
Abstract
Intravenous cannulation is a commonly performed procedure. This study aimed to determine whether the success rate and pain of intravenous cannulation is affected by prior injection of intradermal lidocaine. Intravenous cannulation was performed twice in 45 healthy volunteers. Intradermal lidocaine was administered prior to one of these cannulations. The outcome measures were success or failure of cannulation, and pain of cannulation, measured with a 100 mm visual analogue pain scale. The success rate of intravenous cannulation with and without prior intradermal lidocaine was 54% and 76%, respectively. The difference was 22.0% (95% CI 1.5-27.8%; P = 0.03). Log-linear analysis for three-way interaction between the variables (outcome, vascular condition and use of lidocaine) showed a significant influence of vascular condition on outcome (G 2 24.6, P < 0.001). The mean (SD) pain scores in the control and intervention group were 34.8 (21.0) and 13.6 (13.2) mm, respectively. The difference between the mean pain scores was 21.2 mm (95% CI 15.1-27.3 mm). In conclusion, the success rate of intravenous cannulation may be reduced with the use of intradermal lidocaine, but success rate is primarily dependent on vascular condition. Intradermal lidocaine achieves a clinically significant reduction in the pain of intravenous cannulation.
Introduction
Intravenous cannulation is the second most commonly performed invasive procedure in the UK after venepuncture, 1 and usually causes significant pain and anxiety to patients. Despite this, local anaesthetic infiltration prior to intravenous cannulation is rarely offered to patients in the ward setting. This may be because this technique is rarely taught to medical students, junior doctors or nurses. There is also a belief that local anaesthetic infiltration is time consuming and may make intravenous cannulation more difficult. 2
A number of different methods of reducing the pain of intravenous cannulation are available, including local anaesthetic creams, cutaneous coolant sprays, and both subcutaneous and intradermal injection of lidocaine. Local anaesthetic creams usually require a minimum application time of at least 30 minutes to be effective and are therefore impractical for immediate use. Studies investigating the effectiveness of coolant sprays have produced mixed results.3-6 Subcutaneous lidocaine reduces the pain of cannulation and does not significantly affect success rate irrespective of cannula gauge;7,8 however, intradermal lidocaine may be superior as it is less likely to cause local tissue distortion and has almost immediate effect, owing to anaesthetic being delivered directly to the small dermal nerves. 9 Intradermal lidocaine prior to intravenous cannulation has been shown to reduce pain and to be more effective than local anaesthetic creams and cutaneous coolant sprays.4,9-11 A literature search failed to identify any published studies comparing subcutaneous and intradermal lidocaine. While the intradermal injection itself can be slightly painful, the reduction in cannulation pain achieved justifies its use. 9 Intradermal lidocaine may be the optimal method of precannulation anaesthesia; however, more research is required. 12
The primary aims of this study were to:
Determine whether intradermal lidocaine prior to peripheral intravenous cannulation affects success rate;
Compare visual analogue pain score (VAS) in individuals cannulated with and without prior intradermal lidocaine.
The secondary aim of this study was to:
Investigate the influence of vascular condition on outcome.
Methods
The study was performed between February and April 2009. An email was sent to all medical students at the University of Dundee, informing them of the study and giving them the opportunity to participate. A power analysis performed when designing the study showed that to identify the predicted 20% difference in VAS pain scores, 44 subjects would be needed. Forty-five volunteers were recruited who were able to attend and did not meet the exclusion criteria (less than 18 years of age, currently receiving medical treatment).
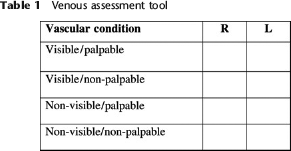
An attempt was made to cannulate each of the participants twice, once in the dorsal aspect of each hand. Intradermal lidocaine was used prior to one of the cannulation attempts and no anaesthesia was used prior to the other. The volunteers therefore acted as their own controls. Anaesthesia was used in either the right or left hand and for either the first or second cannulation attempt. This was randomized by the participants blindly selecting one of four numbered balls from a bag at the beginning of the study. A venous assessment tool adapted from that described by McGowan and Wood 13 (Table 1) was used to assess the vein to be cannulated. The hand to be anaesthetized received 0.1 mL of 1% lidocaine intradermally, using a 29 gauge needle (using a 1 mL insulin syringe) and cannulation was performed immediately after with a 20 gauge cannula. The opposite hand was cannulated without prior anaesthesia, using a 20 gauge cannula. A 20 gauge cannula was used as it is the most commonly used cannula in clinical practice. 14 Each cannulation was attempted only once and was not attempted in any vein assessed as being non-visible, and/or non-palpable. When cannulation was thought to have been successful, 3 mL of saline was flushed through the cannula for confirmation. Immediately after this the cannula was removed.
Venous assessment tool
Immediately after each cannulation, participants were asked to rate the maximal pain experienced using a 100 mm VAS (0 mm = no pain, 100 mm = maximal pain). The VAS is a validated tool for the assessment of pain 15 and has been used by many other studies investigating pain associated with cannulation. Participants were shown the scale and explained how to use it at the beginning of the study.
The study was carried out in the University of Dundee Department of Anaesthesia. All cannulation attempts and administrations of lidocaine were performed by the chief investigator, a fourth year medical student, supervised by a consultant anaesthetist. The student had undergone the standard formal training on cannulation received by undergraduate students at the University of Dundee (a 2 hour practical tutorial) and performed around 20 intravenous cannulations in a clinical setting prior to commencing the study.
The success rates in the control and intervention group were analysed using McNemar's test. Log-linear analysis was used to measure three-way interaction between the outcome, use of lidocaine and vascular condition.
Results
The study group comprised 22 men and 23 women. Eighty-two percent (n = 37) of the participants were aged 18-25. The remaining 18% (n = 8) were aged 26-35. Cannulation was not attempted in four hands (3 participants) as vascular condition was rated as non-visible/non-palpable. Of these four hands, three were to receive lidocaine and one was to receive no lidocaine. One hand was injected with subcutaneous lidocaine accidentally and was therefore removed from the study. This left 41 participants in whom data were complete.
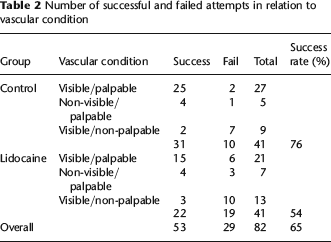
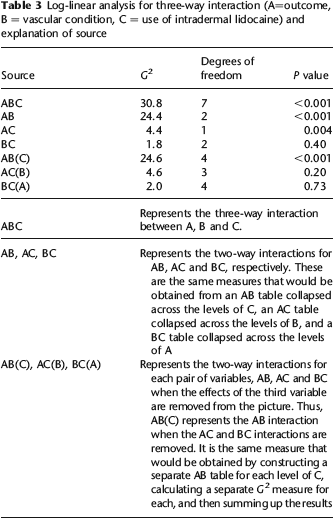
The outcome of cannulation, i.e. success or failure, in relation to the use of lidocaine and vascular condition can be seen in Table 2. The difference in success rates between the control and intervention group was 22.0% (95% confidence interval 1.5-27.8%; P = 0.03). The data were also analysed for three-way interaction between the outcome, use of lidocaine and vascular condition. These results can be seen in Table 3.
Number of successful and failed attempts in relation to vascular condition
Log-linear analysis for three-way interaction (A=outcome, B = vascular condition, C = use of intradermal lidocaine) and explanation of source
The mean (SD) pain score in the control group was 34.8 (21.0) mm. The mean (SD) pain score in the intervention group was 13.6 (13.2) mm. The difference between the mean pain scores was 21.2 mm (95% confidence interval 15.1-27.3 mm). The pain of cannulation with lidocaine was rated as greater than without any anaesthesia in three (7%) participants.
Discussion
This study showed that intradermal local anaesthetic did not reduce the success rate of intravenous cannulation, carried out by a fourth year medical student when the differences between vascular condition in the control group and lidocaine group were accounted for. The VAS pain score caused by intravenous cannulation was significantly lower when intradermal lidocaine was used. This was both statistically and clinically significant.
At first glance, the results of this study appear to show a reduction in success rate when intradermal lidocaine is used prior to cannulation. Further analysis of the results for interaction between the variables (outcome, use of lidocaine and vascular condition) shows that the initial finding may have an oversimplification. The most significant variable affecting success rate is vascular condition. When the effects of vascular condition are removed, the difference in success rates in the lidocaine and control group does not reach statistical significance. The lack of an actual difference or the low number of participants with veins assessed as non-visible/palpable or visible/non-palpable in this study, may be the reason for this. While one previous study investigating intradermal lidocaine assessed vein visibility prior to cannulation, 11 it did not reveal nor specifically discuss success rate.
Studies that have published cannulation success rates have found this figure in control groups to range from 71-100%.3,5,7,10 The success rate in the control arm of this study is at the lower end of this range. There are several reasons for this. Study design meant that cannulation was attempted in the dorsum of every hand. This differs from some previous studies and clinical practice, where time may be spent looking for a suitable vein elsewhere. The chief investigator's experience in cannulation is also likely to be less than investigators in previous studies, several of which were carried out by senior doctors.9,11 However, the experience of the chief investigator was similar to that of other medical students, junior doctors and nurses. The study is therefore perhaps more relevant to these less experienced individuals.
Although the final outcome of cannulation was measured in this study, the difficulty of cannulation was not. Previous studies have produced conflicting results on the effect of intradermal lidocaine on cannulation difficulty5,11 and further research into this area may be beneficial.
The reduction in pain demonstrated in this study is in keeping with previous findings.4,9-11 A difference of 13 mm has previously been judged to be clinically significant.16,17 The findings in this study are therefore both statistically and clinically significant. The three participants who rated the pain of cannulation with lidocaine to be greater than without, found the injection of intradermal lidocaine to be more painful than cannulation itself. Despite this, the mean reduction in cannulation pain with intradermal lidocaine probably justifies its use for this purpose. This is in keeping with previous findings. 9
All studies measuring pain suffer from an inherent difficulty; that pain is subjective and dependent on both physical and emotional factors. This study tried to minimize this problem in a number of ways. All participants were treated in the same room by the same investigator. We felt the use of participants as their own controls was a particular strength of the study, ensuring relative homogeneity between the intervention groups and minimizing the influence of the subjective nature of pain. It was not possible to blind either the participant or investigator, owing to the nature of the intervention. This creates a similar scenario to that experienced in clinical practice and is therefore still relevant. It was felt that non-blinding would not have a significant effect on success rate. While it may have affected perceived pain, this was minimized by randomly allocating participants to receive the intradermal lidocaine either first or second.
Conclusion
The results of this study were inconclusive and a larger study, which takes the effects of vascular condition prior to cannulation into account, is required. Nevertheless, we feel the results of this and previous studies advocate that the technique of local anaesthetic infiltration prior to intravenous cannulation is taught to medical students, junior doctors and nurses.