
Abstract
The objective of the study is to evaluate the viscosity of popular sclerosants and their flow hydrodynamics through a syringe/needle to further discuss Miyake's old, venous-capillary reflux theory, using additional objective data. The following sclerosing agents were tested in the study: 75% dextrose (D75%); 50% dextrose (D50%); 5% ethanolamine oleate (Etha5%); 0.5% laureth-9 (Aet0.5%) and 0.1% sodium tetradecyl sulphate (STS0.1%). Using 5 mL syringes and 27G needles, the resulting pressures and flows for each sclerosant agent were measured. To do this, a three-way stopcock was connected between the syringe and the needle so that an arm of the stopcock could be used to measure injection pressures with a digital monitor in 1 mmHg increments. Two trials were performed: in trial 1, the syringe was attached to a Samtronic 680 infusion pump and in trial 2, the solutions were injected manually. The observed sclerosant viscosities were as follows: D75%: 0.28 Poise; D50%: 0.12 Poise; Etha5%: 0.10 Poise; Aet0.5%: 0.07 Poise; and STS0.1%: 0.04 Poise. In trial 1 (constant flow), it was observed that D75%, which had the highest viscosity of the sclerosants tested, had the highest pressure readings. In trial 2 (constant pressure), the flow obtained with the D75% solution was lower than the flow of the other solutions. In conclusion, based on the rabbit study theory, vessel size and sclerosant viscosity and strength, not extravasation, play a role in causing ulceration from injection sclerotherapy. As a result, they all affect the potential of venous–capillary reflux being caused by sclerotherapy injection and, thus, the risk of postsclerotherapeutic cutaneous ulceration.
Background
Ulceration, or cutaneous necrosis, during sclerotherapy of telangiectasias invariably presents a greater problem than the telangiectasias themselves. For many years, the most widely accepted theory concerning the cause of postsclerotherapy ulceration was perivenous injection of sclerosant, or extravasation. In 2001, Bihari and Magyar questioned whether this long-held theory was accurate or not, since even a small amount of extravasation can cause a large skin wheal without producing any long-term skin damage. Furthermore, ulceration clearly occurs without sclerosant extravasation when telangiectasias are sclerosed. 1 The belief of Bihari and Magyar was that occlusion of the feeding artery was a more likely cause of skin necrosis; they further hypothesized that an arteriovenous shunt was likely to be the responsible mechanism. In further support of their theory, Goldman 2 has found thrombosis in the feeding artery. We concur with Bihari and Magyar's ischaemic necrosis theory: postsclerotherapy skin ulcers are painful and generally have a very lengthy evolution. Still, the question remains: how does the sclerosant reach arteriolar branches and thrombose them?
One hypothesis, proposed by Miyake, 3 is that the occlusion is caused by venous–capillary reflux of the sclerosant solution, when the flow capability of the punctured vessel is exceeded.
As viscosity and pressure influence sclerosing agent flow, we decided to design this in vitro study examining the inter-relationship of injection pressure, flow rate and viscosity of different sclerosing agents.
Objective
The objective of this study is to evaluate the viscosity of popular sclerosants and their flow hydrodynamics through a syringe/needle to further discuss Miyake's old, never-published-in-English venous–capillary reflux theory, using additional objective data.
Materials and Methods
Measurement of viscosity
Some of the most common sclerosing agents2–6 were tested at the Air Pollution Laboratory of the Faculdade de Medicina da Universidade de São Paulo. Vials containing 3 mL of each sclerosing agent were measured at CAP 2000 Viscometer.
The viscosities were measured in Poise (the Poise is the unit of dynamic viscosity in the centimetre gram second system of units. It is named after Jean Louis Marie Poiseuille). The temperature used was 24°C for viscosity measurement (see Table 1).
Sclerosant viscosity: Poise (P)

The agents tested were as follows:
75% dextrose (D75%); 50% dextrose (D50%); 5% ethanolamine oleate 5% (Ethamolin®, Zest Pharmaceuticals, Rio de Janeiro, Brazil) (Etha5%); 0.5% Laureth-9 (Aethoxysklerol®, Teuto Laboratories, Anapolis, Brazil) (Aet0.5%); 0.1% sodium tetradecyl sulphate (Sotradecol®, AngioDynamics, Queensbury, NY, USA) (STS0.1%).
Measurement of pressure and flow
Five mL syringes (Terumo®) and 27G needles (Terumo®, Terumo Europe NV, Leuven, Belgium 27G-1/2) were used. All syringes, needles and other materials were new and sterile. Measurements were made in the operating room of Hospital Alemão Oswaldo Cruz in 1997 at room temperature. Temperature is kept between 22 and 24°C. The resulting pressures and flows for each sclerosant agent were measured. To do this, a three-way stopcock was connected between the syringe and the needle so that an arm of the stopcock could be used to measure injection pressures with a Hewlett Packard (Palo Alto, CA, USA) HP Merlin CMS System M1175/76A digital monitor in 1 mmHg increments (see Figure 1).
INFUSION PUMP 680 – Devices and connections: analysis of pressure at a constant flow
Two trials were performed:
In trial 1, the syringe was attached to a Samtronic (Samtronic, Socorro, Brazil) 680 infusion pump. The flow rate of the injection bolus for the different sclerosant solutions was kept constant at 0.39 mL/second. Pressure values were monitored and recorded after stable for more than two seconds.
In trial 2, the solutions were injected manually, so that a constant pressure was maintained at about 100 mmHg and the corresponding flow rate for each solution was obtained.
All injections were into open air so that they were free of resistance. Measurements were, therefore, obtained in the absence of organic tissue or hydraulic pressure against the needles.
Results
Sclerosant viscosities were as follows:
D75%: 0.28 Poise; D50%: 0.12 Poise; Etha5%: 0.10 Poise; Aet0.5%: 0.07 Poise; STS0.1%: 0.04 Poise.
In trial 1 (constant flow), it was observed that D75%, which had the highest viscosity of the sclerosants tested, had the highest pressure readings. The STS0.1%, which had the lowest viscosity, had the lowest pressure readings (see Table 2).
Analysis of pressure values obtained from the injection of different sclerosing solutions at a constant flow (0.39 mL/second), using a 5 mL syringe and a 27G needle
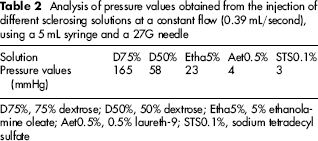
D75%, 75% dextrose; D50%, 50% dextrose; Etha5%, 5% ethanolamine oleate; Aet0.5%, 0.5% laureth-9; STS0.1%, sodium tetradecyl sulfate
In trial 2 (constant pressure), the flow obtained with the D75% solution was lower than the flow of the other solutions. The highest flow was recorded with STS0.1% solution (see Table 3).
Analysis of the flow values obtained from the injection of different sclerosing solutions at a constant pressure, using a 5 mL syringe and a 27G needle
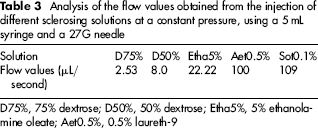
D75%, 75% dextrose; D50%, 50% dextrose; Etha5%, 5% ethanolamine oleate; Aet0.5%, 0.5% laureth-9
Discussion
Discussion of our in vitro study
Simply by injecting different viscosity sclerosing agents, it is easy to tell that less effort is needed to inject Aet0.5% or STS0.9% compared with D75% in open air or during a sclerotherapy session. But the physician's feeling is subjective information. The aim of this study was to find more objective data about pressure, flow and viscosity. For instance, the measurement of pressure needed to inject the same volume of different viscosity sclerosing agents can help in discussion of the existing literature about postsclerotherapy ulcers.
The trial 1 measurement was precise and consistent because the infusion pump kept a constant flow. Measurements were digitally recorded and kept stable throughout the procedure. Flow, syringe, needle, pressure monitor and connectors were all the same. The only variable was sclerosing agents with different viscosities. Even though all injections were made in open air, the difference of pressure values corroborate with the physician's feeling that more pressure in the thumb is needed to inject at the same flow dextrose when comparing to STS0.9%, for instance.
In trial 2, on the other hand, the data obtained did not have the same consistency as in trial 1 because an infusion pump could not be used. Furthermore, as there was a great difference between viscosities, the difference in flow was up to 40 times higher with less viscous sclerosants. Any practitioner performing sclerotherapy might easily notice such a difference. The objective in trial 2 was only to exemplify the resulting difference in flow using sclerosants with different viscosities, even when the same manual (thumb) pressure was exerted on the syringe plunger. It would be interesting to design a study measuring the pressure during sclerotherapy in different scenarios if a less cumbersome pressure measuring system is available. Maybe the ideal equipment would be a syringe with a coupled digital pressure sensor.
The authors did not evaluate whether the sclerosing agents were Newtonian fluids or not and/or if there could be a viscosity change due to pressure variations, but the aim of the study was to evaluate the pressure versus sclerosing agent.
Discussion of the reviewed literature
We agree with the opinion of Bihari and Magyar, 1 Goldman1,4 and others 7 that cutaneous necrosis is not the result of an inadvertent intradermal or subcutaneous extravascular injection. It is, rather, an ischaemic phenomenon. We believe, though, corroborating with Hiroshi Miyake, that sclerosants become arterialized in a different way from that which has been hypothesized by others.
The work of Bihari and Magyar is very important because they compiled a series of related studies on the matter. Unfortunately, Hiroshi Miyake's rabbit study was not available in English and was not therefore included in their analysis nor in their study design. Although we completely agree that imaging studies could help clarify the involved pathophysiology, the Doppler used by Bihari and Magyar was non-specific. Small arterioles are normally present under the skin and are detectable with a Doppler. These normal arterioles could be misinterpreted as arteriovenous shunts. The same Doppler evaluation could be repeated in areas free of telangiectasias to re-evaluate some of their conclusions.
Despite the findings of Bihari, Magyar, Goldman and others, a 2007 review article on the complications of sclerotherapy by Munavalli and Weiss 7 stated that ‘the most common cause’ of necrosis ‘is the extravasation of sclerosants into perivascular tissue’. More recently, however, Schuller-Petrović et al. 8 examined the experimental potential of liquid and foamed polidocanol in causing skin necrosis, when injected into the superficial subcutaneous tissue of rats. Their findings conclusively showed that quantities of up to 0.5 mL of 0.5% polidocanol, as either a liquid or foam, do not induce visible skin necrosis. 8
Below is the translation of Hiroshi Miyake's original study to help discuss postsclerotherapy skin ulcer pathophysiology. In his original experimental study, Miyake based his venous–capillary sclerosant reflux argument on three points:
Necrosis was found even when there was no extravasation of sclerosant solution into the extravascular space; The behaviour and development of postsclerotherapy necrosis was similar to ischaemic ulcers caused by arterial occlusion, both in terms of pain and length of time of ulcer evolution; The greater the strength of a given sclerotherapeutic agent, the greater the probability of ulceration.
In 1972, Miyake tested his theories by studying extravenous injection of sclerosant and intravenous injection, with its resultant occlusion of feeding arterioles, in a total of 25 mixed breed (New Zealand and Giant White) rabbits. The rabbits were divided into two groups:
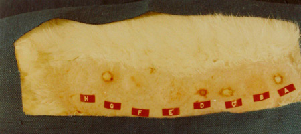
Group 1: injection into rabbit torso. In group 1A, six rabbits received intradermal injections of 0.5 mL of the eight listed solutions (see Figures 2 and 3). In group 1B, the same procedure was repeated in six other rabbits with 0.5 mL of the solutions being injected subcutaneously. In each, the solutions were injected at approximately 2 cm intervals along an imaginary longitudinal line.
Intradermic injection rabbit torso: 10 minutes after injection – the papules formed by the injection of sclerosing substances increased rapidly in size reaching a confluence with the other. Note the appearance of skin necrosis on A, C, D, E, F and G Intradermic injection rabbit ear: 24 hours after injection. The necrosis evidence in various sizes in all local sites injected, except on H

The tested sclerosing agents are listed below:
5% ethanolamine oleate; 0.5% Laureth-9 (Aethoxysklerol); Sodium morrhuate; Sodium silicate 30%; Sodium chloride 20%; Dextrose 50% + 5% ethanolamine oleate (proportion of 10:1); Sodium tetradecyl sulfate 0.1%; Sodium chloride 0.9%.
Even though a large amount of sclerosant was injected into the tissue outside the vein, there was no evidence of skin necrosis in any of the injected rabbits in either group. Furthermore, the volume of extravasated sclerosant was larger than would go unnoticed, considering the fact that 0.1 mL of sclerosant is enough to cause a visible papule.
Group 2: injection into rabbit ear veins. A commonly used sclerosing agent (dextrose 50% + ethanolamine 5% [proportion 10:1], which was commonly used in Brazil in the 1970s) was injected into two different sized veins at three different pressures (300, 500 and 700 mmHg). In group 2A, veins up to 0.4 mm in diameter were injected in different locations at all three pressures. In group 2B, veins larger than 0.8 mm in diameter were only injected at 700 mmHg pressure. A pressure of 700 mm was chosen in an attempt to ensure that the flow of the injectant would exceed venous outflow and, therefore, increase the chance of causing an ulcer. A maximum volume of 0.5 mL was used for each injection (see Table 4).
Correlation between injection pressure and size and frequency of lesions

Group A: veins up to 0.4 mm in diameter. Group B: veins larger than 0.8 mm in diameter
Size of lesions: +, 0–2 mm; ++, 2–4 mm; +++, 4–8 mm; and ++++, >8 mm
Sclerosant used for all injections: dextrose 50% + ethanolamine 5% (proportion 10:1)
The results in group 2A (smaller vessels) showed that at 300 mmHg pressure there was no necrosis at all. At pressures of 500 and 700 mmHg, necroses occurred only with the detergent sclerosants, but not with hypertonic dextrose (see Figures 4 and 5).
Intravenous injection rabbit ear: necrosis aspect 10 minutes after injection of 0.5 mL of dextrose 50% + 5% ethanolamine oleate at 500 mmHg pressure in 0.4 mm vein diameter. The pallor of the area corresponding to the drainage vein was noted. There was reactive hyperaemia, oedema and intense cyanosis Intravenous injection rabbit ear: necrosis aspect 24 hours after injection of 0.5 mL of dextrose 50% + 5% ethanolamine oleate at 500 mmHg pressure in 0.4 mm vein diameter. Same as Figure 4
In group 2B (larger vessels) there was no necrosis, even with injection pressures of 700 mmHg.
The results would seem to indicate that the size of the necrotic area, after injection into the rabbit ear blood vessels, was dependent on:
The pressure of injection: the higher the pressure, the greater the likelihood of an ulcer and also the greater the size of the ulcer; The diameter of the punctured vessel: the smaller the vessel, the higher the probability of ulcer.
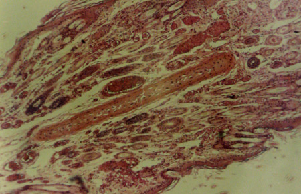
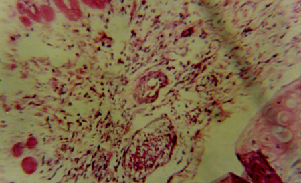
In the same study, after sclerotherapy-induced skin ulceration was reproduced, all necrosis-producing procedures were repeated with China ink added to the sclerosant solution. On histological examination eight hours later, China ink was detected in venules, capillaries and more importantly, arterioles. The histopathology of the biopsied ulcerations also appeared to be consistent with ischaemia. Thus, histological examination made it clear that capillary thrombosis was related to the ischaemic aetiology of the ulcers (see Figures 6 and 7). It is important to remember that the most powerful sclerosants are the detergents. They are also the least viscous. Lower viscosity means higher outflow. Thus, when a detergent sclerosant is injected into smaller vessels, where venous–capillary reflux is more likely to occur, there is an increased chance of a sclerosant reaching arterioles and producing skin necrosis. Figures 8–10 show the histology of the thromboses and ulcerations.
Biopsy of rabbit ear, immediately after injection of dextrose 50% + 5% ethanolamine oleate (proportion of 10:1). China ink is seen inside capillaries. Staining: haematoxylin–eosin,×100 Biopsy of rabbit ear, eight hours after injection of dextrose 50% + 5% ethanolamine oleate (proportion of 10:1). Muscular tunic necrosis was noted. Staining: WvG (Weigert von Gieson staining), ×400 Biopsy of rabbit ear, two hours after dextrose 50% + 5% ethanolamine oleate injection. The appearance of normal interstitial tissue – note the numerous vessels, capillaries, venules and arterioles of light dilated and congested Biopsy of rabbit ear, eight hours after dextrose 50% + 5% ethanolamine oleate injection. The arteriole is seen with necrosis of muscular tunic, subendothelial oedema and inflammatory infiltration Biopsy of rabbit ear, 48 hours after dextrose 50% + 5% ethanolamine oleate injection. There is necrosis of the wall of arterioles, veins and dilated capillaries containing the light in early thrombus organization

If the sclerosing agent reaches the arteriole, it can cause sclerosis or simply cause a veno-arteriolar reflex vasospasm. Regardless of what can happen, the pathophysiology is ischaemic.
In analysing the rabbit study, necrosis could not be produced when the sclerosing agent was injected into larger veins. This result is probably due to the higher outflow volume and lower outflow pressure of larger veins. The fact that the necrosis was reproduced with the use of detergents, which allow for the use of smaller needles in smaller veins, also corroborates the reflux theory. Consequently, patients with the smallest veins are more likely to develop skin ulcers from injection sclerotherapy since smaller veins, which have lower outflow volume and higher outflow pressure, would be more likely to cause venous–capillary reflux. It seems ironic that, in a sense, the more the cosmetic concern over small veins, the more the risk of an even greater cosmetic concern with cutaneous necrosis.
Based on the conclusions of the rabbit study, the present study was directed toward three factors:
The determination of the viscosity of several common sclerosants; The influence of the resulting flow of the sclerosant on the telangiectasia; The resistance caused when injecting the syringe bolus.
Analysis of the results leads to the conclusion that, in clinical practice, for the operator to be able to inject solutions in a vessel and maintain a constant flow rate, s/he would have to exert a pressure on the syringe plunger that would be proportional to the sclerosant viscosity and would be much higher with higher viscosity solutions. In the same manner, exerting the same pressure when injecting different solutions, s/he would inject at a higher flow rate with lower viscosity sclerosants.
It is important to remember that the pressure of an intravascular injection is inversely proportional to the diameter of the syringe. Knowing that pressure (P) equals the quotient of the force (F) exerted perpendicularly on to an area (A) at which it is applied (P = F/A), we see that when the same force is applied, syringes with smaller diameters create higher pressures.
The importance of the above concepts becomes even more evident when considering the rabbit study. Hiroshi Miyake hypothesized that an ischaemic aetiology of cutaneous necrosis could result from venous–capillary reflux of an injected sclerosant, when the flow capacity of the punctured vessel was exceeded. Such a situation could easily occur with less viscous solutions. It is worth remembering that substances like ethanolamine oleate, aethoxyskerol and sodium tetradecyl sulphate, besides being less viscous, are also stronger sclerosants that may potentiate harmful tissue effects. The clinical application of these findings would be the recommendation that, for beginning sclerotherapy practitioners, it might be advisable that they use substances that are more viscous and that are delivered in a 5 mL syringe, rather than in a 1 or 3 mL syringe. It would also be advisable to inject with low pressure and avoid sclerosing tiny telangiectasias.
Viscosity measurements, trial 1 and trial 2 demonstrated, in an objective way, what could be inferred from the rabbit study. According to Poiseuille's law, pressure decreases proportionally as viscosity increases and, therefore, the risk of cutaneous necrosis is lower when using sclerosants with higher viscosities.
After the conclusion of the rabbit study in 1972, Hiroshi Miyake reported that he has no longer used anything but 75% dextrose for sclerotherapy. If the desired results are not achieved, phlebectomy of feeder veins is performed. Since then, he has reported that the incidence of significant cutaneous necrosis caused by sclerotherapy has plummeted. Dextrose can cause minor skin necrosis with extravasation; however, when this occurs, it causes a superficial 1–2 mm scar that heals in one or two weeks. The behaviour of a dextrose scar is completely different from that of cutaneous necrosis caused by ischaemia. 9
We believe that the correlation between outflow capacity of the injected vein and the injection pressure is key to understanding and, therefore, avoiding cutaneous necrosis resulting from sclerotherapy.
Based on the rabbit study theory, vessel size and sclerosant viscosity and strength, not extravasation, play a role in causing ulceration from injection sclerotherapy.
Conclusions
Sclerosant viscosity and injection pressure can change the flow dynamics of the sclerotherapy procedure. As a result, lower viscosity sclerosing agents are easier to inject in a higher volume. A high flow according to the reviewed literature can increase the risk of postsclerotherapy cutaneous ulceration by venous–capillary reflux.
Footnotes
Acknowledgements
The authors acknowledge Air Pollution Laboratory staff of the Faculdade de Medicina da Universidade de São Paulo. The authors thank vascular surgeons Paulo Guimarães (MD PhD), Ronald Fidelis (MD PhD) and Camila Oba (MD), who contributed to the viscosity and pressure analysis; and also Jeff Hsu (MD), who helped with discussion and concepts.