
Abstract
The aim of this paper is to describe the anatomical relations of the small saphenous vein (SSV) in order to define the high-risk zones for the treatment of chronic venous disease. The SSV runs in the saphenous compartment demarcated by two fascia layers: a muscular fascia and a membranous layer of subcutaneous tissue. The clinician should be keenly aware of the anatomical pitfalls related to the close proximity of nerves to the SSV in order to avoid their injury: At the ankle, the origin of the SSV is often plexiform, located deep below the fascia, and the nerve is really stuck to the vein. The apex of the calf is an area of high risk due to the confluence of nerves which perforate the aponeurosis. Moreover, the possible existence of a ‘short saphenous artery’ which poses a high risk for injection of a sclerosing agent due to a highly variable disposition of this artery surrounding the SSV trunk. For this reason, procedures under echo guidance in this area are mandatory. The popliteal fossa is probably a higher risk zone due to the vicinity of the nerves: the small saphenous arch is close to the tibial nerve, or sometimes the nerve of the medial head of the gastrocnemius muscle. In conclusion, before foam injection or surgery, a triple mapping of the small saphenous territory is mandatory: venous haemodynamical mapping verifying the anatomy that is highly variable, nerve mapping to avoid trauma of the nerves and arterial mapping. This anatomical study will help to define the main high-risk zones.
Keywords
Introduction
The 3 venous compartments of the lower limb
The subcutaneous tissues of the lower limb are arranged in two connective fasciae in the thigh and the leg: superficially below the skin is a thin membranous layer (formerly called the fascia superficialis), and a deep fascia layer, also called the muscular fascia, covering the muscles. These two layers delimit three venous compartments: (Figure 1)
The three compartments of the venous system of the lower limb: (1) skin, (2) saphenous fascia, (3) muscular fascia (aponeurosis) (from Caggiati A.). The deep venous system is located in the deep layer, beneath the muscular fascia: deep trunks (c) and muscular veins (d) inside the muscles (4). The saphenous trunks (b) are located between the two fascia layers inside the saphenous compartment (or saphenous ‘eye’). Tributaries (a) of the saphenous trunks are found under the skin The deep veins and the muscular veins located below the muscular fascia; The saphenous system located between the two layers, called saphenous compartment; The saphenous tributaries, located subcutaneously, also called epifascial veins.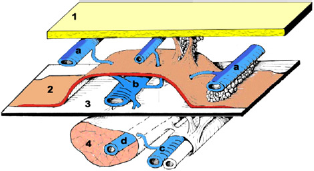
These two fascia layers are in close relation with the saphenous venous system: Bailly. 1 and then Lemasle 2 et al. have described the great saphenous vein (GSV) located between the muscular fascia and saphenous fascia. With ultrasonography, these fascia appear as two white lines surrounding a black dot; thus, forming an eye. This is the so-called ‘Egyptian eye’ sign (Figure 2).
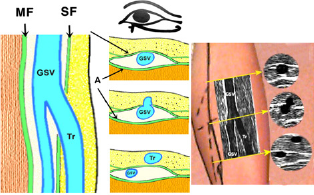
The ‘Egyptian eye’ and saphenous compartment: drawings and echo aspect. MF, muscular fascia; SF, saphenous fascia; GSV, great saphenous vein; Tr, tributary of GSV
This enables differentiation of the saphenous trunks, localized inside the ‘saphenous compartment'3–5 and the tributaries which run more superficially below the skin. This should be checked during venous mapping, which is now mandatory prior to treatment.
For this reason, the saphenous veins do not fit the classical description of ‘superficial’ veins.
This concept was validated at a consensus meeting organized at the UIP congress of 2001 in Rome. 6
Venous embryology 7 : theory of ‘angio-guiding’ nerves
One important fact during the embryo development is that the arrangement of the vessels parallels the layout of the neuronal network. From the axons and Schwann cells that coat them, they secrete a vascular endothelial growth factor, VEGF. This factor appears to have a two-fold role: to attract the primitive blood vessels to the vicinity of the nerves, and then to induce their arterial, venous or lymphatic specialization.8,9
The ephrin family (B2–B4) plays an important role in venous or arterial differentiation. 10 In addition, Le Noble 11 showed that arterial-venous differentiation and patterning are controlled by the blood flow.
In this way, three main ‘angio-guiding’ nerves (Figure 3) determine the venous development of the embryonic leg as we described previously:7,12 the axial nerve (or sciatic nerve), the preaxial of femoral nerve is a companion of the femoral vessels and the postaxial nerve a companion of the thigh extension of the SSV. Along the limb axis:
Embryogenesis with the three angioguiding nerves during the embryo development, (a) Embryo; (b) fetus; (c) adult. (1) Axial nerve (sciatic nerve), (2) preaxial nerve (femoral nerve), (3) postaxial nerve (posterior femoral cutaneous nerve), (4) preaxial venous plexus (femoral vein), (5) postaxial plexus (dorsal extension of the SSV), (6) axio-preaxial anastomosis (deep femoral vein), (7) axio-postaxial anatomosis (arch of SSV). SSV, small saphenous vein One can see the axial nerve or sciatic nerve (no.l, in yellow). One of its branches, the sural nerve directs development of the SSV; The preaxial nerve becomes the femoral nerve (no. 2, in pink); The postaxial nerve (no. 3, in white) becomes the posterior femoral cutaneous nerve.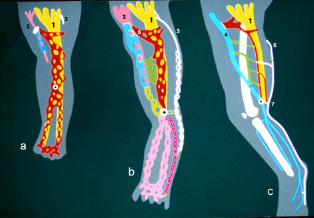
The axial venous plexus (coloured in red) participates in formation of the saphenous system. Ventrally the pre-axial venous plexus (in blue) becomes the femoral vein and the GSV. Dorsally the postaxial venous plexus (in purple) becomes the postaxial or dorsal extension of the SSV.
Thus, capillary blood vessels differentiate along vascular-guided nerves and produce several anastomoses, determining the final configuration of the venous system.
The axio-preaxial anastomosis in the thigh forms the emergence pathway for the deep femoral vein. It connects the axial plexus and its popliteal anastomosis dorsally with the postaxial venous plexus. This is the SSV arch. Ventrally, it connects with the preaxial venous plexus. It is the origin of the popliteal vein. Lastly, Giacomini's vein represents the posterior anastomosis of the SSV at the root of the thigh.
Descriptive anatomy
The objective here is to identify potentially hazardous areas in the treatment of venous disease by surgery, endovenous procedures or sclerotherapy based on anatomy, venography and ultrasound mapping of the venous system.
The saphenous compartment of the SSV
The SSV is located in the saphenous compartment but has some particularities (Figure 4).

The saphenous compartments along the limb with the great saphenous vein (1) anterior accessory of the great saphenous vein (AAGSV) (2) and the small saphenous vein (3). Please notice the thickness of the superficial fascia layer at the upper calf: at this level, it is truly an aponeurosis. It becomes thinner at the lower leg level
The SSV starts at the lateral malleolus. Running up the calf and back of the leg, the SSV and the GSV are located in the ‘saphenous compartment’. But in these areas, the membranous layer (saphenous fascia) is different. 13 It is thick and resistant, appearing more like an aponeurosis. Therefore, the SSV is an interfascial vein.
Functional anatomy
The fascial relations of the saphenous trunks suggest that muscular contraction affects their diameter and hemodynamics. In addition, the saphenous fascia acts as a type of mechanical barrier that can counteract pathological vasodilation in varicose veins.
The saphenous tributaries and collateral vessels emerge from this space and are devoid of any fascial sheath. In fact, they are unprotected and thus subject to varicose dilation before the large saphenous trunks are affected. 5
Descriptive anatomy of the SSV7,14,15
The SSV arises posterior to the lateral malleolus as a continuation of the lateral marginal vein of the foot, close to its companion nerve the sural nerve. It rises along the lateral border of the tendocalcaneus and then crosses to reach the middle of the posterior aspect of the leg.
Running upwards, it perforates the deep fascia in the lower part of the popliteal fossa between the heads of the gastrocnemius muscle. It usually ends in the popliteal vein, commonly with a thigh extension running vertically below the deep fascia.
Origin
The SSV originates in front of the lateral malleolus (Figure 5). It is usually formed by three roots: 16

Origin of the small saphenous vein (SSV) at the ankle. The lateral marginal (LM) vein is not a constant finding, but is often large. The lateral malleolar plexus (MP) on the contrary, is a constant finding. It gives rise to two perforator veins: P, premalleolar and S, submalleolar. One can see a common vessel of the lateral perforators of the foot (C), which is a true third root of the SSV; it crosses the fibular long flexor tendons: the intertendinous (I), and cuboidal (Cu) perforator veins
The lateral marginal vein, which arises from the perforator of the first metatarsal interspace and runs along the external border of the foot;
The lateral malleolar plexus, connected to two ankle perforators (premalleolar and submalleolar);
A common vessel of the lateral perforators of the foot, which is a true third root of the SSV It crosses the fibular long flexor tendons: the intertendinous and cuboidal perforator veins.
The ankle level and above is a high-risk zone because the vein is stuck to the nerve, as shown in Figure 6.
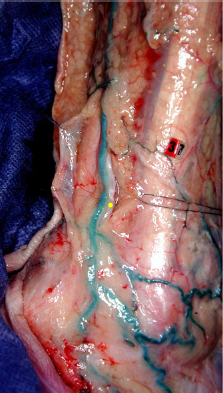
Anatomical dissection of the small saphenous vein and the sural nerve (yellow dot) at the ankle. Note the thickness of the fascia layer covering the structures peeled back (on the left). At this level, the nerve is really stuck to the vein
Apex of the calf
The junction at the apex of the calf provides an exchange for blood flow with its inferior leg tributaries (medial and lateral) (Figure 7). The distribution pathways of the SSV
14
are:
Anatomical dissection of the small saphenous vein (SSV) at the apex of the calf. Notice the thick membranous layer (open) of the SSV (1) at the upper calf level, showing the sural nerve convergence (2) and a medial gastrocnemius perforating vein (3) The great saphenous trunk or a posterior tributary; The inter gastrocnemius vein: this is the ‘vein of the sural nerve'; The muscular perforator veins in the calf: posterior and superior perforating veins of the medial head of the gastrocnemius; Apical perforating vein of the lateral head of the gastrocnemius; Trans-gastrocnemius: soleus perforating veins (lateral); Lateral perforating veins of the soleus muscle.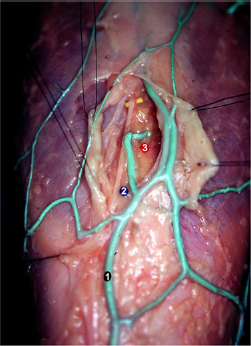
Termination of the SSV 15
In the popliteal fossa, the short saphenous vein runs a few cm above the popliteal fold to form an anterior arch before terminating in the posterior or posterolateral surface of the popliteal vein. This is the model anatomy.
However, the SSV termination is highly variable with three main types (Figure 8).
The main anatomical variations of the SSV (9) termination. Low termination (in red) in the popliteal vein (1, in light blue): (a) crossing the tibial nerve (2) medially; (b) crossing laterally; (c) lateral arcade next to the fibular nerve (3). Deep termination in the thigh muscles (d) biceps laterally, (e) semi membranosus medially. High termination either (f) in the popliteal vein or (g) in the deep femoral vein (5) Termination in the low popliteal vein. 1.1. The arch usually crosses the medial aspect of the tibial nerve (a) to join the medial or posteromedial aspect of the popliteal vein. In this case, it has a common trunk with the medial gastrocnemial veins in 30% of the cases. 1.2. Rarely, the arch crosses the lateral aspect of the tibial nerve (b), ending higher in the lateral aspect of the popliteal vein. It could also have a lateral arch next to the fibular nerve (c). Termination in the thigh muscles: the SSV has no saphenopopliteal junction (SPJ) and continues with the thigh extension vertically, ending in the semimembranosus (d) and biceps (e) muscles. Lastly, the SSV could have a high termination in the popliteal vein below the Hunter hiatus (f) or in the deep femoral vein (g).
From a practical and surgical point of view, we described with Lemasle et al. 17 five types of termination of the SSV (Figure 9) according to the presence (A and B) or the absence (C, D and E) of an SPJ.
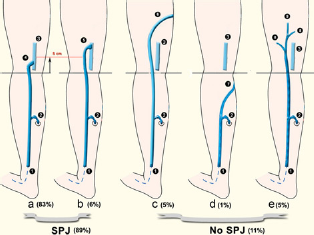
The different types and frequency of small saphenous vein (SSV). 17 (a, b) With saphenopopliteal junction (SPJ). (c, d and e) With no SPJ. SSV (1); calf gastrocnemial perforator (2); popliteal vein (3); normal SSV termination with a low arch (4); high termination (5); Giacomini's vein with no arch (6); short type of SSV ending with a communicating vein into the GSV (7); muscular perforators of the thigh (8); thigh (or dorsal) extension of SSV (9)
Type A: normal SPJ located <5 cm above the crease (83%):
Type A1: without a common trunk with the medial gastrocnemial veins (62%); Type A2: with a common trunk with the medial gastrocnemial veins (21%).
Type B: high SPJ, ≥5 cm above the crease (6%);
Type C: no SPJ, SSV extension by Giacomini vein (5%);
Type D: no SPJ, plexiform deep termination in the thigh muscles (5%);
Type E: no SPJ, short termination at the level of the leg (1%).
The existence of a venous arch (french ‘crosse’) is not a constant finding in normal subjects (70%). It is more common in patients with varicose veins because it is often responsible for a pathological reflux in this area (Cretan and Kohler 18 ). Such a reflux from higher points, the popliteal or deep femoral vein, feeds the superficial network.
In summary, the arch of the SSV usually crosses closely to the lateral or medial aspect of the tibial nerve, and distally, the nerve of the medial gastrocnemius also crosses the arch (Figures 10 and 11). Those nerves are at risk during thermal ablation and surgery of the SSV termination.

Anatomical dissection: The arch of the small saphenous vein (SSV, purple dot) crossing the medial aspect of the tibial nerve. The nerve of the medial head of the gastrocnemius muscle (yellow dot) crosses over the termination of the SSV in the medial aspect of the popliteal vein. The gastrocnemius trunk joining the SSV just before the saphenopopliteal junction (blue dot)
Anatomical dissection: The arch of the small saphenous vein (SSV, purple dot) crossing the medial aspect of the tibial nerve. The nerve of the medial head of the gastrocnemius muscle (yellow dot) crosses over the arch of the SSV (1) Sciatic nerve; (2) popliteal vein; (3) popliteal artery; (4) thigh (or dorsal) extension of the SSV; (5) sural nerve; (6) Hilus of the medial gastrocnemial muscle with the vascular pedicle; (7) arch of the SSV (purple dot); (8) vein of the sural nerve (inter gastrocnemial vein)
The ‘DEEP'extension of the SSV 19
It is known as an axial extension (aa) because it is located dorsally near the tibial nerve (axial nerve in the embryo). It can join an axial arch (A or sciatic nerve arch) that is located ventrally to the sciatic nerve (Figure 12).
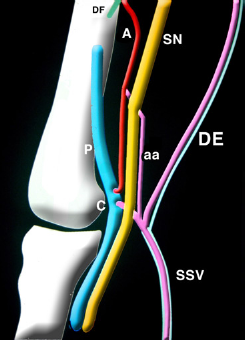
The veins of the popliteal fossa. The dorsal or thigh extension of the SSV (DE) with its companion the post-axial nerve. A preaxial vein (A) along the sciatic nerve (SN), axial nerve of the embryo and the axial arch (aa) joining the deep femoral vein (DF), P, popliteal vein; SSV, small saphenous vein; C, arch of the SSV
The ‘thigh extension'of the SSV14,19,20
Known also as the postaxial, cranial or dorsal extension of the SSV (postaxial nerve of the embryo), it is located more superficially, but below the muscular fascia. It accompanies the femoral posterior cutaneous nerve (Figure 12).
It perforates the fascia at various levels, and commonly gives rise to Giacomini's vein,21,22 an intersphenous anastomosis joining the GSV.
In about 5% of cases (Figure 8), the dorsal extension ends deeply inside the thigh, connected with the venous arcades of the semimembranosus and or biceps muscles. (Figure 13) These veins are draining upwards in the deep femoral vein (Figures 13 and 14).
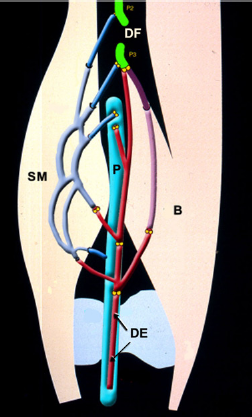
The connections of the thigh or dorsal extension of the SSV (DE): the muscular venous networks of the semi-membranosus (SM) of the short head of the biceps (B) joining the deep femoral vein upwards at the levels of the perforators P2 and P3. Please notice that the semi-membranosus has several arcades making a direct shunt between the popliteal vein and the deep femoral vein (P2 and P3 perforators). Therefore, these arcades could be considered as a safety valve in case of stenosis of the femoral vein in the Hunter's canal
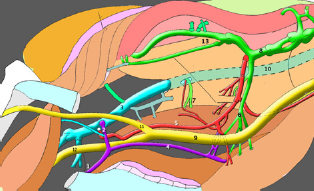
This drawing from a real case shows the modal SSV (1) termination by an arch (2) in the popliteal (3) vein with a thigh extension (4, in purple) joining the pre axial vein (5, in red) along the sciatic nerve also connected upwards with the muscular venous networks of the semi-membranosus (6) and short biceps (7). All these veins are ending in the deep femoral vein upwards (8, in green). (9) Sciatic nerve; (10) femoral vein; (11) fibular nerve; (12) tibial nerve; (13) veins of the vastus medialis muscle
So, the Giacomini's vein21,22 (intersaphenous anastomosis) consists of two parts: the thigh extension of the SSV and the anastomosis towards the GSV as first described by Cruveilhier. 23
The sural nerve pedicle
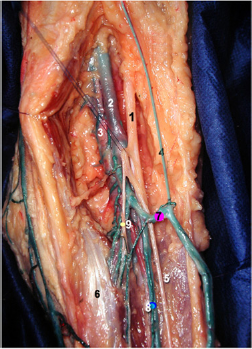
The sural nerve is an axial nerve formed by sensory branches of the tibial and peroneal nerves (Figures 15 and 16). The sural accessory nerve emerges from the fibular nerve, oblique and anterior to the lateral head of the gastrocnemius muscle, below the muscular fascia. At the apex of the calf, the sural nerve and its accessory branch join in a common trunk. This nerve can be called the ‘SSV nerve’ because it accompanies the SSV down to the ankle.

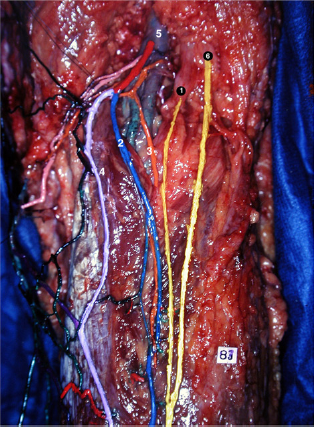
The sural nerve pedicle. The sural nerve (1) is formed at the apex of the calf (arrow) by two branches: one is located medially (2), coming from the tibial nerve (T), the second (3) comes laterally from the fibular nerve. It is the companion nerve of the inter gastrocnemial vein (4) or vein of the sural nerve and of the small saphenous artery (5) which originates from a common trunk with the medial gastrocnemial artery (6). Please notice the arch of the small saphenous vein (7, in purple) joining the popliteal vein (8) and crossing medially the tibial nerve (T) and laterally the medial gastrocnemial nerve (9)
Anatomical dissection of the sural nerve (1) with its companion vein (2, in blue) and artery (3, in orange). The small saphenous vein (4, in light purple) joins the vein of the sural nerve to form a common trunk (in red) ending in the medial aspect of the popliteal vein (5). Laterally, note the accessory nerve (6) joining the sural nerve at the lower part of the diagram (apex of the calf)
The sural nerve has two companion vessels:
Relationship between the SSV and the nerves
The sural nerve is distant from the SSV in the upper part of the calf, joining the SSV at the apex of the calf. From the apex of the calf, the so-called ‘SSV nerve’ is very close to the SSV vein down to the ankle.
In the popliteal fossa, the nerves are in a close relationship with the SSV termination:
The arch of the SSV usually crosses the lateral aspect of the tibial nerve, close to the nerve (Figures 8 and 11);
The medial gastronemial nerve is also very close to the arch, especially when the SPJ is low (Figures 10 and 11).
What is the relevance of these anatomical features for the daily practice of venous treatment?
The close proximity of these nerves to the SSV accounts for possible injury to the nerve during surgical procedures (invagination, phlebectomies and endovenous procedures).
This is particularly true:
At the popliteal level due to the high variability of the SSV termination: a good rule for endovenous laser treatment is to remain at least 4 cm below the popliteal crease to avoid a thermal injury of the nerves. An accurate ultrasound mapping is mandatory before surgery of the popliteal fossa;
At the apex of the calf where the two branches of the sural nerve join together;
At the ankle, a cautious dissection of the vein is necessary due to the closeness of the sural nerve, and any ‘conventional’ (non-invaginated) stripping of the SSV is contraindicated: the up to down invagination stripping under local tumescent anaesthesia is the best technique.
Several authors26,27 have described nerve complications after thermal ablation of the saphenous veins.
Therefore, for any treatment of the SSV (foam, surgery and endovenous ablation) it is highly recommended to perform a complete mapping by duplex ultrasound (Figure 17):
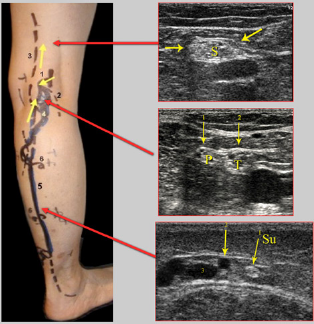
Mapping of the nerves before small saphenous vein (SSV) surgery. Skin marking showing reflux of the right SSV coming from the saphenopopliteal junction with a common trunk with the medial gastrocnemial veins. The arrows show: At the thigh level, the honeycomb aspect of the sciatic nerve (S) at the popliteal level, the tibial (T) and peroneal (P) nerves. At the apex of the calf, the sural nerve (Su), (1) SPJ; (2) gastrocnemial vein; (3) thigh extension of the SSV; (4) incompetent tributary of the SSV responsible for the reflux in the trunk below; (5) refluxing SSV trunk; (6) gastrocnemial perforator veins
First, a venous hemodynamic map to identify the patient's anatomy and reflux location28,29. Second a mapping of the nerves30,31 to verify their vicinity and to choose the best technique, approach or puncture site so as to avoid any nerve trauma during the procedure. Third, using colour mode to check for the presence of a small saphenous artery.24,25
This triple check is the best way to reduce the risk of severe arterial or nerve complications.
Case Reports of rare cases illustrated by computed tomography venography
In addition to the color duplex providing haemodynamic information, computed tomography (CT) venography provides a more precise morphological depiction of the venous map, creating a true guideline before treatment. This is particularly true in complex cases or recurrent varicose veins of the popliteal fossa after SSV surgery.32,33
Here are some case reports of rare patients assessed by CT venography and color duplex:
Ring shaped SSV arch (Figure 18)
Double SSV arch (Figures 19 and 20)
Dystrophic SSV termination (Figure 21)
SSV ending in an axial vein (Figure 22)
High termination of the SSV (Figure 23)
Common trunk of the SSV with the medial gastrocnemial trunk (Figure 24).

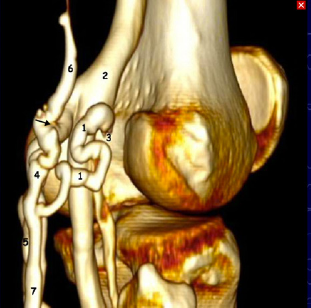
Case report of a varicose trunk of the small saphenous vein (SSV) with reflux. The SSV termination is ring-shaped. (1) Popliteal vein; (2) SSV trunk; (3) ring shaped arch of the SSV
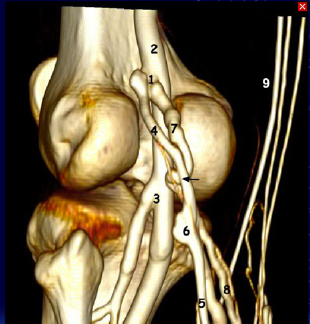
Case report of a varicose trunk of the small saphenous vein (SSV) with reflux. The SSV termination is X shaped with a medial gastrocnemial trunk (8) connected to the SSV (5) 1 cm above the valvular dilatation (6). The connection point is marked with a black arrow. Then, the arch is divided into two parts medial (4) and lateral (7) joining together just at the junction (1) with the popliteal vein (2). Medially, the GSV (9) is thin and competent. Notice the two roots of the popliteal vein joining (3)
Case report of true duplication of the small saphenous vein (SSV) arch. The three-dimensional model shows a lateral arch, sinuous and dystrophic (1) ending at the lateral aspect of the popliteal vein (2) at the level of the condyle. The SSV trunk (7) has also a medial arch (4) connected (arrow) to the gastrocnemial trunk (5), leading to a thigh extension of the SSV (6) running vertically
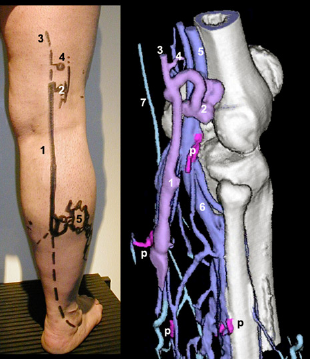
Case report of a reflux trunk of the small saphenous vein (SSV) trunk (1), with a dilated varicose tributary of the lateral aspect of the lower leg. The SSV termination is sinuous and dystrophic (2), ending in the lateral side of a duplicated popliteal vein (5). The arch gives birth to a thigh extension of the SSV (3). Notice the perforator of the popliteal fossa (4) and the several perforators of the calf (p)
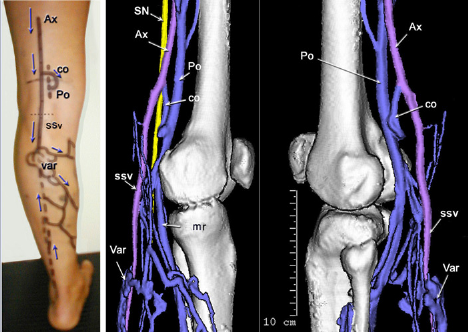
Case report of a varicose trunk of the small saphenous vein (SSV). The SSV reflux is fed by an axial vein (Ax). Notice on the skin map the varix of the calf (var) with no reflux in the lower part of the SSV trunk. The SSV is connected to the popliteal vein (Po) by a vertical communicating vein (Co). Notice the medial root (mr) of the popliteal vein. The identification of the feeding axial vein is done by the vicinity of the sciatic nerve (SN) according to the venous embryology
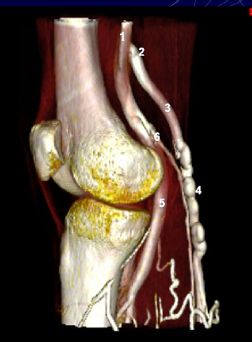
Computed tomography venography with a medial view of a right knee, showing the high termination (2) in the popliteal vein (1) 11 cm above the knee joint of a varicose SSV (3) with a dystrophic segment (4). (5) Medial root of the popliteal vein. (6) Gastrocnemial trunk

Computed tomography venography (posterior view of the right knee) showing a common trunk (1) of a varicose small saphenous vein (4) with the medial gastrocnemial trunk (2) ending in the lower part of the medial aspect of the popliteal vein. Notice the thigh extension of the SSV upwards (3), and the normal great saphenous vein medially (5)
In case of recurrence after SSV surgery CTV34–36 is highly recommended, in addition to duplex ultrasound, to precisely check the anatomy. The anatomy is often complex, and a good knowledge of the disposition of the roots of the popliteal vein is mandatory. 37
Conclusion
The clinician needs to be aware of potentially hazardous areas in the treatment of venous disease, particularly with injection, surgery or endovenous procedures38–41 of the SSV:
Possible existence of a ‘short saphenous artery,’ which poses a high risk for injection of a sclerosing agent due to the highly variable location of this artery. This is why sclerotherapy under echoguidance is highly recommended.24,25
Close proximity to associated nerves at the ankle level, at the apex of the calf and in the popliteal fossa. The clinician should be well aware of the anatomical pitfalls in order to avoid their injury.
42
The main rule is to use duplex to obtain a detailed understanding of the course of any nerve in the region of interest:43,44
At the ankle, the origin of the SSV often is plexiform, located deep below the fascia. The nerve is located very close to the vein, surrounded by fat, often dense and associated with sclerosis, which makes approaching it rather difficult. In the apex of the calf: this is an area that is the most hazardous:
It is the junction of several veins, with risk of perforations or of entering the wrong vein during catheterization. The confluence of nerves which perforate the aponeurosis. The perforating veins join the gastrocnemius muscles. In the popliteal fossa the SSV is very close to the nerves:
The short saphenous arch is close to the tibial nerve, or sometimes the nerve of the medial head of the gastrocnemius muscle. The existence of a common SSV trunk with the gastrocnemius veins is always associated with a medial arch of the tibial nerve. The axial extension of the SSV is along the tibial nerve and the sciatic nerve. The dorsal extension of the SSV is along the posterior cutaneous femoral nerve.
These findings also emphasize the usefulness of a triple check, verification of the anatomy of the veins, nerves and small saphenous artery, by ultrasonographic mapping prior to an invasive treatment of a varix of the SSV