
Abstract
Objective
Endovenous laser treatment (EVLA) is fast gaining acceptance as an alternative to open surgery for the treatment of saphenous vein incompetence. The method of action of these techniques is based on heat, making tumescence anaesthesia necessity. Heat-induced complications may occur with inadequate application of tumescent anaesthesia. Our hypothesis was, local cooling effect of tumescent anaesthesia on tunica adventitia might be kept undamaged from disruption due to the thermal injury.
Methods
We experimented with two popular laser wavelengths (980 and 1470 nm) and with two different thermal media (+4 and +24°C) in vitro for perforation. Twenty different 12 cm length vein pieces were numbered randomly to set up four groups of the experiment. Endovenous laser procedures were applied in same manner in a unique design test tube with same energy density per pieces on same duration (10 W/second) (linear endovenous energy density 60 J/cm). Procedure video was recorded for macroscopic perforations. All postprocedure vein segments were examined microscopically.
Results
Activities of both wavelengths were much better in cold medium (P < 0.05). Cold tumescent anaesthesia reduces the bleeding complication rate. But the performance of 1470 nm laser was better than that of 980 nm in cold environment (P = 0.0136).
Conclusions
It can be commented that reducing the ambient temperature is more beneficial than modifying the laser wavelength on perforation rates. Therefore we suppose tumescent anaesthesia temperature is effective on perforation independently from the wavelengths or type of the laser fibre.
Introduction
Recently minimally invasive alternatives to open surgery for the treatment of long saphenous vein incompetence have been developed. Endovenous laser treatment (EVLA) is gaining rapid acceptance as an alternative to open surgery for the treatment of long saphenous vein incompetence.
EVLA achieves long saphenous vein closure through the delivery of laser energy directly into the blood vessel lumen to produce endothelial and vein wall damage with subsequent fibrosis and long saphenous vein closure.1–5 Most of the published EVLA data concern 810-, 940-, 980-nm diode and 1064- or 1320-nm Nd: Yag laser systems. In most publications, the success rate after various follow-up observation times is 90–100%.6–8 Results after EVLA with 1320 nm showed good occlusion rates, and less bruising and less pain. Higher wavelengths, more specific for water than for blood, might be useful.9–12 It is discussed whether these systems produce more direct damage to the venous wall and not indirectly by steam bubbles as demonstrated with the diode lasers of 810–980 nm. 13
The method of action of these techniques is based on heat, making tumescent anaesthesia necessity. Most of the tumescence anaesthesia combination includes different ratio of lidocain, epinephrine and sodium bicarbonate. 14 The intracompartmental infiltration of a large volume of this fluid causes the targeted tissue to become swollen and firm, or tumescent, and permits procedures to be performed on patients without general anaesthesia while minimizing blood loss due to the vasoconstrictive effect of epinephrine. 15
Most EVLA series describe the use of local anaesthetic infiltration of the perivenous stroma for tumescent analgesia and protection against thermal injury to the nearby structures.2–5 Heat-induced complications such as skin burns, nerve damage and prolonged pain may occur inadequate application of tumescence anaesthesia.
The complications were classified as minor or major according to the Society of Interventional Radiology Standards of Practice Committee Guidelines on reporting complications. Ecchymosis, pain, induration, skin burns, dysaesthesia, superficial thrombophlebitis and haematoma were classified as minor complications. Deep vein thrombosis and nerve injury were classified as major complications. 16
Reason for haematoma and ecchymosis is bleeding from the perforated vein segment. The optimum energy density is still controversial for EVLA procedures. Catheter researchers argue how their perforation rates are lower than the rest. 17
We experimented effects of two different laser wavelengths in the EVLA procedure in two different temperature media (+4 and +24°C) and to research how variation on tumescent cooling works on perforation rates.
Methods
Saphenous veins were harvested in similar lengths in 20 consenting patients who were undergoing coronary bypass graft surgery. Great saphenous vein (GSV) was removed from the thigh by stripper as minimal invasive surgical technique without extra incision. Dissection of the vein is carried out in a similar manner except that branches are divided in situ and ligated once the vein is explanted. After harvesting, all veins were stored in autologous heparinized blood and Ringer's solution mixture. The Hospital Human Ethics Committee under the guidelines of the National Health and Medical Research Council approved the protocol.
Our hypothesis was collagen in tunica adventitia might be kept from disruption of the thermal injury of laser via localized cooling. So we designed a cold media passing in a tube in order to cool external surface of vein. We applied laser energy in a frozen cold serum in order to cool the adventitial collagen.
Twenty different 12 cm vein samples were numbered randomly to set up four subgroups of the experiment. In the standard group (n = 10) (normal room temperature tumescence fluid, +24°C) two different laser wavelengths were tested (980 and 1470 nm radial tipped porcelain covered 600 μ laser fibre). Each catheter was tested also in cold tumescence solution (+4°C) as the cold group. Vein diameters were taken with digital caliper (TESA technology, TESA CAL IP67 magna & mu system, Rennes, Switzerland, TESA SA) after filled up with fresh blood. Time is very important from harvesting to experimentation. EVLA procedures were performed immediately after harvesting saphenous veins to avoid the epithelial desquamation. Endovenous laser procedures were applied in same manner with the same energy density and for same duration on all samples. A1470-nm diode laser (Elves radial, Biolitec AG, Bonn, Germany) with radial emitting fibre was used at a power of 10 W in the continuous pullback mode (10 W/second, linear endovenous energy density [LEED] 60 J/cm). Laser energy was administrated over the straight section of the vessel, by pulling back 1 cm in six seconds. A unique experiment tube was designed and used during the experiments (Figure 1). Experiment contrivance is constructed from a glass cylinder that has two plastic plugs on each poles, one of them got implanted a short introducer for laser catheter insertion into vein.
(a) Experiment contrivance is constructed from a glass cylinder that has two plastic plugs on each poles, one of them got implanted a short introducer for laser catheter insertion into vein, (b) There is a vein, which is suspended in the middle of the tube that is filled up with tumescent media. In vitro endovenous laser ablation procedure is seen in this picture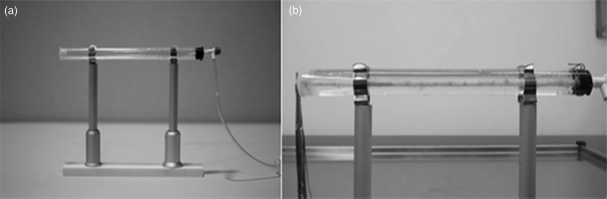
Procedure video was recorded for macroscopic perforations. An unbiased interpreter was asked to examine each vein segment. Each postprocedure video was analysed via macroscopically counting perforations.
Double blinding method
To ensure the objectivity of the experiment we double-blinded the operators. One operator gave a random number to the procedure and applied the laser process, while recording video, and a second interpreter analysed and noted the numbered videos for perforations by counting on the tissue samples afterwards another time.
Statistical method
Statistical analysis was performed with Graphpad Instat software (version 3 for Mac; version 11.5, GraphPad Software Inc. La Jolla, California, USA). All values were expressed as median and min–max. Variables between groups were compared by Kruskal–Wallis test and Dunn's multiple comparison tests as post-test. Comparison of the variables between tumescent anaesthesia temperatures and laser wavelengths was performed using Mann-Whitney test. A P value <0.05 was considered statistically significant.
Results
After performing a statistical analysis to four subgroups, we obtained striking results compared with the current literature.18–20 Perforation counts median value and minimum (min) and maximum (max) range of values after laser procedures are shown in Table 1. Two popular laser wavelengths were tested in the standard tumescent medium, which is currently the worldwide standard, and in cold tumescent solution. In comparing the 980 nm wavelength in the cold environment with 1470 nm in the standard environment, there was not a significant statistical difference in terms of perforation rates. But the performance of the 1470 nm laser is better than that of the 980 nm in cold environment (P = 0.0136). Both wavelength performances were much better in cold environment than in the standard environment (P < 0.05). Application of 1470 nm laser in the cold environment reduces the perforation rate in comparison to the 980 nm laser in the standard environment (P < 0.001). Cold tumescent anaesthesia should be used in conjunction with the 980 nm wavelength laser catheter in order to avoid relatively high perforation rates (Table 1).
Perforation numbers of subgroups
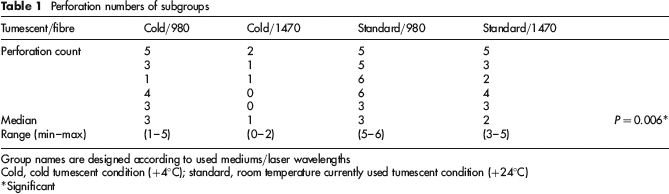
Group names are designed according to used mediums/laser wavelengths
Cold, cold tumescent condition (+4°C); standard, room temperature currently used tumescent condition (+24°C)
Significant
When we compare the environment temperatures (+4 versus +24°C) independent of the laser wavelengths (Table 2a), which could be considered significant in favour of the lower temperature (*P = 0.0114). On the other hand, when we compare laser wavelengths (980 versus 1470 nm) independent of the ambient temperature (Table 2b), which could be considered significant in favour of the higher wavelength (*P = 0.0194).
Comparison of tumescent temperatures and laser wavelengths independently
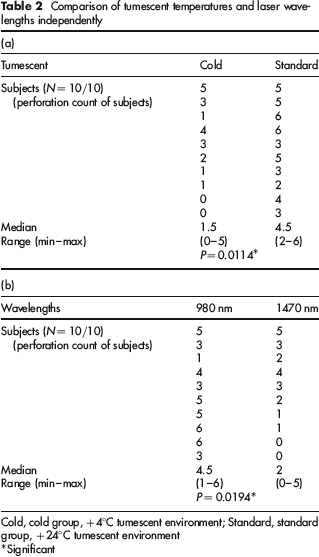
Cold, cold group, +4°C tumescent environment; Standard, standard group, +24°C tumescent environment
Significant
We used similar GSV segments in diameters in our experiment. The cold temperature group vein diameters (5.352 ± 0.47686 mm) and the standard temperature group vein diameters (5.254 ± 0.63416 mm) were similar (P = 0.7007) with a digital caliper.
Comments
The blood vessels are consisting of three major layers. Tunica intima (the thinnest layer), a single layer of simple squamous endothelial cells glued by a polysaccharide intercellular matrix, surrounded by a thin layer of subendothelial connective tissue interlaced with a number of circularly arranged elastic bands called the internal elastic lamina. Tunica media (the thickest layer) that is made up muscles mostly and tunica adventitia entirely made of connective tissue. Veins have different structures, they having two layers void of tunica media.
Connective tissue is found throughout the body. It has three main components: cells, fibres and extracellular matrix. Collagen is the main protein of connective tissue in animals and the most abundant protein in mammals, making up about 25% of the total protein content.21,22
Denaturation is a process in which proteins lose their tertiary structure and secondary structure by application of heat. If proteins in a living cell are denatured, this results in disruption of cell activity and possibly cell death. 23 Mechanism of action in EVLA is thermal injury of tissues, vascular spasm, thrombosis, fibrosis and occlusion of the vascular lumen. Histological evaluation revealed thermal damage of the intima and the internal part of the media. At the site of the laser tip, carbonization and necrosis were observed. Vascular perforation with subsequent perivascular bleeding was occasionally (<10%) seen in cases. 24
In the Schmedt and colleagues experimental ex vivo treatment study, the subcutaneous foot veins from freshly slaughtered cows, which were re-perfused in situ with, heparinized bovine blood. The veins were treated with either radiofrequency or with endoluminal 980 nm laser light using a continuous pullback mode. Immediately after treatment, perivenous tissue and veins were examined macroscopically Laser treatment produced carbonized lesions of the vein wall. After longitudinal opening of treated veins carbonized lesions of the vein wall were visible, increasing from the proximal start of the treatment toward the distal end. After 12–24 laser illuminations corresponding to 3.6–7.2 cm of vein length these lesions regularly became transmural, causing complete perforation of the vein wall. 25
Wall defects after EVLA ranged from nontransmural punctiform damage to complete perforation, depending on the energy density applied. 26
Pannier has published a prospective randomized comparative study, where he reported that, the temperature of the tumescence fluid did not influence the occlusion rate when a high LEED was used. In both groups pain and ecchymoses were less frequent than in our study with a 1470 nm diode laser or what is reported in studies with 810–980 nm systems. 27 But Pannier and colleagues’ conclusions may be due to the design of their study. Today, the current standard practice for tumescence fluid for local anaesthesia is at room temperature. Unlike in our study, where we focused on standard temperature and cold temperature tumescent fluid, Pannier and colleagues applied warm (37°C) and a cold tumescence fluid for local anaesthesia in the track of GSV.
Both wavelength performances were much better in the cold environment than in the standard environment in our study. Application of 1470 nm laser in the cold environment reduces the perforation rate in comparison with the 980 nm laser in the standard environment (*P < 0.001). Cold tumescent anaesthesia should be used in conjunction with the 980 nm wavelength laser catheter in order to avoid relatively high perforation rates.
When we compare the environment temperatures (+4 versus +24°C) independent of the laser fibre types (Table 2a), which could be considered significant in favour of the lower temperature. On the other hand, when we compare laser wavelengths (980 versus 1470 nm) independent of the ambient temperature (Table 2b), which could be considered significant in favour of the higher wavelength. It can be commented that reducing the ambient temperature is more beneficial than modifying the laser wavelength on perforation rates. We noticed that after the application of the 1470 nm laser, the number of perforations in the standard environment was higher than in cold environment and we considered that to be a very significant advantage in favour of the cold tumescent medium. Even if one prefers the 1470 nm water specific laser wavelength, we suggest use of cold tumescent anaesthesia for better postoperative results with lower complications. As evidence of a beneficial effect, cooling process reduces the number of perforations.
Some authors conclude that quantity of perforation on vein wall depends on vein diameter. Saphenous ablation using an 808 nm laser by variable retraction speed showed under histological evaluation that the average penetration of thermal injury in specimens was in the range of 10–900 μm, in other words 14.61% of the mean wall thickness. Complete intimal circumference injury occurred in 27.5% of the veins <10mm in diameter, full thickness damage was observed in 20.7% of the veins with a perforation rate of 6.9%. 28
In former EVLA studies, an LEED of more than 60 J/cm was proposed to sufficiently occlude GSV.29,30 Based on these results, lower energy densities should be studied in further trials. The results for occlusion rate, pain and ecchymosis were comparable to current methods. 31 In earlier studies using a lower wavelength and bare fibres, the majority of the patients developed ecchymoses or bruising and moderate postoperative pain for a few days. 32 According to Pannier, endothelia-specific laser fibres provoke less ecchymosis and pain. Twenty of the patients in his study developed bruising at any time and 44% had no postoperative pain. 33 Sroka et al. 4 demonstrated in ex vivo experiment that reduced ablation energy resulted in no perforation.
The most striking outcome of present experiment is high perforation rates observed at standard tumescent temperatures. We assume perforation rates in the recent literature do not reflect reality. 35 As a perforation indicator, previous clinical papers accept ecchymosis or haematoma.5,25,35 However, we suppose that having a perforation on the vein wall as a result of heat injury during ablation may be underestimated by presence of ecchymosis or haematoma alone. Blood oozing due to smaller vein perforations can cause blood accumulation in interstitial area and induce pain via nerve mediators. Not having clinically significant ecchymosis or haematoma does not imply lack of anatomical perforation. We suppose many perforations, which present with postprocedural leg pains, long in duration, have not shown up in previous clinical studies.
In our experimental organ bath simulator performing cold (+4°C) tumescent anaesthesia, we noticed lower perforation rates. Therefore we suppose tumescent anaesthesia temperature is effective on perforation rates independently from the wavelengths of the laser fibre used. We suppose, when we use cold tumescent anaesthesia clinically we may face with more favourable pain scores after EVLA procedures. Another interesting conclusion is that reducing the ambient temperature may be more beneficial than modifying the laser wavelength on perforation rates.