
Abstract
Introduction
Chronic venous disease (CVD) is a common disease all over the world, mainly in Western Europe and the USA.
Aim
To evaluate the prevalence of CVD in the Greek general population and the characteristics of CVD.
Materials and methods
The study sample included 1500 individuals, 15–64 years of age, who were citizens of Athens, Thessaloniki, or one of five Greek cities with more than 10,000 in the population. The sample was selected by a stratified, multistage, random sampling procedure based on the Greek Census 2001. Questionnaires were completed for each individual by personal interview.
Results
From 1500 individuals, 224 (14.9%) had symptoms and/or signs of CVD, 9.6% were men and 20.1% were women. The highest percentage of presenting CVD symptoms was among 45–54-year-olds (23.4%) and 55–64-year-olds (27%). The symptoms that were mostly mentioned among sufferers were 58% achy legs, 37.4% swollen legs and 25.3% heavy legs, whereas the frequent signs were broken capillaries – telangiectasia (19.2%) and varicose veins (14.8%). About 62.9% with CVD had an obese body mass index (BMI > 25). The prevalence of CVD in patients with prolonged standing hours at work (4+ hours) was 20.8%. The symptoms of CVD were worse during the summer period only in 26.8% of the patients whereas in 50.8% during all the year. Regarding quality of life, more than 40% of the patients had either health or cosmetic problems. Sufferers mentioned that they took first advice from physicians (28%), or from friends and relatives (27%) or from pharmacists (26%).
Conclusion
This is a real whole-population study of Greece – a Mediterranean country that provides important and remarkable data on the epidemiology of CVD and highlights that we need improvement of relations within the triangle constituted by physicians, patients and disease.
Introduction
Chronic venous disease (CVD) is a common disease all over the world, mainly in Western Europe and the USA.1–4 CVD is characterized by symptoms or signs produced by venous hypertension as a result of structural or functional abnormalities of veins. Symptoms may include aching, heaviness, leg-tiredness, cramps, itching, sensations of burning, swelling, restless leg syndrome, dilation or prominence of superficial veins and skin changes. Signs may include telangiectasia, reticular or varicose veins, oedema and skin changes such as pigmentation, lipodermatosclerosis, eczema and ulceration. The term chronic venous insufficiency (CVI) describes a condition that affects the venous system of the lower extremities with venous hypertension causing various pathologies including pain, swelling, oedema, skin changes and ulcerations. 5 CVI is classified according to the CEAP (clinical, aetiological, anatomical and pathological elements) classification. 6
There are different risk factors that could help the development of CVD, such as age, sex, obesity, pregnancy, the way of everyday life (sitting and/or standing position), etc. The treatment of CVD is either mainly conservative and/or surgical. 7
The aim of this study was to evaluate the prevalence of chronic venous disease in the Greek general population and the characteristics of chronic venous diseases: who presents with chronic venous insufficiency, their symptoms, the relation between symptoms and risk factors of chronic venous disease, if the patients are aware of their disease, from whom the patients take advice about their disease, which treatments the patients follow and if the patients are satisfied with that treatment.
Materials and methods
Study population
The data analysed in this study were collected during a survey carried out in Greece during the period 21 October 2010 to 8 November 2010. Participants were selected from Greek citizens of Athens, Thessaloniki or other cities of Greece with >10,000 populations with the following inclusion characteristics: (i) man or woman aged between 18 and 65 years and (ii) citizen of Greece. We studied a sample of 1500 persons from what was estimated to be approximately 4,531,000 persons according to the 2001 National Census.
Survey methods
The survey was carried out with the assistance of a specialized market research company (QED, Athens, Greece). The participants were chosen randomly and the sample was defined with the use of a multistage, proportional, random sampling method. In particular, the sample was based on data derived from the 2001 Greek Census demographic benchmarks and the household distribution according to the National Statistical Service, and it was balanced according to the proportions of the Greek population stratified by sex, age and geographical distribution. The study protocol was designed and reviewed by the Hellenic Society of Primary Health Care Research and Continuing Education Bioethical Committee. The survey was conducted in agreement with the version of the Declaration of Helsinki and in keeping with local regulations. The survey was carried out by nurses who were trained specially to conduct the survey. Nurses questioned, recorded the answers and made a physical examination of the person. Participants, in order to arrange the face-to-face interview, were contacted in advance by random-digit telephone dialling and asked to participate in a survey concerning personal health-related issues. One adult was interviewed per household, the one whose birthday fell earliest after the telephone contact date. If that person was unavailable, the adult with the next closest birthday was requested. Up to 10 call attempts were made for each selection to produce higher response rates and more representative data. All contacts were assured of complete confidentiality, advised that their participation was voluntary and that they had the option of not answering specific questions. Once a participant had agreed to participate, an appointment was arranged in the next 10 days for the personal face-to-face interview. The interview began with certain demographical questions (age, sex, height, body weight, occupation, hours of sitting or standing, etc.) followed by questions on CVD divided into sections: (1) signs – telangiectasia or varicose veins, and/or, etc.; (2) symptoms – swollen legs, heavy legs, aching legs, and/or, etc.; (3) the symptoms were classified using a 5-scaled index: as always – all day, very often – in the evening, regularly 4–5 days/week, occasionally – rarely – only after tired day); (4) if the symptoms were presented during all the year or during a particular season or month. They were also asked to report on treatments: (5) if patients visit any physician, (6) the pharmacological treatment and (7) if patients were satisfied with that kind of treatment.
All the answers were recorded onto the questionnaires. At the end of the survey, all data were tracked and collected in a database for subsequent analysis. All symptom-related questions referred to a 12-month period before the interview.
Diagnostic criteria
The inclusion criterion for the participants was only to volunteer to participate in this study. The diagnostic criteria for the patients that had CVD were on the basis of clinical criteria: (a) all the patients should have had at least two symptoms of chronic venous disease the last 24 months and/or at least one sign of chronic venous disease (CEAP classification), (b) patients were without any other medical problem such as heart failure, liver failure or renal failure, or obvious arthritis in the legs.
Statistical analysis
Data were analysed using SPSS 15.0 for Windows (Chicago, IL, USA). Categorical data were compared with the corrected w2 or w2 for trend test or two-sided Fisher's exact test and continuous data were analysed with the Student's t-test. Logistic regression models were used for multivariate analysis. A P value of less than 0.05 was considered statistically significant.
Results
Demographic characteristics of participants in the survey
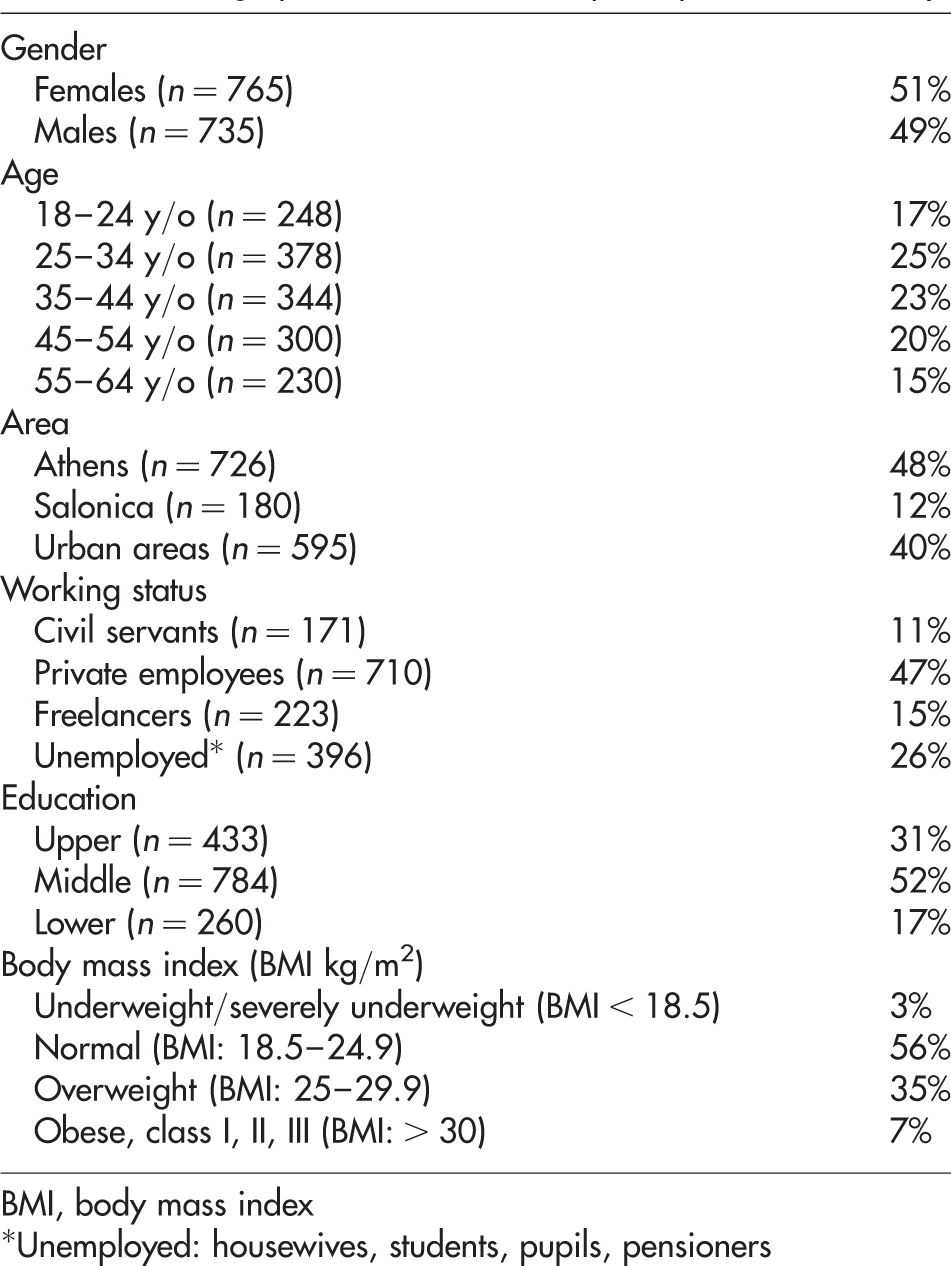
BMI, body mass index
*Unemployed: housewives, students, pupils, pensioners

Sufferers of chronic venus disease (CVD) within the general population
The symptoms that were mostly mentioned among CVD sufferers were 58% achy legs, 37.4% swollen legs and 25.3% heavy legs, whereas the frequent signs among sufferers were spider veins – telangiectasia (19.2%) and varicose veins (14.8%) (Figure 2). The most frequent symptoms among men were 56% achy legs and 22% heavy legs, whereas the most frequent symptoms among women were 59% achy legs and 48% swollen legs. The most frequent signs occured among female sufferers and obese sufferers (female sufferers: 26% spider veins – telangiectasia and 19% varicose veins; obese sufferers: 35% spider veins – telangiectasia and 25% varicose veins).
The symptoms and signs that were mostly mentioned among chronic venous disease (CVD) sufferers
Concerning obesity, which is a risk factor for CVD, we found out that the mean average body mass index (BMI) of people was 24.6 (men: 25, women: 24.3). Among the total population, 35% were overweight and 7% obese. Out of 224 patients, 141 (62.9%) had both CVD and obesity (BMI > 25).
Moreover, when examining their way of life (standing), we found out that from 948 working persons, 767 were standing during their work with 515 persons experiencing prolonged standing at work for at least 4+ hours The occurrence of CVD among persons with prolonged standing hours at work (4+ hours) was 20.8% with 70% of them at least occasional sufferers (Figure 3).
Chronic venous disease (CVD) among the total population and working people standing at work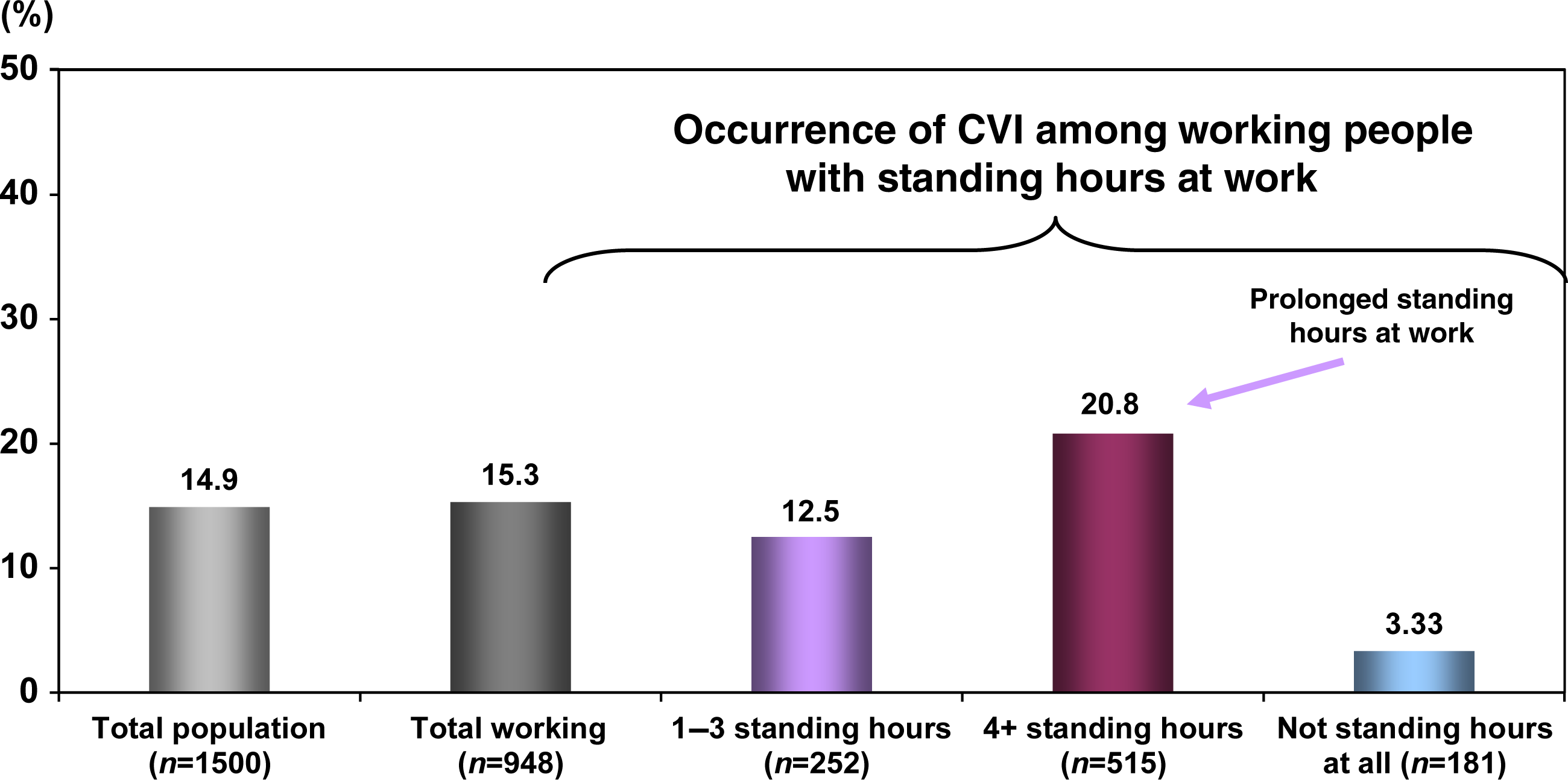
When sufferers (224 persons) were asked in which season CVD symptoms were more intensive, 50.8% did not associate their condition with any particular season, whereas only 26.8% mentioned the summer period. During summer CVD symptoms worsen, mainly among women (32.1%) and among obese patients (47.8%) (Figure 4).
The presence of CVD among the total population during the seasons and by gender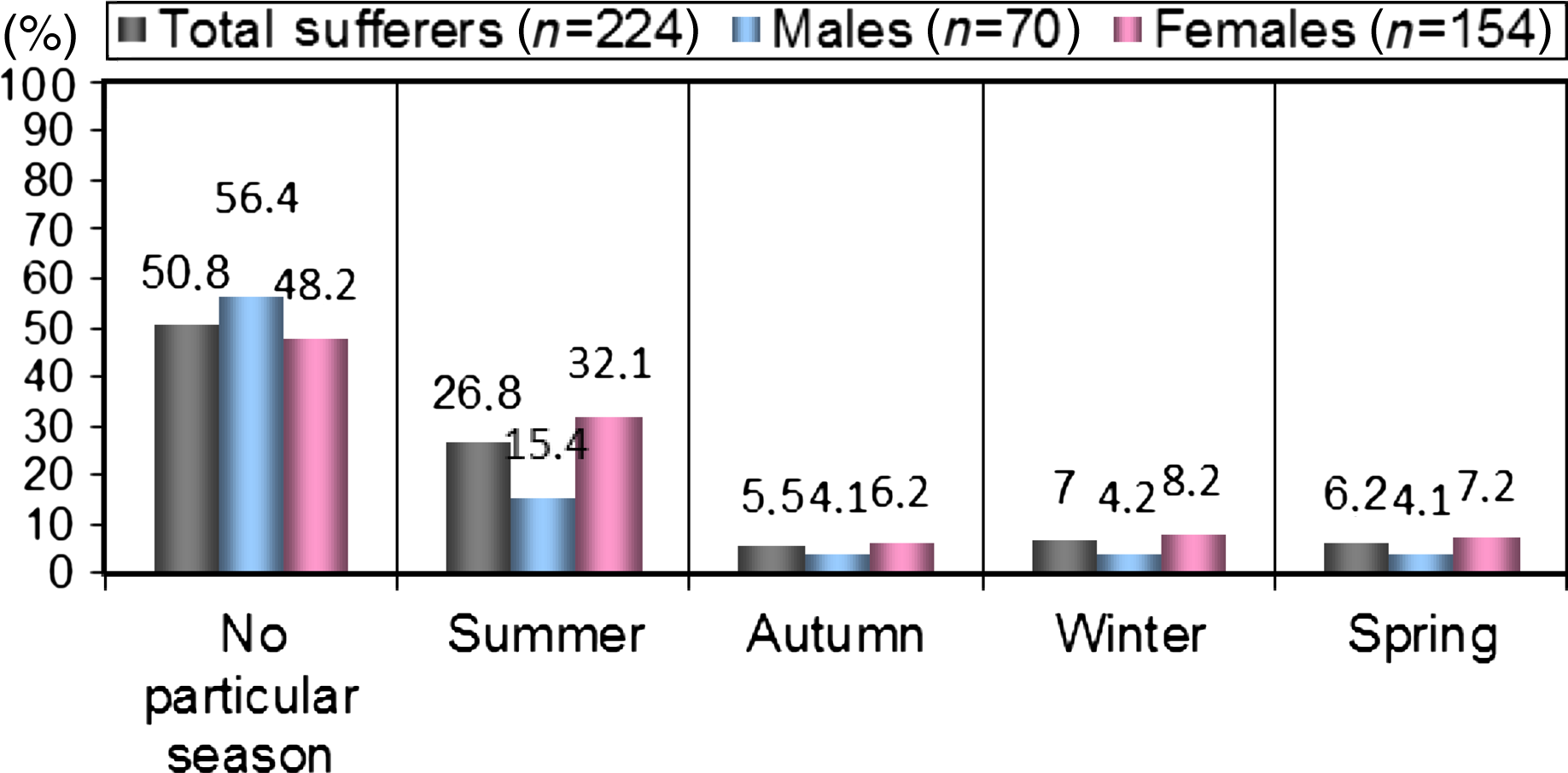
Sufferers mentioned that they took first advice from physicians (28%), from friends or relatives (27%) and (26%) from pharmacists. Fifty-two percent of systematic sufferers mentioned that they visited a physician for first advice.
The specializations of the physicians visited were general practitioners/internists (60%) and vascular surgeons (25%), while 15% visited other specialists.
Out of 224 sufferers, 28% visited physicians, 37% of them did not receive any drug, 22.2% did not remember the drug's name and among 40.6% that received medication, 25.4% were given flavonoids, 9.5% non-flavonoids and 9.5% topical drugs.
Sufferers received that treatment for on average 7.5 months and 76% of them were satisfied by the treatment, 20% were neutral, while only 5% were very dissatisfied.
Discussion
There are a lot of epidemiological studies on CVD because CVD is a common disease mainly in Western Europe and the USA.4,8–13 CVD is a simple disease but it has important complications such as haemorrhage, ulcers, venous thrombosis and pneumonic embolism.14,15 This study is a wide epidemiological Greek study concerning CVD in the general population and its findings are very important. About 14.9% of the general Greek population presents the symptoms and/or signs of CVD. The prevalence of symptoms/signs is lower compared with other studies and it could be explained by the younger age of the population and by the participation of men. The presence of CVD is mainly in women and less in men (2:1) and the biggest percentage of presence of CVD was in 45–64-year-olds. That depends on hormonal factors in women, the way of life (sitting or standing), pregnancy, age, obesity and heredity factors that help to cause and to develop CVD.3,4,16
Obesity plays a very important role and this study confirms it: most of the patients (62.9%) with BMI > 25 present with CVD perhaps due to difficulty walking and, in addition, they may have either many hours of standing and/or many hours of sitting. These situations increase the hypertension of the venous system and this leads to CVD.17–19 At this point we have to emphasize that obesity, as it is known, it is a serious risk factor among the patients from C3–C6 and less among C0–C2, and that the high percent of 62.9% is perhaps due to the fact that the patients themselves think that CVD is not an important disease and they are not interested in their disease especially for the first stages of CVD.
From the study the low percentage of CVD in patients with prolonged standing (20.4% – >3 hours) showed to us that our lifestyle is not a risk factor for CVD but is an influencing factor among the patients with CVD, which could worsen the symptoms and the signs of CVD. The mechanism of appearance of CVD is the same as we describe latterly concerning obesity. Moreover, as we know, walking helps the calf muscle pump function to push venous blood to the heart.20–22 The immobilization of those patients (prolonged standing and/or sitting) increases the hypertension of the venous system and it leads to CVD, so walking and generally exercise are very important tools in order to prevent or to avoid the worsening of CVD especially in patients that have many hours of standing or sitting in their work.23–25
Another important finding is that most patients reported that their symptoms did not worsen in any particular season and only 26% answered that the symptoms worsened during the summer. It is known that when patients are in a hot environment the venous symptoms worsen. 26 The fact is that about 50% of the patients report the presence of symptoms during the entire year and not only during the summer season. This is due to Greece and generally the Mediterranean countries are hotter than the Northern countries of Europe. This means that physicians in Mediterranean countries have to consider that CVD is not only a summer disease but also a chronic disease all year and they have to give good advice and the best treatment to patients.
In our study we had a surprise finding: the patients took first advice about their disease with almost the same percent either from friends and relatives (27%), or physicians (28%) or pharmacists (26%). This indicates to us bad management of the disease from the patients and perhaps from some physicians, perhaps due to no good, correct and timely diagnosis of the symptoms of the patients when they suffer from CVD. It means that more efforts are needed to raise the awareness of the patients in the form of education on CVD, clear guidelines from the Ministry of Health and comprehensive information from media (television, radio, etc.). From the point of view of the physicians, they must always be aware about the latest data, the guidelines for diagnosis and the treatment of CVD. 27
Concerning the trouble with leg CVD, one-third of the persons with CVD (about 40%) admitted that they have either health or cosmetic problems to such a level as to be burdened from going somewhere (19.5%) or to cancel activities and stay at home (11.8%), to avoid wearing clothes exposing their legs (8.7%), or to avoid going on vacations to very warm places (6.6%) (Figure 5). This fact confirms that CVD is not only a severe disease but is also a disease linked with social issues that can create many and important difficulties in the everyday activities of the patient.9,28–31
The quality of leg status among the sufferers with chronic venous disease (CVD)
There are a lot of drugs for the treatment of CVD.32–34 In this study we found out that only two-thirds (62.8%) of the patients who visited physicians are recommended phlebotonic drugs, either pills and/or topical gels (only Vitis Vinifera/AS 195 or heparinoids) in order to get better relief of the symptoms of CVD.35,36 But it is important to note that there was a huge percentage (76%) of patients who were satisfied with that pharmaceutical treatment especially when the patient received both systematic and topical drugs for better relief of the symptoms of CVD. Thus, the treatment of CVD with drugs only is not enough, but we definitely need to use elastic garment compression, the treatment of the risk factors of CVD such as obesity or the way of life, venous exercises and absolutely direct communication with the specialist physician who can give the right advice to patients on health care – as well as sometimes surgery and sclerotherapy.
Conclusion
This is an epidemiological Greek survey – a representative study of the Greek population that provides important and remarkable data about prevalence, incidence of symptoms, the signs, the risks and aggravating factors and the pharmaceutical treatments for the disease known as CVD. The knowledge of the status of a disease in a country could help and improve the relationships within the triangle comprising physicians, patients and disease.