
Abstract
Objective
The aim of this retrospective study was to assess the long-term results of stripping the insufficient great saphenous vein (GSV) with stump coagulation, closure of the cribriform fascia and some additional measures, which will be described in detail.
Methods
Patients treated from 1998 to 1999 for varicose veins had been invited in 2009 for follow-up colour-coded duplex sonography and had been asked to answer a quality-of-life questionnaire. In 2009, the examinations for the study were conducted at a clinic of angiology by an independent and experienced sonographer.
Results
From a total of 165 patients, 91 (136 limbs) had been willing to participate in the study. Duplex ultrasound after a mean follow-up of 10.7 years revealed only clinically non-relevant (Ø < 0.3 cm) neovascularizations in 1.5% of all treated legs. No clinical relevant varicosities from the groin had developed.
Conclusion
The crossectomy combined with stump coagulation and suture of the fossa ovalis, completed with some additional measures, is a successful method to reduce neovascularization and recurrent varicosities, even for redo-crossectomies, without increasing the risk of perioperative complications.
Keywords
Introduction
The standard surgical treatment for great saphenous vein (GSV) insufficiency includes disconnection of the saphenofemoral junction (SFJ) and stripping of the vein. Recurrence of varicosities remains a major problem with the method and has been reported to be as high as 20–60%.1–4 Neovascularization with re-connection of the venous channels at the SFJ after crossectomy is one of the main causes of recurrence. 5 Several factors are discussed as causes for neovascularization: hypoxia, various growth factors, such as vascular endothelial growth factor, vascularization of the haematoma, scar-vascularization, free endothelial cells and high venous blood pressure.6–10 Still, the pathogenesis of neovascularization is not yet clearly understood. To prevent recurrence at the level of the SFJ, various surgical techniques have been investigated, with differing results: modified crossectomy without SFJ dissection, 11 resection of the SFJ with direct suture of the femoral vein, over-sewing the ‘stump’, electrocoagulation of the ‘stump’, 12 leaving a long ‘stump’ or barrier techniques such as closure of the fossa ovalis or patch plastics with various materials.13–20 Few of the mentioned methods to prevent neovascularization showed some success, and, despite some significant reduction, the neovasculogenic response remains high and takes place even after endovenous techniques with laser or radiofrequency.21,22
We report the 10-year results of a combined surgical technique with electrocoagulation of the GSV-stump as well as of all ligated tributaries, closure of the cribriform fascia and some additional measures, which are particularized. The procedure was introduced into clinical practice by the phlebologist (SG) and the vascular surgeon (SS) in 1998.
Patients and methods
Demographics, including risk factors for varicose veins and thromboembolism, and history of previous treatment for varicose veins and CEAP (clinical, aetiological, anatomical and pathological elements) classification were noted. All patients with GSV insufficiency and truncal incompetence at the SFJ (documented by preoperative duplex examination), operated between April 1998 and June 1999 using the combination of coagulation of the ligated GSV and tributaries and closure of the cribriform fascia had been contacted by the surgeon in 2009. Patients willing to participate in the study received written information regarding the study and gave informed consent for the trial, which was approved by the Ethics Committee of Zurich, Switzerland.
Between April 1998 and June 1999, a total of 165 patients had been operated by the described combined technique for varicose veins. Follow-up was not possible in 74 patients; five died, 37 were not reachable and 32 patients were not willing to participate in the study. Eleven of them mentioned having no time for a visit but were satisfied with the result, two patients refused participation and were not satisfied. Baseline characteristics of the 91 patients (136 limbs) willing to participate in the study are given in Table 1. In 63 patients with primary varicose veins, 90 crossectomies had been performed and 32 patients had been treated for recurrent varicosis (46 legs). Four patients had a primary crossectomy on one and a re-crossectomy on the other side. Six patients had one, and one patient had two further operations within the 10-year period for new developments of varicose veins. None of the additional operations had to be done at the primary operation site.
Patient characteristics (n = 91)
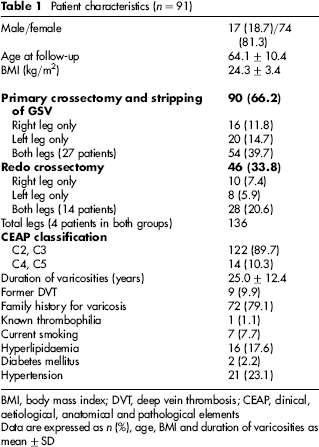
BMI, body mass index; DVT, deep vein thrombosis; CEAP, clinical, aetiological, anatomical and pathological elements
Data are expressed as n (%), age, BMI and duration of varicosities as mean±SD
Surgical technique
Double-ligation of the GSV at the level of the common femoral vein (Polysorb 0) and ligation of all tributaries as distally as possible (Polysorb 2-0). The entire wall of the remnant of the GSV of about 1 cm is coagulated intermittently with monopolar electrocoagulation to shrink the remnant to about 0.5 cm (Figure 1), followed by the same procedure for all tributaries. Anterior accessory veins are stripped whenever possible or removed as far as possible from the groin incision. It is possible to remove these veins over quite a long distance. Posterior accessory veins are ligated as distal as possible or even stripped in selective cases. Pudendal tributaries are ligated separately. The lamina cribriformis is closed with a 2-0 Polysorb Z – suture. The GSV is mobilized as far as possible with flexion of the hip articulation. Most of the time we mobilize the GSV about 10 cm. Thus we can ligate or coagulate further side branches. The GSV is stripped at least to below the knee in Esmarch ischaemia. Eventual further saphenous veins (double GSV) are stripped in the same manner. In recurrent vein crossectomy, the classical approach was chosen via oblique incision 1 cm above the inguinal skin crease. In case of relevant cicatrizations, the femoral artery is prepared first before dissecting the common femoral vein.
(a) ‘Stump’ before intermittent coagulation. (b) ‘Stump’ after intermittent coagulation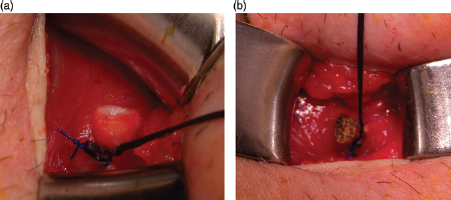
All limbs were treated with phlebectomy of tributaries and ligation of perforating veins (average 5.8 per limb). In 42 limbs, a short saphenous vein was treated additionally, of which 11 limbs showed a recurrence. In three limbs, we ligated an isolated insufficient medial gastrognemic vein, and in one limb, we resected an ischiatic vein. A drainage of the Redon-type is rarely used. After the operation, which is done in general or spinal anaesthesia, we bandage the leg with elastic bandages with gauze-compression on the GSV-canal for about 24 hours. We put a sandbag on the groin incision for about two hours after the operation. Low-molecular-weight heparin is administered once daily in a prophylactic dose for 10 days postoperatively.
Follow-up
Colour-coded duplex ultrasound (CCDS) assessment was performed by a single experienced and independent sonographer (FM) using a Philips iU22 (Philips Medical Systems, Best, The Netherlands) with a linear 4–8 MHz linear array probe with colour and spectral Doppler modalities. 23 Pathological reflux was defined as flow reversal for more than 0.5 seconds after the manometer controlled Valsalva manoeuvre with the patient in a standing position. To detect groin tributaries, the region of the previous SFJ was examined accurately for new connecting veins. Repeated Valsalva manoeuvres were used to detect retrograde flow. Tiny vessels with a diameter ≤3 mm without reflux were classified as not relevant. Relevant neovascularization was defined by a refluxing vein with a diameter >3 mm. Veins in the groin, which are not connected with the common femoral vein, originating mainly from the ligated epigastric vein and from lymphnodes, were not analysed, because it is almost impossible to distinguish between residual veins and neovascularizations in this area. Patients were asked about ‘severe postoperative pain’ (yes/no), ‘satisfaction 10 years after operation’ on a scale from 1 to 6 (1: very bad, 6: excellent result) and if they ‘would undergo surgery again’ (yes/no). Clinical findings were documented as recurrent or residual varicosis of the GSV, tributaries, reticular varicose veins and telangiectasias (Table 2).
Results: 10-year follow-up of 136 legs (91 patients)
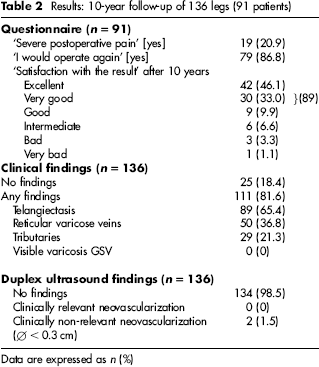
Data are expressed as n (%)
Results
The most frequent clinical findings were telangiectasias in 65.4%, followed by reticular varicose veins in 36.8% and tributaries in only 29 legs (21.3%) (Table 2). The satisfaction with the result was good to excellent in 89% of the patients after 10 years and 87% would do the operation again. CCDS documented no residual GSV-stump and no clinical relevant neovascularization in the groin had been found. Only two patients showed clinical non-relevant neovascularization (Ø < 0.3 cm) at the SFJ; one of them had initially been treated for recurrent varicosis. We had one postoperative haematoma, which had to be evacuated, and one postoperative wound infection in the groin. No lymphatic leaks, no deep vein thrombosis and no pulmonary embolism (PE).
Discussion
Recurrent varicosis at the SFJ after conventional crossectomy with stripping of the GSV is a relevant problem in up to 60% of the patients after standard surgical treatment for GSV insufficiency. Neovascularization is one of the main risk factors for recurrences and many different approaches to reduce it have been tried with little success 1 , e.g. resection of the GSV-junction with direct suture of the common femoral vein, ligation of the GSV with non-resorbable materials like Prolen or Mersilen, over-sewing of the GSV-stump or leaving a long saphenous stump, barrier techniques with suture of the cribriform fascia or covering of the saphenous opening with PTFE-, Dacron- or Silicon-patch, or raising a flap of fascia.1,12,17,19,20,24–29 Some of those techniques resulted in either short- or long-term complications, especially when foreign material was used. 26 A reduction of neovascularizations of more than 50% with the suture of the cribriform fascia had been published by three different groups.30–32 Also haematoma formation is discussed to promote neovascularization; therefore, it is important to avoid haematoma in the groin and in the stripping canal. 9 In 2005, Hartmann 27 reported a reduction of neovascularization from 20.7% to 7.9% with coagulation of the GSV stump only. In order to further reduce neovascularization the combination of GSV-stump coagulation and suture of the cribriform fascia had been introduced in 1998 by Gabler and Schnyder. The combination of these methods is easy to perform and the suture of the fossa ovalis needs less than one minute. Furthermore, electrocoagulation can easily be used at the sapheno–popliteal junction as well, where other methods appear impossible to perform. Also, if in the future a redo crossectomy would become necessary, there would not be more difficulties compared with a redo crossectomy after a classic crossectomy. Since 1998, the first author had applied this method in over 2500 crossectomies without method-related complications. The results after 10 years in 91 patients were even better than expected with no clinical relevant neovascularization at all and in only two patients small (Ø < 0.3 cm) incompetent veins at the SFJ had been identified by CCDS. Even in patients with crossectomy for recurrent varicose veins, no clinically relevant recurrences had been found by clinical and CCDS examination, in contrast to the results of De Maeseneer 26 observing neovascular vessels (Ø ≥ 0.4 cm) in 45% without and in 9% with silicon patch five years after re-intervention. These excellent results might be due to the combination of several factors: coagulation of the wall of the GSV remnant and of all tributaries, resection of all tributaries as distal as possible, stripping of the GSV and of eventual additional GSV 26 as well as of anterior and/or posterior accessory veins, suture of the cribriform fascia and avoiding haematoma close to the GSV stump by meticulous haemostasis. Further measures to avoid haematoma formation were stripping in Esmarch ischaemia, compression of the stripping canal and of the groin incision postoperatively. 9 It is not clear how much any of these measures contributed to the reduction of neovascularization.
Fortunately, after more than 10 years, the follow-up examination was possible in 55% of patients operated between 1998 and 1999. The possibility that a few patients declined to give informed consent because of dissatisfaction with the postoperative result cannot be ruled out. However, long-term follow-up studies are known to be associated with a lower follow-up rate of about 50%.28,29,33
Conclusion
The crossectomy combined with stump coagulation and suture of the fossa ovalis is a successful method to reduce neovascularization without increasing the risk of perioperative complications. The good results underline that surgery for GSV-varicosis with the described technique should be added to the classic crossectomy for primary as well as for recurrent varicosis of the GSV. Furthermore, considering the simplicity of the surgical technique and the excellent outcome of this study, it is questionable if it is scientifically justified to perform a randomized trial on this subject, above all in comparison with the results of other published procedures. Our retrospective study might nevertheless give input to initiate further studies.