
Abstract
Objective
Saphenopopliteal ligation (SPL) for venous insufficiency is a challenging procedure, with mixed results being reported. The role of stripping of the small saphenous vein (SSV) is contentious. This prospective observational study aimed to assess the risks and benefits of this procedure.
Methods
Fifty patients underwent SPL under general anaesthesia by a single surgeon in a tertiary referral vascular centre. The aim was to perform inversion stripping in each case, but in a proportion this was not possible. Patients were grouped into SPL with short segment excision ≤5 cm (n = 23) and SPL with extended stripping >5 cm (n = 27). Outcome measures included venous clinical severity scores (VCSS), quality of life (QoL), Aberdeen varicose vein questionnaire (AVVQ), patient satisfaction, recurrence and complication rates.
Results
Intragroup analysis demonstrated statistically significant improvements in VCSS (P < 0.001), and QoL measures (generic and disease-specific AVVQ) (P < 0.050) with both treatments. Intergroup analysis demonstrated statistically significant superior VCSS scores at one year (P = 0.001), AVVQ at three months and one year (P < 0.05), and cosmetic satisfaction at one year (P = 0.011) in the SPL extended stripping group. There was no difference in clinical recurrence 1/23 (4.3%) versus 1/27 (3.7%) (P = 0.900) or complication rates (P > 0.050).
Conclusions
SPL with or without stripping is an effective procedure improving clinical severity and QoL in the short term. Early outcomes favour SPL with extended stripping to offer greater improvement in disease-specific QoL, venous severity and cosmesis. With this small sample, there is no evidence of increased complications following stripping, or increased short-term recurrence without it. Greater numbers and follow-up are required to make firm conclusions.
Background
Varicose veins are a common problem affecting 10–40% of the adult population in the UK.1,2 Although the majority of such patients have saphenofemoral incompetence with great saphenous varicosities (GSV), isolated saphenopopliteal reflux may contribute up to 15% of patients with primary varicose veins. 3 Conventional saphenopopliteal junction (SPJ) ligation with or without stripping of small saphenous vein (SSV) has been the standard treatment for varicose veins associated with saphenopopliteal reflux. Despite the growing popularity of minimally invasive endoluminal treatment for varicose veins, SSV surgery is a procedure commonly undertaken by vascular surgeons. 4 A survey of the surgical members of the Vascular Surgical Society of Great Britain and Ireland on the management of SSV revealed up to two-thirds of the respondents performed over 15 saphenopopliteal ligation (SPL) procedures per year. 5 Incidentally the survey also highlighted the lack of consensus among surgeons on the best surgical technique for small saphenous varicosities; one of the key areas of contention being the role of formal exposure and ligation of SPJ with stripping of SSV in primary small saphenous incompetence. Mixed results have been reported in the literature associating SPL with extended stripping of SSV to increased incidence of complications especially nerve injury 6 and SPL without stripping to increased recurrence of varicose veins. 7 The objective of this retrospective cohort study using prospectively collected data was to evaluate the risks and benefits of this procedure in context to both the technical outcomes and the patient's quality of life (QoL) improvement.
Method
Patients
Fifty consecutive patients (50 limbs) presenting with symptomatic unilateral lower limb varicosities due to primary SPJ/SSV reflux underwent SPL by a single consultant vascular surgeon in a tertiary vascular surgical unit. All patients were examined clinically and assessed with venous duplex ultrasound scan (DUS) to confirm the diagnosis. Clinical severity of the limbs was objectively categorized according to the clinical, aetiological, anatomic, pathophysiological elements (CEAP) classification. DUS was performed with the patient stood and incompetence at the SPJ/SSV defined as reverse spectral flow trace of more than one second after distal augmentation manoeuvers. Patients with recurrent varicose veins, absent SPJ with or without incompetent giacomini vein, associated GSV and deep venous incompetence were excluded from this observational study. Patient demographics are as shown in Table 1. The intraoperative aim was to perform inversion stripping in each case, but in a proportion this was not possible. Patients were hence grouped into SPL with short segment excision ≤5 cm (n = 23) and SPL with extended stripping >5 cm (n = 27). All demographic variables between the two groups were comparable without significant differences (P > 0.050).
Demography and quality-of-life measures at baseline
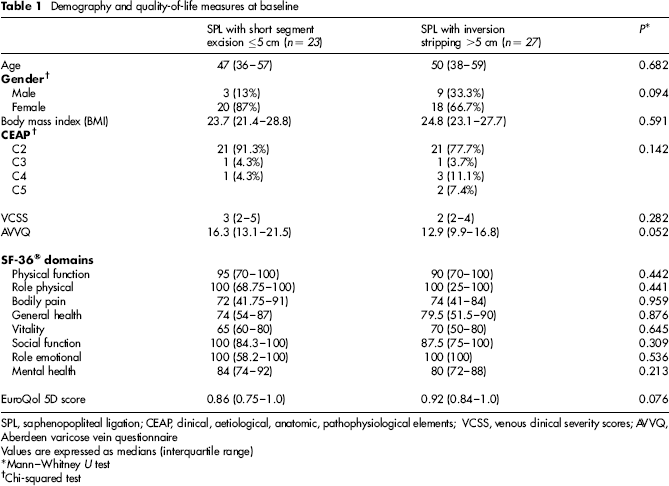
SPL, saphenopopliteal ligation; CEAP, clinical, aetiological, anatomic, pathophysiological elements; VCSS, venous clinical severity scores; AVVQ, Aberdeen varicose vein questionnaire
Values are expressed as medians (interquartile range)
Mann–Whitney U test
Chi-squared test
Surgical technique
Preoperative duplex marking of the SPJ was standardized for all patients and was performed by the operating surgeon with accredited certification in the use of ultrasound. The duplex established site of the SPJ and the course of SSV were marked on the overlying skin. With the patient in the upright position, the clinically obvious tributary varicosities were meticulously sought and intermittently marked to facilitate stab avulsions.
Surgical procedure involved formal exploration of the popliteal fossa under general anaesthesia (GA) with the patient in the prone position and access gained with a 3–5 cm transverse incision over the duplex skin mark. Absorbable suture material was used for the junctional ligation (Vicryl, Ethicon Endo-Surgery; Johnson and Johnson Company, Spreitenbach, Switzerland). The sural nerve was identified and protected when the SSV was dissected. No other nerves were exposed and retractors were placed with caution. PIN stripper (PS) (Credenhill Ltd, Derbyshire, UK) was inserted proximally into the divided end of SSV and advanced distally. The SSV was secured to the tip of PS with 2/0 Vicryl sutures and the palpable distal end of the PS delivered out along with the inverted vein through a small skin incision above the ankle. In the group where inversion stripping of the SSV was not possible, excision of a short proximal segment of SSV (≤5 cm) was attempted post-SPL. Stab incisions of 1–2 mm were made over varicose tributaries, and the veins were avulsed using a kocherized mosquito clip or vein hook. In both groups, stab incisions were closed with Steri-stripsTM (3M, St Paul, MN, USA), cotton wool and gauze. Panelast (Lohmann & Rauscher International GmbH & Co KG, Rengsdorf, Germany) elastic adhesive bandage was applied to the whole length of the treated limb postprocedure and left in place until the first follow-up at one week, when it was changed to a class II (30–40 mmHg) knee-length graduated support stocking that was worn for a further five weeks, except during sleep and bathing. All patients were asked to walk immediately postprocedure, and to return to normal activities as soon as they felt comfortable. A week's course of non-steroidal anti-inflammatory drugs was prescribed to all patients with no associated contraindication to their use as per surgeon's preference. No routine thrombo prophylaxis was prescribed unless indicated.
Data collection and follow-up
Pretreatment data collection included clinical severity of the varicose veins as categorized by the CEAP clinical stages and the venous clinical severity scores (VCSS). Generic QoL was measured using the Short Form 36 (SF-36®; Medical Outcomes Trust, Waltham, MA, USA) and EuroQol (EQ-5D) instruments, both of which have been validated to measure efficacy of varicose vein treatment.8–14 The Aberdeen Varicose Vein Questionnaire (AVVQ) has been shown to be a reliable, valid and responsive instrument to measure the specific impact of venous disease on patient's QoL.8–10 DUS findings, procedure duration, complications and length of SSV excised/stripped were recorded prospectively. Postoperative pain on days 1, 3 and 7 was recorded by the patient on a 10-cm visual analogue scale and additional analgesic requirement noted in the pain diary. The number of days to return to work and normal activities were also recorded.
Patients were followed up by the consultant vascular surgeon or an experienced research fellow at one week, six weeks, three months and one year. Each visit consisted of clinical examination followed by DUS examination and collection of QoL questionnaire completed by the patients. The need for secondary procedures was assessed at 6–12 weeks. If patients remained symptomatic with residual/unsightly varicosities or developed symptomatic incompetent perforators affecting QoL, treatment options were discussed and offered subsequently.
Statistical analysis
Continuous data were first tested for normality (histograms, Kolmogorov–Smirnov and Shapiro–Wilks testing). Non-normally distributed data are presented as medians (interquartile range, i.q.r.), and analysed with the Mann–Whitney U test and Wilcoxon's signed ranks test for paired data. Categorical data were analysed using the Pearsons χ2 test. P < 0.050 was considered statistically significant. Statistical analysis was performed using SPSS® version 18.0 (SPSS, Chicago, IL, USA) software.
Results
Pre- and postoperative duplex findings
On preoperative DUS evaluation, SPJ incompetence was found in all limbs, SSV reflux from junction to at least mid-calf was demonstrated in 21/23 legs in the short excision group and 26/27 legs in the extended stripping group. The remaining two and one legs, respectively, demonstrated SSV reflux in the proximal segment only. Tortuosity of the SPJ and proximal SSV was recorded in one limb each in both groups. An incompetent distal calf perforator was found in one limb of the short excision group. None of the limbs demonstrated gastrocnemius vein reflux which could be attributed to cause SSV incompetence. Postoperatively, none of the limbs in both groups demonstrated SPJ incompetence over the follow-up period. At three and 12 months SSV reflux from proximal to at least mid-calf level was demonstrated in 11 (48%) legs in the short excision group; at the mid-calf level (excluding the stripped proximal segment) in three (11%) and two (7.4%) legs in the extended stripping group respectively. The patency and reflux status as recorded in the proximal, mid and distal segments of SSV are listed in Table 2.
Duplex ultrasound findings of SSV competence pre- and postoperative

SPJ, saphenopopliteal junction; SPL, saphenopopliteal ligation; SPJ, saphenopopliteal junction
One limb each in both groups required EVLT of the incompetent SSV and ambulatory phlebectomies of the recurrent symptomatic tributaries, at 12 weeks
One further limb in the short excision group required EVLT of symptomatic SSV reflux following the one year duplex scan
Intraoperative measures
The SPJ was positively identified and ligated in all patients (100%) in both groups. There was no significant difference in procedure duration between the short excision and extended stripping groups (median [i.q.r.] 60 [55–72] versus 65 [55–78] minutes, respectively; P = 0.470). The median (i.q.r.) length of SSV removed was 0 (0–3) versus 19 (15–22) cm, respectively; P < 0.001.
Complications and recurrence
Minor complications recorded prospectively included phlebitis in one leg (3.7%) with subsequent infection at a phlebectomy site requiring antibiotic treatment, in the extended stripping group. Haematomas developed in two legs (7.4%) of the extended stripping group, which resolved completely by the six-week follow-up visit. Symptoms of sural neuropathy, predominantly numbness in the sural nerve distribution, was present in two legs (8.6%) in the short excision and four legs (14.8%) in the extended stripping groups at six weeks postoperatively. Sensory disturbance persisted up to a year in two legs (8.6%) in the short excision and one leg (3.7%) in the extended stripping groups.
Major complications in the short excision group included popliteal vein (PV) tear due to avulsion of tributary veins at the junction requiring surgical repair. One leg each in the short excision (4.3%) and extended stripping groups (3.7%) were found to have deep vein thrombosis (DVT) in the PV, at the one week duplex scan. These otherwise asymptomatic patients required warfarin anticoagulation which resolved the DVT by the three-month follow-up visit.
At three months, clinically recurrent, symptomatic varicosities were found in one leg each of both short excision (4.3%) and extended stripping groups (3.7%), requiring endovenous laser therapy (EVLT) of the intact SSV and ambulatory phlebectomies of the recurrent tributaries, respectively, as secondary procedures. At one-year follow-up one more leg in the short excision group (8.6%) was found to have symptomatic recurrence necessitating EVLT procedure.
Intergroup analysis did not show any significant difference between the groups in the rate of occurrence of complications and recurrence (P > 0.050) over the follow-up period.
Pain scores
There were no significant differences in the median (i.q.r.) pain scores between the short excision and inversion stripping groups on day 1, 3 (0.5–6.7) versus 4.4 (1.6–7.8), P = 0.223; day 3, 1.5 (0–4.9) versus 3.2 (0.7–5.7), P = 0.256; and day 7, 0.5 (0–3.5) versus 1.3 (0.4–4.7), P = 0.221, respectively, postprocedure. By day 7 pain scores had significantly improved in both groups (P < 0.050).
Return to work and normal activity
There was no significant difference between the short excision and extended stripping groups for the time taken to return to work (median [i.q.r.] 21 [14–24] versus 21 [7–28] days, respectively; P = 0.347) and normal activities (median [i.q.r.] 14 [3.5–28] versus 17.5 [6.5–31.5] days, respectively; P = 0.773), following surgery.
Venous severity scores
In both groups, there was significant improvement in the severity scores postprocedure, sustained over the follow-up period of one year (P < 0.001) (Figure 1). There was no significant difference in VCSS between the groups at three months (P = 0.357); however the scores were significantly better for the extended stripping group as compared with the short excision group at one year (median [i.q.r.] 0 versus 0 [0–1], respectively; P = 0.001).
Venous clinical severity score (VCSS) before and after saphenopopliteal ligation (SPL) with small saphenous vein (SSV) short excision (≤5 cm) or with inversion stripping (>5 cm). Horizontal lines within boxes, boxes and whiskers represent median, interquartile range, and range within 1.5 times i.q.r. below the first and above the third quartile, respectively; the open circles represent outliers and asterisks extreme outliers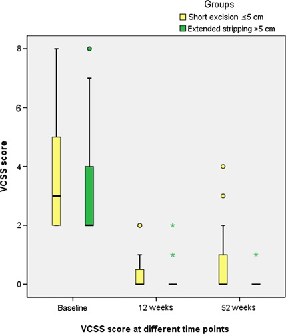
Patient satisfaction and QoL scores
At one year patient satisfaction with the overall treatment was similar in both groups with no difference between the groups (P = 0.220). However, patient satisfaction with the cosmetic appearance of the treated leg was significantly higher for the extended stripping group as compared with the short excision group (median [i.q.r.] 9.5 [8.85–10] versus 8 [7–9.75], respectively; P = 0.011) (Figure 2).
Visual analogue scores (VAS) for patient's cosmesis perception at different time points after treatment for saphenopopliteal ligation (SPL) with small saphenous vein (SSV) short excision (≤5 cm) or with inversion stripping (>5 cm). Horizontal lines within boxes, boxes and whiskers represent median, interquartile range and range within 1.5 times i.q.r. below the first and above the third quartile, respectively; the open circles represent outliers
Both groups reported significant improvement in the generic- and disease-specific QoL measures over the follow-up period (P < 0.050). However, there were no significant differences between the groups in either the SF-36® domains or the EQ-5D scores over the one-year follow-up period (P > 0.050). The disease-specific AVVQ scores were significantly better (lower scores represent better outcomes) in the extended stripping group as compared with the short excision group at three months (median [i.q.r.] 2.0 [0.51–9.24] versus 7.21 [2.51–9.8], respectively; P = 0.002) (Figure 3), and at one year (median [i.q.r.] 2 [0–3.62] versus 5.36 [1.84–12.89], respectively; P = 0.050).
Aberdeen varicose vein questionnaire (AVVQ) scores before and after saphenopopliteal ligation (SPL) with small saphenous vein (SSV) short excision (≤5 cm) or with inversion stripping (>5 cm). Horizontal lines within boxes, boxes and whiskers represent median, interquartile range, and range within 1.5 times i.q.r. below the first and above the third quartile, respectively; the open circles represent outliers and asterisks extreme outliers
Discussion
Management of small saphenous varicosities are undeniably challenging and technically demanding compared with those arising from the great saphenous venous system. Variability of the venous anatomy in the popliteal fossa and failure to locate the SPJ necessitating extensive dissection have often been attributed to the higher recurrence rate and incidence of major neurovascular injuries. 15 In addition, unlike the clear benefits demonstrated by stripping of GSV, 16 the role of stripping SSV has been controversial, with reports of increased sural nerve injury deterring surgeons from combining SPL with SSV stripping.17,18 Owing to these very reasons, there has been no randomized controlled trial undertaken to validate the clinical outcomes of SPL with or without SSV stripping.
Our study, similar to results reported by Ikponmwosa et al., 19 clearly demonstrated the usefulness of preoperative duplex marking which facilitated in positively identifying the SPJ in all 50 limbs. This is in stark contrast to some of the studies that have reported no better outcomes with preoperative duplex marking.20,21 Our results may have been influenced by the fact that the experienced vascular surgeon also held an accredited qualification in the use of ultrasound and routinely performed the preoperative duplex personally. This may have facilitated planning of the popliteal fossa exploration and to anticipate technical difficulties that may arise due to anatomical variations. Similarly formal exploration of the popliteal fossa to identify and ligate SPJ in all 50 limbs resulted in 100% technical success without increased risk of neurovascular complications, contrary to the low technical success of 59% recorded by Rashid et al., 20 who operated on 59 patients with formal SPJ dissection. Overall there were three major complications recorded in our study, two patients developed DVT which resolved completely within three months and one patient had popliteal vein tear intraoperatively requiring surgical repair with follow-up duplex scans demonstrating no compromise to venous blood flow. The preoperative duplex marking and the formal exploration of the popliteal fossa thus seems to have positively influenced the abolition of deep to superficial venous reflux at the SPJ without significantly increasing the risk of complications. Despite low postoperative morbidity, it was surprising to see both groups in this study take up to a mean duration of three weeks to return to normal functioning, even after being given written advice to resume normal activities as soon as possible. This may reflect the variability in return to activities following varicose vein surgery as reported by Darwood et al., 22 and the observation may also be encouraging to proponents of minimally invasive endovenous treatment to advocate change of practice in the management of SSV incompetence based on the slow recovery following surgery, which may be particularly disadvantageous to economically active patients.
The operative aim for all 50 limbs was to perform SPL with inversion stripping of SSV, although the extended stripping was not possible in a proportion. This may be one of the shortfalls of this study wherein the SPL short excision group was not unstripped by choice, but due to failed attempts. Whether preoperative duplex evaluation could have predicted the accomplishment of SSV stripping or not in this study is debatable as the majority of patients in both groups had refluxing incompetent SSVs up to mid-calf level or lower, thereby providing enough length of SSV to perform inversion stripping, and only one limb each in both groups had tortuous SPJ/proximal SSV segments which could be speculated to cause difficulty in passing the PS past the tortuosity without creating vein tear in these limbs. The senior author contemplates venous spasm during attempts to introduce PS or intraluminal valves restricting passage of the stripper or a combination of both as being likely causes for inversion stripping failure. The inability to strip SSV post-SPL in nearly half of the operated limbs, despite elective planning to do the same, also bears implications for considering alternative endovenous ablative treatments with reported higher rates of SSV occlusion.23–25 The rationale for planned stripping was extrapolated on the best long-term results and reduced rates of late re-operations reported in literature with GSV stripping. 26 The method of SSV stripping was standardized to inversion stripping with a PS, based on level 1 evidence demonstrating better clinical and QoL outcomes in GSV stripping with the PIN technique.27,28 Contrary to the reported morbidity associated with SSV stripping, our study showed no significant increase in sural nerve injury in comparison to the short excision group, nor was there an increased incidence due to formal exposure of popliteal fossa as discussed above. Whether these low rates of nerve injury were influenced by the use of PS, which is known to cause less perivenous trauma, is difficult to determine as there have been no randomized studies carried out comparing PIN technique to conventional stripping for SSV. 29
Akin to the results seen with SFJ ligation and GSV stripping,16,30 SPL with stripping may be expected to decrease the risk of recurrence due to removal of the SSV run-off channel into which new veins could otherwise drain. In this study the incidence of recurrence was low in both groups but this may be due to a type II statistical error associated with the small sample size.
The QoL outcomes described in this study are fascinating. There was significant improvement in both the generic- and disease-specific QoL measures up to one year in both groups establishing the effectiveness of SPL with or without stripping in the treatment of SSV incompetence. The significantly better disease-specific AVVQ scores in the extended stripping group at three months and at one year in the context of the lack of significant difference in the generic QoL domains between the groups indicates that the observed difference in AVVQ scores were specifically due to improvement in venous symptoms post-SSV stripping. Similarly intergroup analysis on patient satisfaction favoured SSV stripping to effect significantly higher scores in comparison to the short excision group at one year. This subjective evaluation complemented by objective clinician assessment of venous severity at one year which also showed significantly better scores in favour of SSV stripping adds credence to the management of SSV incompetence with SPL and extended stripping. These relative differences in favour of extended stripping may have been masked in the earlier months post-treatment due to equally high technical success with low rates of complication and recurrence in both groups, resulting in equally high patient satisfaction and QoL outcomes. The residual varicosities as a result of leaving SSV in situ may have contributed to the comparatively lesser cosmetic satisfaction and inferior disease-specific QoL benefits in the short excision group at one year.
Conclusion
SPL either with or without extended stripping of SSV is an effective treatment for varicose veins arising from the small saphenous system. Both achieve clinical and QoL improvement up to 12 months. Early outcomes favour SPL with stripping to offer greater improvement in venous severity, cosmesis and disease-specific QoL, without evidence of increased complications. Hence our practice will continue to remain SPL with extended stripping when possible, complemented by preoperative duplex marking and formal exposure of the popliteal fossa. Although the study did not show increased short-term recurrence without stripping of SSV, greater numbers and follow-up are required to make firm conclusions. Further randomized controlled trials are also required to compare ablative procedures (chemical and thermal) and stripping in the SSV system.