
Abstract
Aneurysms of the extracranial carotid artery are rare but may have debilitating clinical consequences. A case causing a cerebrovascular accident is reported followed by a discussion of the clinical features, investigation and treatment of this condition. Aneurysms usually develop in the common or internal carotid artery (ICA) and presentation typically results from cerebral embolization. Distal ICA lesions are often not detected during ultrasound examinations, and computed tomography is most commonly used to plan treatment. This may be performed by open surgery or endovascular intervention.
Extracranial carotid artery aneurysms are rare, accounting for approximately 1% of all arterial aneurysms and 1% of carotid surgical procedures, but may have devastating clinical consequences.1–3 Ultrasound (US) plays a major role in the diagnosis and quantification of carotid atherosclerotic stenoses, but may be limited in its ability to detect this particular condition. This article reports the case of an internal carotid aneurysm and reviews the diagnosis and management of this interesting condition.
Report
Clinical features
A 56-year-old woman presented to her general practitioner with a history of sudden weakness of the fingers of her right hand. This had occurred two weeks prior to the consultation and had significantly improved. However, a residual subjective weakness persisted associated with a feeling of unsteadiness on her feet. There was no history of headache, visual disturbance or other neurological symptoms.
Her past medical history included hypertension and mild asthma controlled with bendroflumethiazide together with budesonide and terbutaline inhalers. There was no history of significant trauma. In addition to hypertension, her risk factors for vascular disease included being an occasional smoker and that her mother had suffered a myocardial infarction in her 50s. She was not diabetic.
She was subsequently referred to a neurologist who, on examination, found a mild weakness of her right arm in association with hypertonic reflexes. However, there was no muscle wasting or fasciculation, and examination of her other limbs, cranial nerves and gait was unremarkable. A differential diagnosis of either a cerebrovascular accident or cervical spine pathology was formulated. Aspirin 75 mg and simvastatin 40 mg daily were prescribed and magnetic resonance imaging of her brain and cervical spine was requested. This revealed no focal brain or cervical spine lesion to account for her clinical presentation. However, it did demonstrate an abnormality on the left side of her neck, which was reported to be a ‘focal ectasia of the jugular vein’. A US examination was recommended, the results of which prompted urgent referral to a vascular surgeon who arranged a computed tomography (CT) angiogram.
Imaging findings
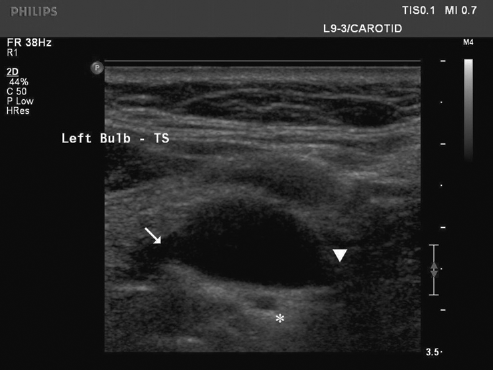
The US examination was performed in the supine position with a Philips iU22 using the L9-3 MHz (40 mm linear array) transducer (Philips Medical Systems, Surrey, UK). Compound and harmonic imaging improved image quality and were therefore utilized.
Initial US imaging revealed prominent and dilated vascular structures, but their exact relationship to each other was complex. Scanning in the cephalad direction along the distal common carotid artery (CCA) in longitudinal section leads, as expected, to the bulb (Figure 1). However, superior to this was a dilated vessel that initially appeared separate from the bulb (Figure 2). In transverse section, the bulb/CCA bifurcation appeared to be splayed; the external carotid artery (ECA) ran anteriorly while the internal carotid artery (ICA) coursed posteriorly and, after a tortuous route, was continuous with the dilated vessel first seen (Figures 3 and 4). This dilated structure had a maximum transverse diameter of 2.1 cm and contained pulsatile flow, confirming it to be an aneurysm of the ICA rather than an abnormality of the internal jugular vein as previously reported. No mural thrombus was detected.

Ultrasound image of left distal common carotid artery in longitudinal section (asterisk)

Ultrasound image of left distal common carotid artery in longitudinal section. Note the dilated vascular structure (asterisk) that initially appeared separate from the bulb (arrow)
Ultrasound image of common carotid artery bifurcation in transverse section. Note the external carotid artery running anteriorly (arrow) and the internal carotid artery coursing posteriorly (arrowhead). A segment of the tortuous internal carotid artery is also demonstrated in cross-section (*)

Ultrasound image of internal carotid artery aneurysm in transverse section containing pulsatile flow
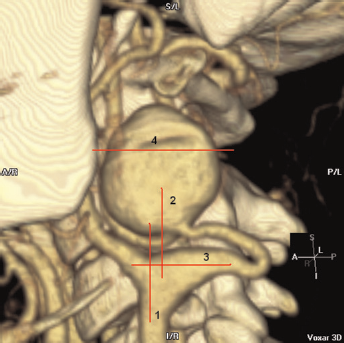
The CT angiogram was performed on an eight-slice GE Light Speed Ultra (GE Healthcare, Buckinghamshire, UK). The three-dimensional (3D) reconstruction illustrates the complex arrangement of the saccular ICA aneurysm in relation to the adjacent carotid arteries (Figure 5). The US probe positions of Figures 1–4 are superimposed upon the image to aid interpretation.
Treatment
Following US examination, the cause of the neurological dysfunction was considered to be an ischaemic stroke. Despite the absence of mural thrombus, the ICA aneurysmwas almost certainly the embolic source and so intervention was recommended. The tortuosity of the adjacent (proximal loop of the same vessel) ICA precluded endovascular intervention, and therefore open surgery was required (Figure 6). This involved mobilization of the carotid arteries, resection of the aneurysm and then restoration of cerebral perfusion by anastomosis of the distal and proximal ICA. Biopsies of the aneurysm wall were sent for histological and microbiological analysis.
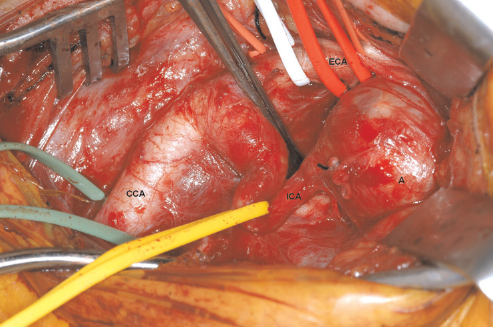
Operative photograph following mobilization of the carotid arteries and prior to aneurysm resection. CCA, common carotid artery; ICA, internal carotid artery; ECA, external carotid artery; A, aneurysm
Outcome
The patient recovered from anaesthesia without any neurological complications and was discharged three days later. Microbiological cultures of the aneurysm wall were negative. Histological examination revealed myxoid degeneration of the arterial wall.
Discussion
Extracranial carotid artery aneurysms are defined as localized increases in diameter of more than 50% compared with reference (ICA: men 0.55 ± 0.06 cm, women 0.49 ± 0.07 cm; bulb: men 0.99 ± 0.1 cm, women 0.92 ± 0.1 cm). 4 They usually involve the CCA or ICA with ECA lesions being exceptional. 5 The majority of true aneurysms are most commonly described as atherosclerotic or degenerative but other causes are arterial dissection, fibromuscular dysplasia, infection and neck irradiation.1,6,7 They have also been described in association with systemic disorders such as neurofibromatosis, Marfan's syndrome, Behçet's disease, Takayasu's arteritis and type IV Ehlers–Danlos syndrome.8–12 In older series, a significant number of cases are pseudoaneurysms, complicating endarterectomy due to synthetic patch infection or silk suture degeneration. 6 While post-endarterectomy cases are declining as a result of prophylactic antibiotics and modern monofilament sutures, pseudoaneurysms following blunt and penetrating trauma are increasing. 2 Modern case series find a male/female sex ratio of 2:1 and the average age of patients is around 55 years, significantly lower than those with atherosclerotic stenoses.3,13
Like any other aneurysm, they may present as a result of embolization, rupture, compression of adjacent structures or as a pulsatile mass. Rupture is very unusual and most present with transient ischaemic attacks (TIA) or ischaemic strokes from cerebral embolization or with a lump in the neck.1,2,6 Local symptoms from cranial nerve compression and/or mass effect include dysphagia, dysphonia, dyspnoea/stridor and tinnitus. 6 On examination, a pulsatile mass may be palpable externally in the neck or protruding into the pharynx, but only in a minority of patients.2,7 A thrill or bruit may also be detected. Neurologically, an ipsilateral Horner's syndrome may be present in addition to signs from local cranial nerve palsy or cerebral infarction. 14
Carotid US has a high sensitivity for stenotic disease which occurs principally in the bulb and proximal ICA. 15 However, the location of ICA aneurysms depends on their underlying aetiology, with those due to fibromuscular dysplasia, spontaneous dissection or trauma tending to lie above the level of the angle of the mandible and degenerative/atherosclerotic lesions occurring more proximally towards the bifurcation.2,16 In one series, only 8/25 aneurysms were detected by US due to a high proportion of lesions being located at or above the angle of the mandible, a difficult area to examine with US.2,3,7 Techniques to image this segment may include a more lateral or posterior transducer position, cephalad angulation of a transversely oriented transducer and the use of curvilinear, lower frequency transducers. Despite these techniques, some authors still advocate CT imaging in all patients with a normal carotid US examination following TIA. 7
The relationship between the aneurysm and skull base can be difficult to determine on intra-arterial angiography and has resulted in CT becoming the most common imaging modality used to plan intervention.3,7 Even if a more proximal aneurysm is visible with US, the appreciation of complex 3D structures from 2D images is difficult. Applications for 3D US are improving and are beginning to address some of these difficulties. However, most surgeons still prefer to plan surgical reconstruction from intra-arterial, CT or magnetic resonance angiograms.
The dominant indication for treatment is the prevention of neurological complications by removing the embolic source. This can be performed by open surgical intervention or by endovascular radiological techniques. At open surgery, the aneurysm is usually resected and vascular continuity is restored with direct anastomosis of the remaining arteries, transposition of the ECA to distal ICA, placement of a synthetic or venous interposition graft or rarely ICA ligation. 2 , 16 – 18 Ligation of the ICA should be performed only as a last resort because it results in stroke in about 50% of patients and death in 20%.3,13 Aneurysmorrhaphy has also been described and involves excision of the redundant aneurysm wall and closure of the artery, often with a Dacron or venous patch.1,6 This technique has been advocated for extensive fusiform aneurysms where resection runs a higher risk of cranial nerve injury. 6 Infected synthetic patches are usually treated by their removal and arterial closure with the saphenous vein.
Endovascular intervention avoids the need to surgically expose carotid arteries. As a result, cranial nerve injury risk is lower but there remains a risk of stroke. 19 Two techniques are available. First, the aneurysm may be ‘re-lined’ with a stent graft to exclude the sac from the rest of the circulation. Second, a saccular aneurysm may be thrombosed with embolization coils. 17 Experience is limited to small case series but the use of endovascular interventions is likely to expand, particularly for distal lesions.
In conclusion, the identification of extracranial ICA aneurysms before significant complications can ensue allows the opportunity of successful repair. Sonographers should be aware of this rare condition and maintain a high index of suspicion, particularly in younger patients presenting with cerebral embolic disease.