CI 7.5–11.8] by ES and −11.5% [95% CI 9.9–13.2%] by IB) and after seven days (−13.2% [95% CI 10.4–16.2] by ES and −15.6% [95% CI 12.8–18.4] by IB). Bandages showed a more pronounced reduction in leg circumference and in skin thickness in the calf region. The pressure of IB in the lying position fell from initially 63 to 22 mmHg after two days, but only from 33 to 26 mmHg under ES (median values). The optimal pressure range concerning oedema reduction was found between 40 and 60 mmHg, while higher pressures produced by bandages showed a negative correlation with volume reduction.
Conclusions
Compression stockings exerting a pressure of around 30 mmHg are nearly as effective as high-pressure bandages with an initial pressure over 60 mmHg in reducing chronic leg oedema.
Introduction
The classical concept of care for patients with chronic oedema of the lower extremities recommends starting with a therapy phase, consisting of firm bandages, and then switching to a maintenance phase, in which the extremity should be kept free from oedema using compression hosiery. 1,2 One practical argument supporting this concept is the fact that compression stockings prescribed for a swollen leg would rapidly lose their fit and would need to be newly prescribed repeatedly, which can be quite expensive. On the other hand, bandages requiring trained staff and being frequently thrown away after a single use may also pose a considerable economic burden.
The aims of this study were: To clarify if compression stockings, in spite of much lower pressure, are able
to achieve a comparable volume reduction after a number of days compared with
inelastic bandages (IBs) applied with a much higher starting pressure; To check in which leg segments oedema reduction is most prominent under
compression stockings and bandages; To investigate the optimal pressure range for achieving maximal oedema
reduction.
Material and methods
Patients
Forty-two legs of 30 patients (10 men and 20 women aged 72.8 ± 9.7 years, range 57–81 years) affected by chronic leg oedema caused by venous stasis were randomized to receive a strong IB or an elastic stocking (ES) exerting a pressure of 23–32 mmHg.
Inclusion criteria included patients of each sex, aged between 18 and 85 years, suffering for more than three months from chronic oedema due to venous stasis (CEAP C3). The venous pathophysiology of oedema was investigated by a Duplex scanner (Esaote Technos® with linear probe 7.5–10 MHz, Esaote s.p.a. Genoa, Italy): 17 patients were affected by superficial venous insufficiency (C3 Ep AsPr); five by deep venous insufficiency (C3 EsAdPr,o); three by both superficial and deep venous insufficiency (C3 Ep,s As,d Pr); in five patients with restricted mobility and no venous pathophysiology, bilateral leg swelling was related to immobility or ‘dependency syndrome’ (C3 EnAnPn).
Exclusion criteria included patients younger than 18 or older than 85 years, patients with skin indurations due to venous insufficiency (CEAP C4-C6) or lymphoedema, cardiac failure, conditions requiring diuretics or cortisone treatment, and patients with an Ankle Brachial Pressure Index below 0.8.
Drugs and other procedures influencing leg oedema (diuretics, venotonic drugs, bandages or stockings) were stopped after enrolment and seven days before baseline oedema assessment (wash-out period) and remained discontinued for the study period, during which the patients were encouraged to maintain their usual lifestyle. All individuals were informed about the investigation and gave their written, informed consent. Ethics committee consent for the study was also obtained.
Primary endpoint was oedema reduction; secondary outcome parameters were the interface pressure of the compression device in the supine and standing position, and the comfort of the compression systems during day and night.
Timing
One week before starting the experiments the patients were randomly allocated to
treatment by means of IB or ES according to a list randomizer (
On day 0, measurements of oedema were performed and either ready-made compression stockings fitted to the individual legs or inelastic compression bandages were applied. Pressure measurements were taken after application.
On day 2, compression was removed, oedema was measured and compression was applied again; elastic stocking size was re-adjusted to the new leg volume. Interface pressure was measured before removing the old and after applying the new compression devices.
On day 7 (end of the study) the pressure of the compression devices was measured before compression removal and oedema measurement was repeated after compression removal.
Patients were always seen at the same time of the day (late afternoon).
Compression
Multilayer, multicomponent IB consisted of a cotton padding layer (Cellona®), a short-stretch, non-adhesive bandage (Rosidal K®) and a cohesive, short-stretch bandage on top (Mollelast®) (Lohmann & Rauscher GmbH & Co KG, Rengsdorf, Germany). The three components were applied in a spiral fashion, with 50% overlap between the layers, from the base of the toes up to 2 cm below the knee. Rosidal K® and Mollelast® were applied under full stretch to exert a strong to very strong pressure. 3
Elastic knee-length stockings were Mediven Forte® exerting a pressure range between 23 and 32 mmHg at B point as stated by the producer. The size was chosen according to the leg circumference using the smallest possible size.
In order to provide a fair comparison, stockings and bandages were worn day and night during the study period.
Measurements
Measurements were recorded during morning time in a quiet room, with a constant temperature about 22°C.
Three different methods were used to assess leg oedema: Leg circumference and skin thickness were measured at the following four segments: smallest ankle circumference (point B), at the transition between the medial gastrocnemius muscle into its tendon (B1), largest calf circumference (C) and below the patella (D). The measuring points on the leg were marked at time 0 in those four sites to allow the repetition of measurements exactly in the same place after two and seven days.
The interface pressure (IP) between the compression devices and the skin was measured in supine and standing position by means of Picopress® (Microlabitalia, Padua, Italy), a device based on the pneumatic method. 7 The pressure probe measuring 5 cm in diameter and less than 1 mm in thickness was placed at B1 point, the medial aspect of the leg where the tendinous part of the gastrocnemius muscle turns into its muscular part, and filled with 2 mL of air during measurement. After measurement at application the probe was disconnected from the measuring device and left in place under the compression systems. It was re-connected before the compression devices were removed, and supine and standing pressure was measured again.
The wearing comfort of the compression device was assessed by using a visual analogue scale (VAS) at times d2 and d7 (0 very poor comfort, 10 optimal comfort).
Leg pictures were taken at every visit using a digital camera.
Statistical analysis
A sample size calculation showed that 40 individuals in each group would have been necessary to detect a significant difference in volume reduction after two days in each group with a power of 80%. Since it was not the intention of this study to demonstrate superiority of one compression method over the other, but rather to check for a comparable outcome, we have restricted the number of tested legs to 21 in each group. Medians with interquartile ranges and maximal and minimal values are given. For repeated measures analysis of variance was used to compare the volume and pressure changes on the same leg. To compare the effects of bandages and stockings the non-parametric Mann-Whitney test was used. The non-parametric Spearman's rank test was used to quantify correlations. Differences with a P < 0.05 were considered statistically significant.
The graphs and the statistical evaluations were generated using Graph Pad Prism, version 5 software (Graph Pad, San Diego, CA, USA).
Results
Volumetry
Baseline characteristics
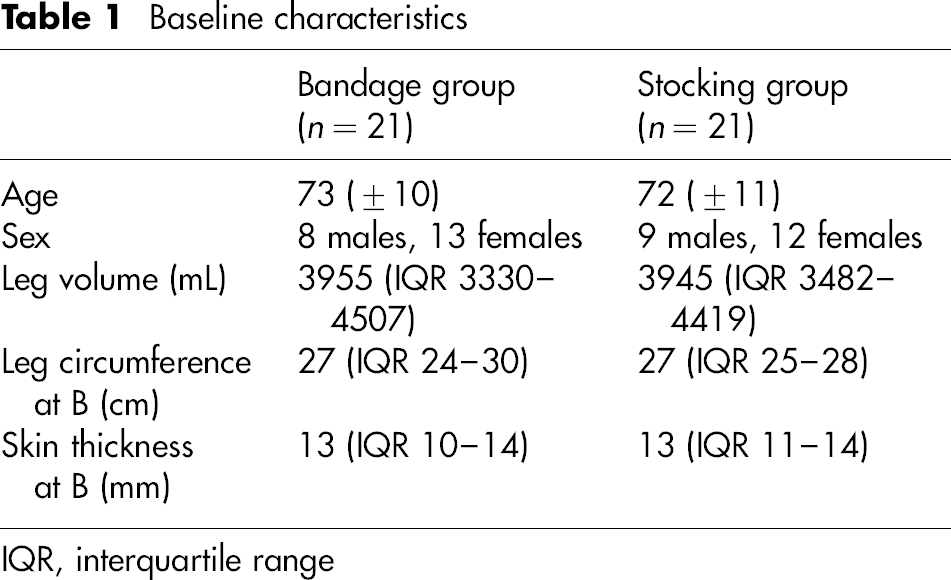
IQR, interquartile range
Both bandages and stockings achieved a significant reduction in the total leg volume
after two and seven days (P < 0.0001) (Figures 1a and b). There was no significant
difference concerning the effect of bandages and stockings after two and after seven
days. (a) A significant reduction in the leg volume was achieved both by bandages
and by stockings after two and seven days. Leg volume reduction compared
with initial volume is more pronounced in the first two days. Mean percent
change in comparison with the initial values is given. (b) Mean percent
volume reduction achieved by bandages compared with stockings after two and
seven days (no significant differences)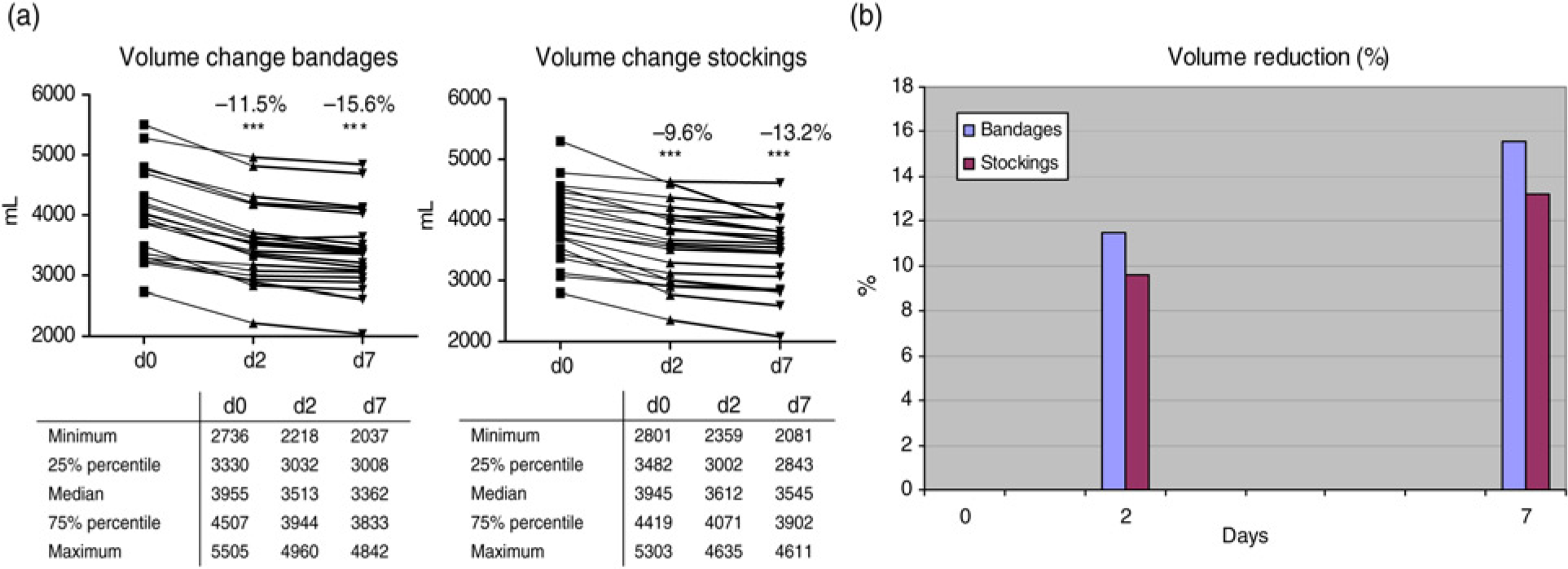
Leg circumference
Concerning the local effect of compression on different leg segments, bandages and
stockings reduced leg circumference at point B and B1 to a similar extent (no
significant difference), but at point C and D inelastic compression was more
effective (Figures 2a and b). Changes in the leg circumference at different leg segments with (a) bandages
and (b) compression stockings after two and seven days
Skin thickness
A significant reduction in skin thickness was observed at all leg segments, both by
stockings and by bandages (Figures 3a and b). Changes in the skin thickness at different leg segments with (a) bandages
and (b) compression stockings after two and seven days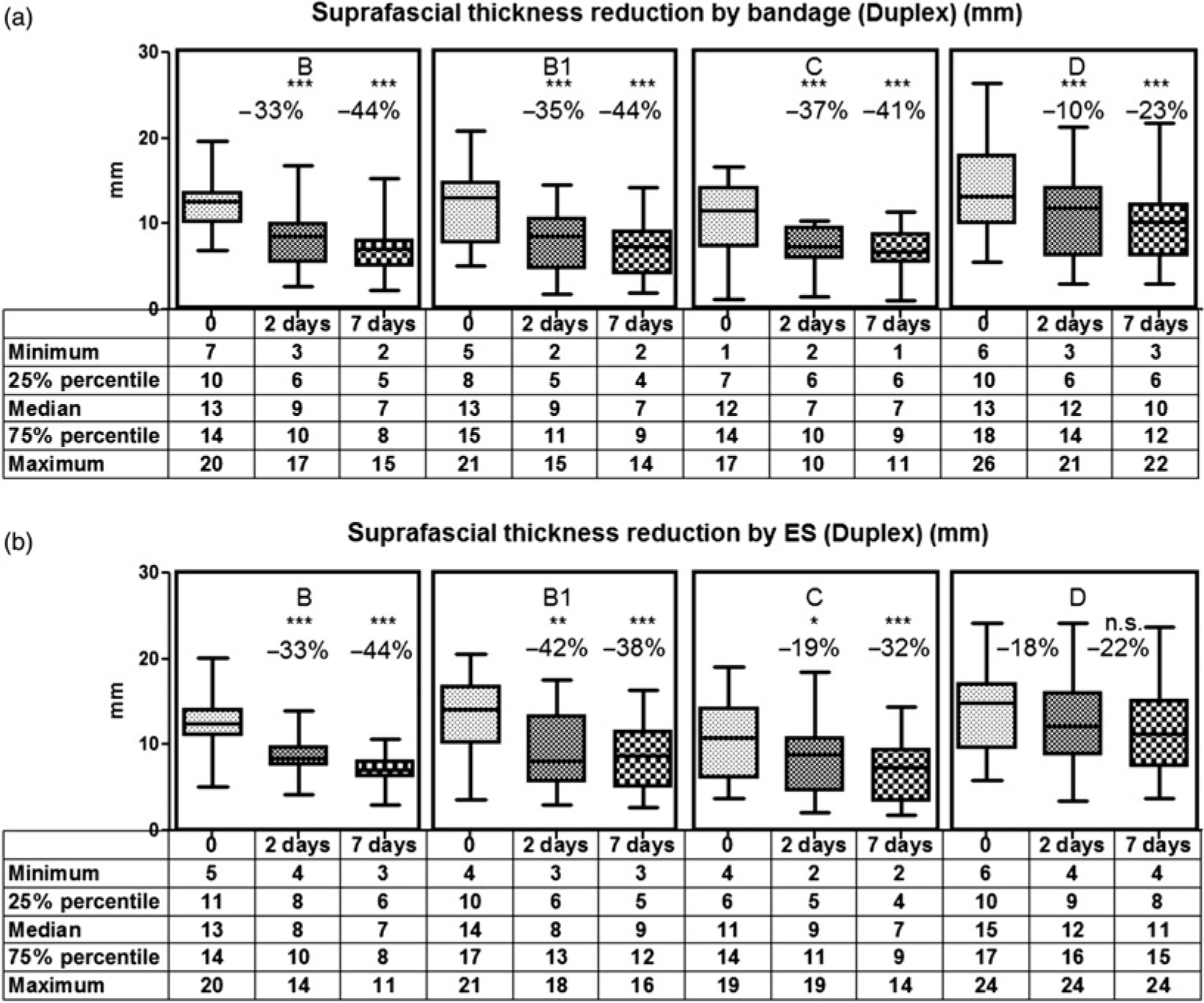
Interface pressure
IP was much higher with IB compared with ES, both in the supine (63 versus 33 mmHg)
and in the standing position after application (87 versus 36 mmHg) (P < 0.001) (Figure 4); two days later the supine pressure of IB was lower
than that of ES (22 versus 26 mmHg) (NS), while the standing pressure was still
higher with IB (35 versus 29 mmHg) (P < 0.05). On
day 7, the pressure of bandages and stockings was in the same range in the supine
position (28 versus 29 mmHg), while during standing IB still produced a significantly
higher pressure than stockings (41 versus 32 mmHg) (Figure 4). Median values of interface pressure measured at B1 under bandages (B) and
stockings (Sto) in the lying (L) and standing position (St) after
application (0), two days later before removal (b.r.), then after
re-application (d2 r.a.) and seven days later before removal (d7)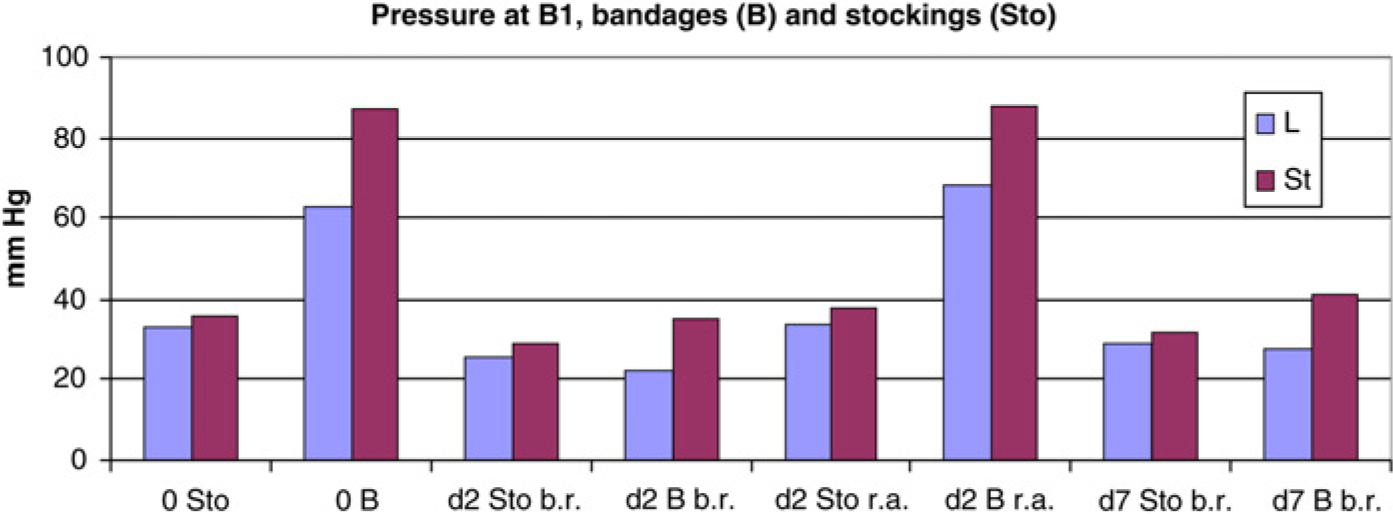
Patient comfort
Average comfort score assessed by Visual Analogue Scale during day and night in the first two days (left columns) and in the following five days (right columns) wearing bandages and elastic stockings (score 10 = optimal comfort, score 0 = unbearable)
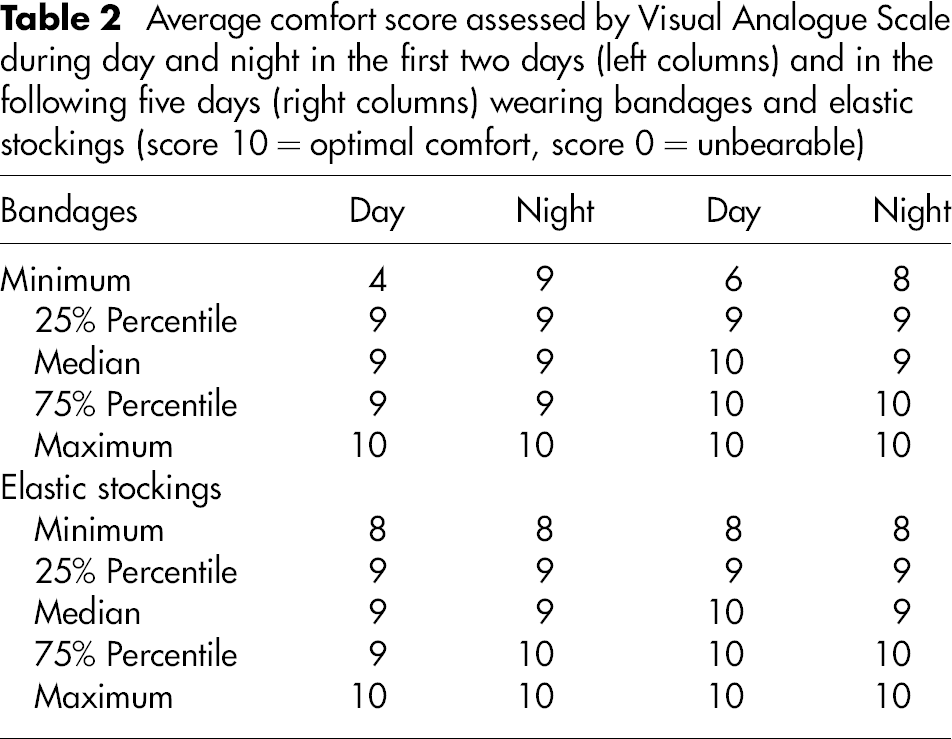
The continuous wearing of compression devices during day and night was well tolerated and did not cause any problems.
Discussion
The evaluation of leg volumetry by water displacement, tape measurements and skin thickness is a well validated method to assess oedema reduction by compression. 4–6,8–12
The present study has revealed some interesting results concerning the amount of oedema reduction achieved by compression hosiery in comparison with IBs, regarding the optimal pressure range of external compression and concerning the segmental distribution of oedema reduction on the leg.
Although it could be expected that IBs exerting higher pressure might lead to a more pronounced and faster oedema reduction, the mean percent reduction in the leg volume achieved by compression stockings was only slightly lower than that of compression bandages, both after two days (9.6% versus 11.5%) and after seven days (13.2% versus 15.6%). From a clinical point of view it remains an open question if a faster volume reduction could be of major relevance. It may be speculated that long-lasting oedema will rather be complicated by fibrosis and irreversible tissue changes so that faster oedema reduction could be beneficial. On the other hand, it has to be proved that a difference of a few days in reducing oedema can make any difference.
Oedema reduction increases with increasing pressure of stockings and bandages up to a
range of around 40 mmHg. Higher pressures, as produced by bandages, do not lead to more
pronounced volume reduction. In principle, this tendency can be shown by measuring leg
circumference, leg volume and skin thickness (Figure 5). Fitted line plots for exerted pressures (x-axis)
and oedema reduction (y-axis) assessed by the
measurement of leg circumference (left), leg volumetry (middle) and skin
thickness at segment B1(right)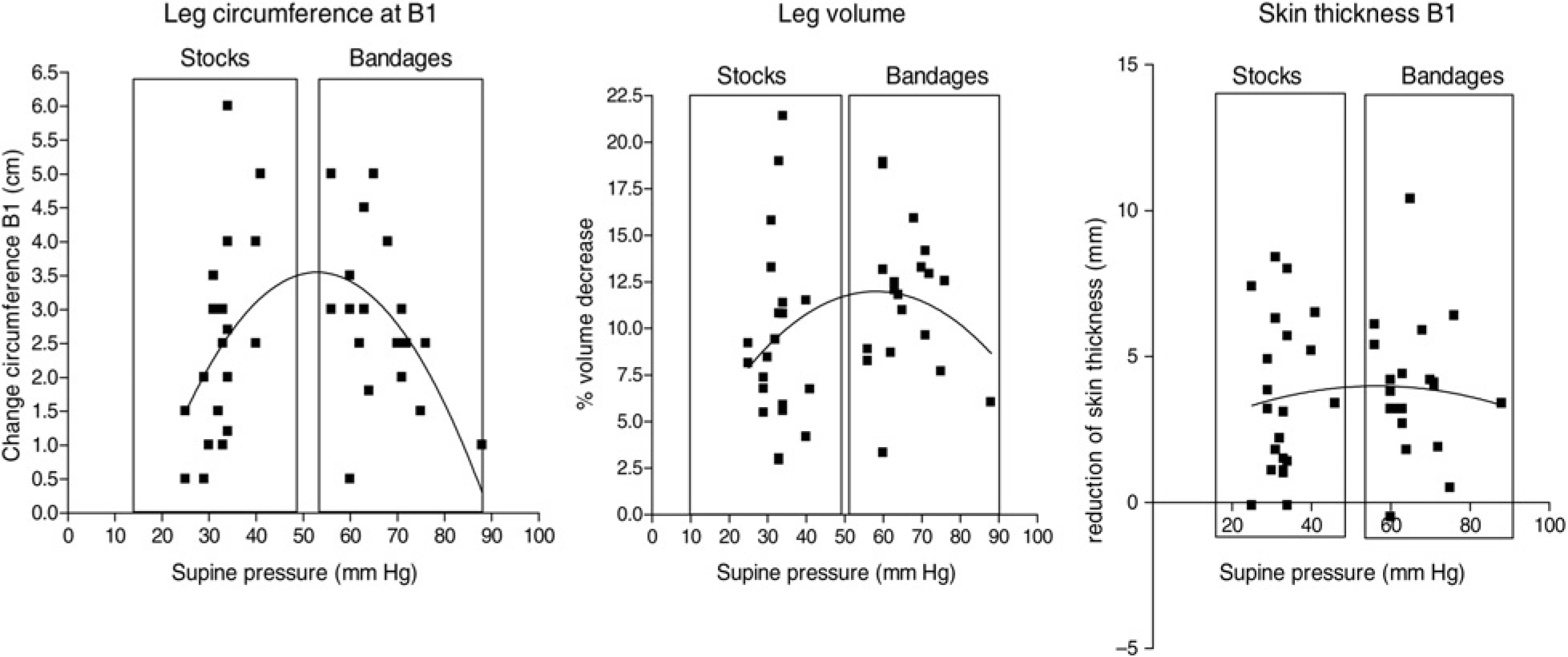
While stockings exerting a pressure range between 20 and 40 mmHg showed a significant
correlation between the pressure and the reduction of leg circumference (Spearman
r 0.52, P < 0.05),
bandages applied in a pressure range between 50 and 90 mmHg demonstrated less effect
under higher pressures, corresponding to an inverse correlation (Spearman r − 0.49, P < 0.05)
(Figure 6). Correlation between compression pressure (x-axis)
and reduction of leg circumference at level B1 (y-axis) for stockings (left) and bandages (right)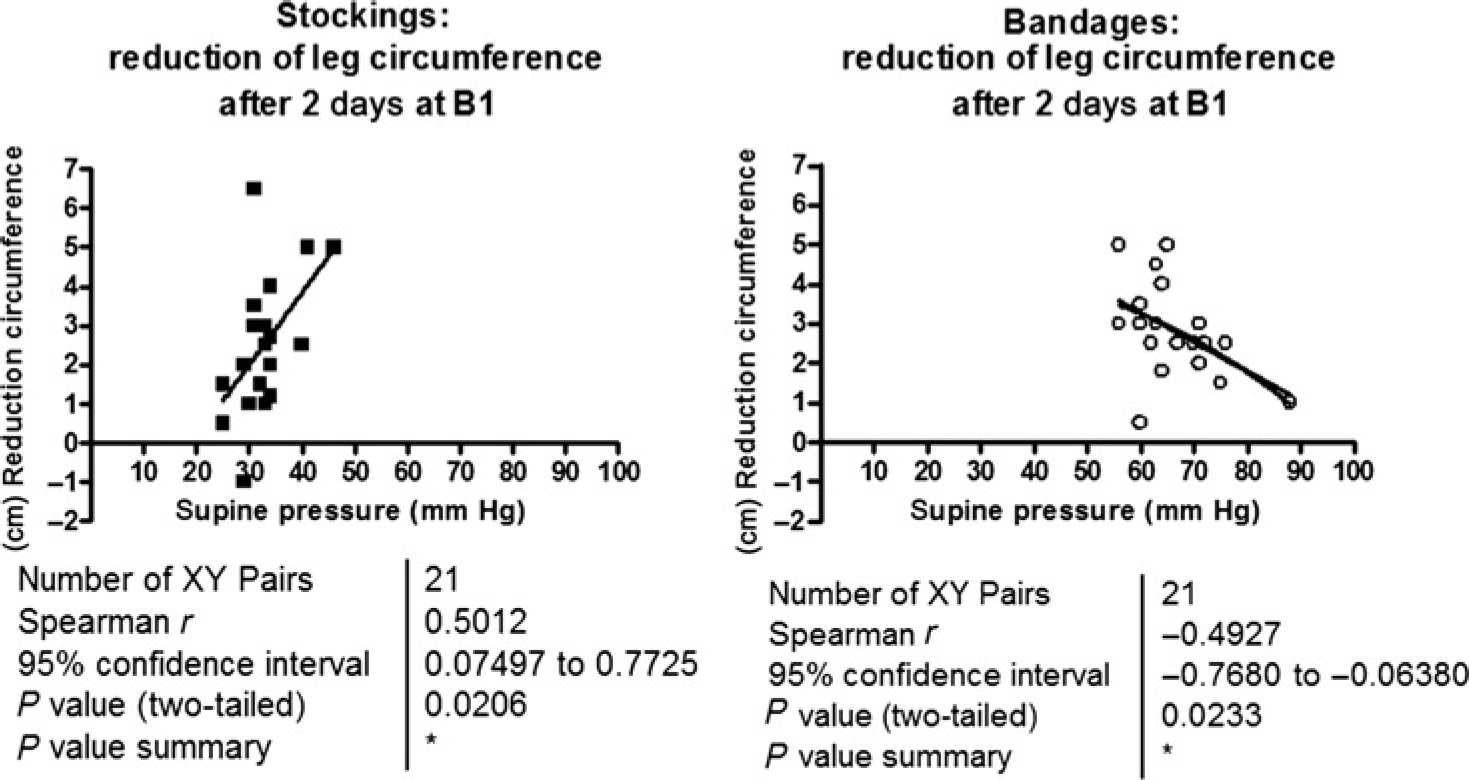
Concerning the localization of compression effects, bandages showed a more pronounced reduction in leg circumference than stockings, mainly in the calf region. The same was also true for the reduction in skin thickness and is probably due to the higher pressure of bandages over the proximal calf area.
The most interesting result of this study is the correlation between the pressure of the compression device and the extent of oedema reduction after two days. Initial bandage pressures higher than 70 mmHg do not lead to a stronger, but to a less pronounced volume reduction (Figure 5). Analogue paradox findings were reported in patients with arm lymphoedema, in whom a pressure between 20 and 30 mmHg was shown to be more effective than pressures over 50 mmHg. 13 The two main mechanisms of compression in reducing oedema are the reduction in fluid filtration from the blood capillaries and the enhancement of lymphatic drainage. The filtration pressure is a function of the pressure in the venules, which depends mainly on the body position. External pressures exceeding this venular pressure could be counterproductive, since they may have a negative effect on the lymphatic transport. 14
These findings related to volume reduction cannot be extrapolated to compression effects on the venous pumping function in patients with chronic venous insufficiency, in which intermittent pressure peaks of more than 80 mmHg during walking have been shown to increase the ejection fraction of the calf pump. 15
The Picopress device allows pressure to be measured not only after application of the compression stockings and bandages but also after some days, before removal. While elastic stockings keep their pressure relatively constant, IBs start to lose their pressure immediately after application, which is one of the reasons why such bandages should be applied with initially high or very high pressure. As was shown in our oedema patients, average bandage pressures starting with 60 mmHg fell to 20 mmHg after two days, which is then in the same range as the stocking pressure (Figure 4). However, in the standing position the IB has still a higher pressure than the stocking. The extensive pressure fall of IBs in swollen extremities may be explained by the volume reduction in the leg 16 and is the reason why such bandages will become loose and should be renewed after a few days. The oedema reduction and the consequent pressure drop occurring with bandages and, to a minor extent, with elastic stockings make the compression devices very comfortable, both during day and night time.
This study surprisingly shows that the reduction in leg oedema by elastic stockings was only slightly less pronounced than that achieved by high-pressure bandages. This could be an important argument for using stockings in the initial treatment phase of chronic oedema, especially taking into consideration that correctly applied IBs need training and experience, which is far less the case for the application of high-quality compression stockings. However, the practical use of hosiery is certainly limited by the fact that it would be necessary to prescribe new tighter stockings already after two days, which would certainly be a very expensive and unrealistic approach. Owing to the low size range of the high-quality stockings which were used, even two to three sizes smaller stockings had to be prescribed in some cases. On the other hand, this low size range could be responsible for the significant effectiveness we observed concerning oedema reduction.
Future studies are advisable to find a solution for this important restriction. One alternative could be providing a wide range of elastic stockings to the treatment centres, where they could be washed and reused. Another option could be to develop cheap, disposable, elastic oedema kits consisting of double-layer garments for the treatment phase, before the ultimate stocking is adjusted to the final leg size to prevent refilling of oedema.
Conclusion
Compression stockings are quite effective and can also be used in the treatment phase of oedema, provided that their size is re-adjusted to the reduced leg volume after initial decongestion. Bandages applied with a resting pressure of 60 mmHg and more do not lead to an increased capacity of oedema reduction.
Footnotes
Acknowledgements