
Abstract
A 64-year-old man with histologically proven autoimmune pancreatitis and membranous nephropathy presented for evaluation of suspected liver metastases on computed tomographic abdominal scan. Ultrasound, contrast-enhanced ultrasound and visceral angiography demonstrated multiple hepatic artery aneurysms. Coil embolization of the largest aneurysm was undertaken successfully. The investigative findings indicate that necrotizing vasculitis was the underlying process, resulting in aneurysm formation. There is evidence that the smaller aneurysms have been effectively treated conservatively with immunosuppressive therapy.
Case report
A 64-year-old male patient re-presented to us following an abnormal review computed tomographic (CT) scan (Figure 1) carried out in an external unit, the report suggesting that the multiple focal liver lesions detected might be metastatic in nature, from an occult primary malignancy.
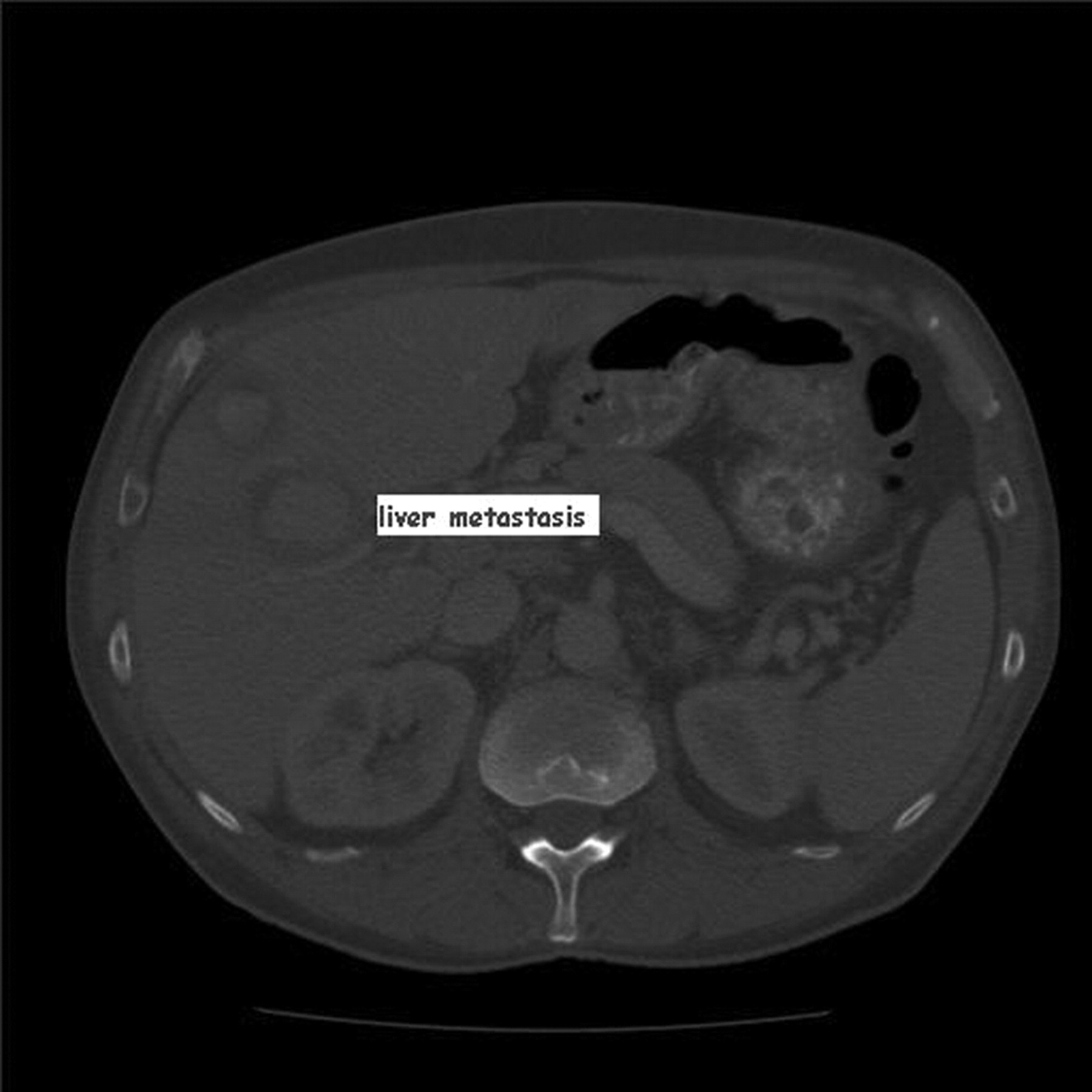
Computed tomography image interpreted as suspected liver metastases
This patient had been under our care previously from August 2007, being reviewed every three months given his diagnosis, ab initio, of autoimmune pancreatitis and membranous nephropathy with proteinuria up to 15 g/L (<20 mg/L). Screening for malignancy, including CT, gastrointestinal endoscopy and bone marrow biopsy at that time had been negative. On his most recent general medical visit he was asymptomatic on physical examination. Routine haematological and biochemical profiles were normal.
In January 2009 ultrasound examination of the liver had reported no abnormality.
On the index ultrasound examination (Toshiba Aplio Japan, 3.5 MHz, MI 0.06) multiple hypoechoic masses in nearly all liver segments were detected, the largest measuring 49 mm in diameter (Figure 2). The smaller lesions were around 20 mm in diameter.
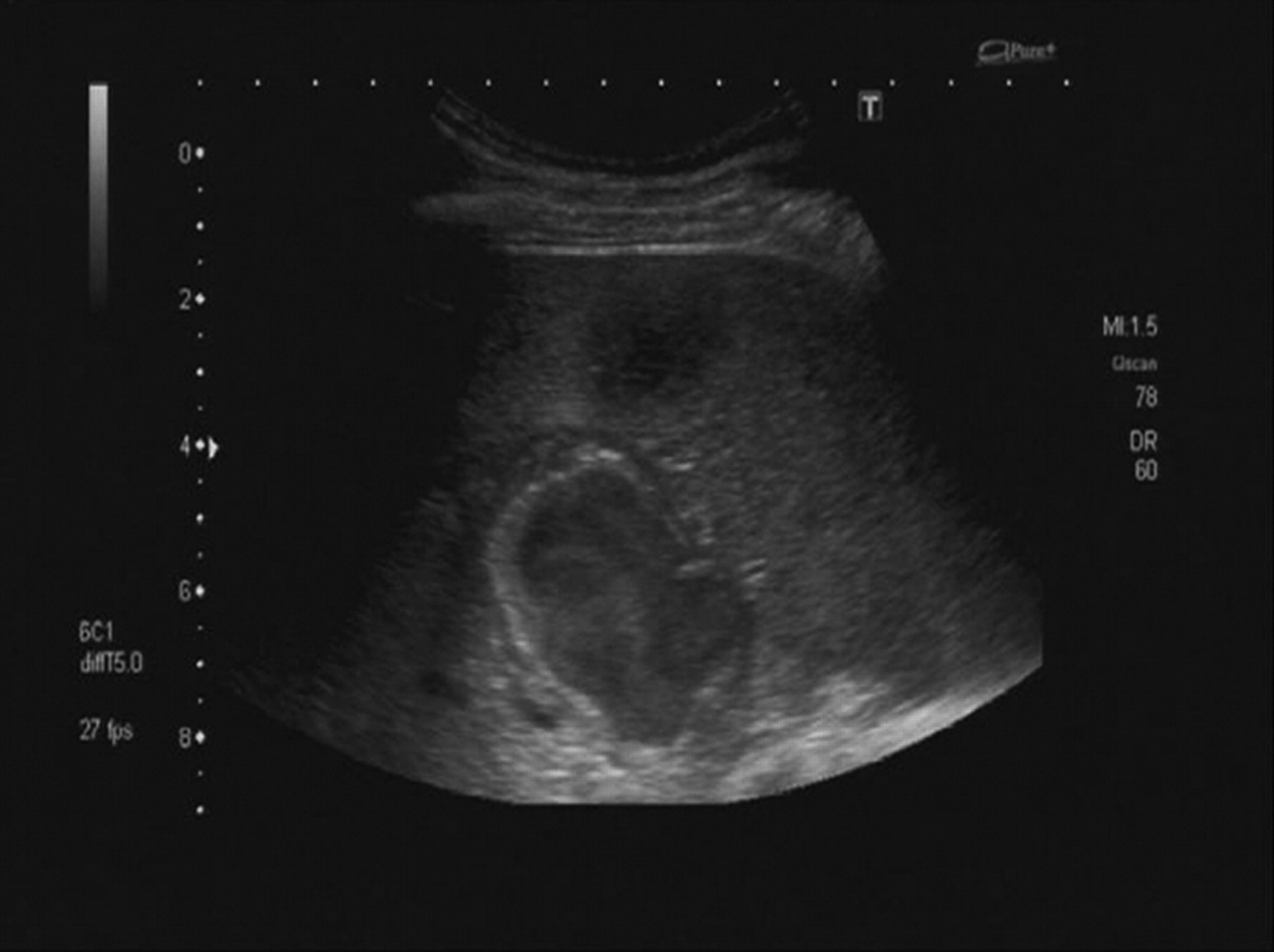
Baseline B-mode image of the largest aneurysm arising from the right hepatic artery prior to therapy
Colour Doppler (Figure 3) and contrast-enhanced ultrasound (CEUS, contrast agent: Sonovue™ 2.4 mL) (Figure 4) revealed pulsatile and turbulent arterial flow into and within the majority of the lesions.
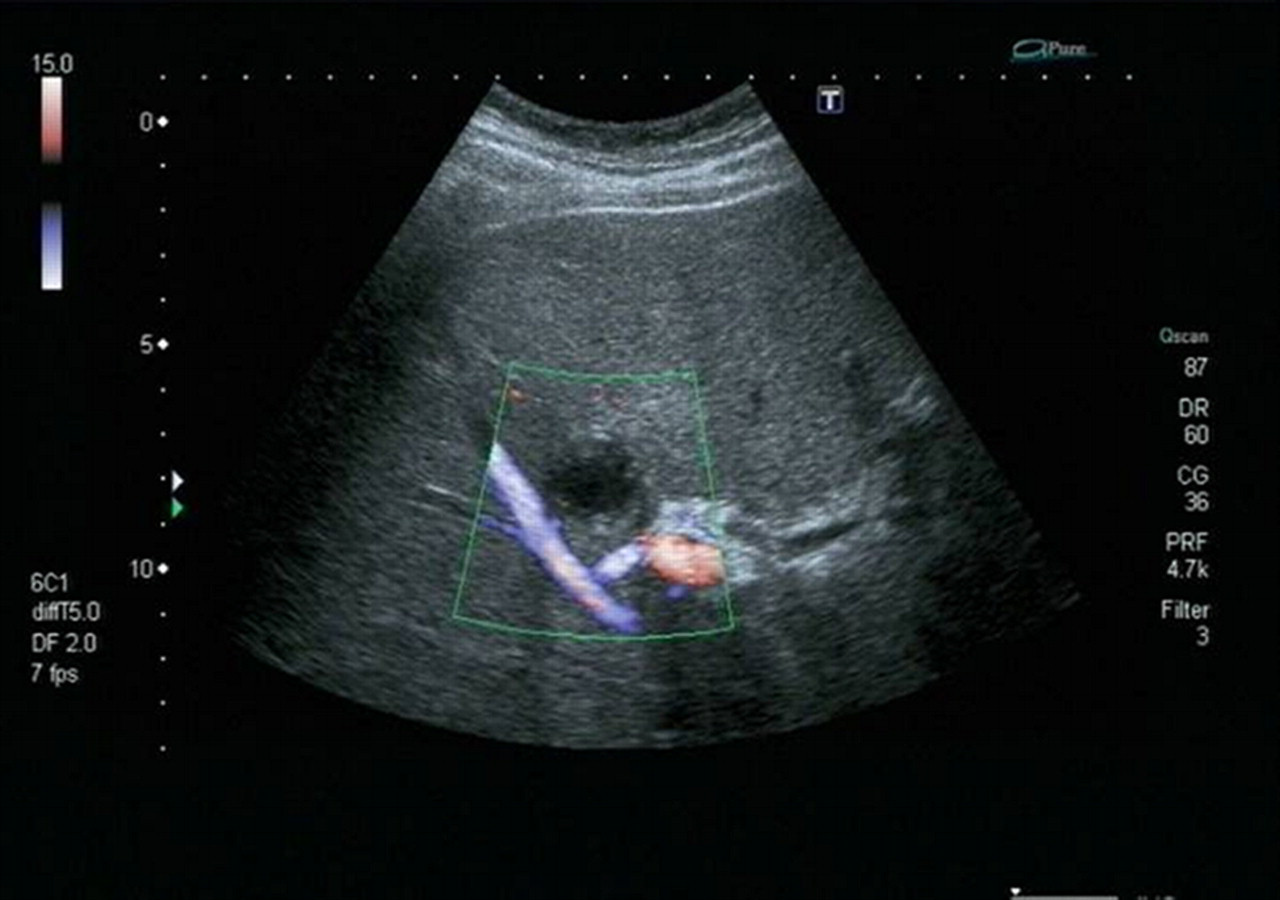
Colour Doppler image of aneurysm

(a) Angiographic findings after selective visceral angiography of the hepatic arteries. (b) Selective angiography after coiling the largest aneurysm, with consent of Dr Wiskirchen
To further elucidate the diagnosis of multiple aneurysms of the hepatic artery we carried out selective visceral angiography (Figure 5). Additionally at the time of the diagnostic angiogram, the largest aneurysm originating from the central right hepatic artery was subject to coil embolization using two coils (Cook Medical). No other therapeutic coil embolization was performed.
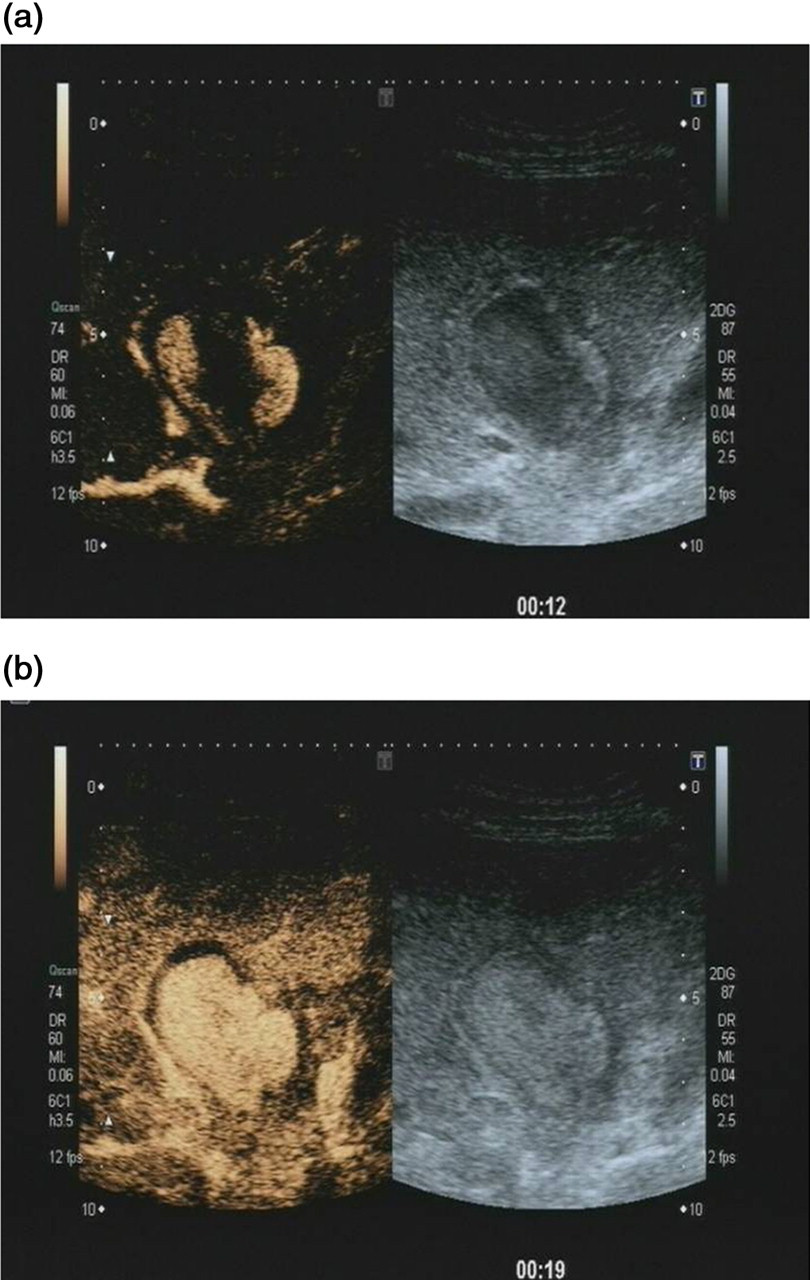
Contrast enhanced ultrasound images: (a) 12 seconds and (b) 19 seconds after infusion of the contrast agent (Sonovue 2.4 mL)
No other aneurysms were seen outside the liver using Doppler sonography, CT and magnetic resonance imaging (MRI).
Ultrasound-guided biopsy of the hypoechoic margin of the lesion was performed 48 hours after coil embolization. Histologically, three distinct layers of change were noted, namely thrombosis, scar tissue and infiltration with eosinophilic granulocytes (Figure 6). Infiltration with eosinophilic granulocytes was similar to the cytological findings on pancreatic biopsy. The previous renal biopsy, however, did not reveal any features in concordance with the current liver lesion biopsy appearances.

Histological image from the margin of the lesion: three distinct layers of change were noted with consent of Prof Dr Raute
Given the patient's recent course, histological findings with eosinophilic infiltration, increased blood/serum eosinophils and immunoglobulin values, this indicated an aetiology of autoimmune/allergic inflammatory granulomatosis or necrotizing vasculitis as the underlying process resulting in aneurysm formation.
We commenced immunosuppressive treatment with prednisolone and azathioprine. The prednisolone dose was reduced from 60 to 10 mg for maintenance, while increasing the azathioprine gradually up to 125 mg dosage level.
Surveillance using periodic ultrasound, particularly with the consistency of findings on CEUS, is documenting a reduction in size of the aneurysms alongside a trend towards thrombosis in the uncoiled lesions, due to the presumed efficacy of immunosuppression. In the follow-up evaluation of this case we employ CEUS rather than CT. CEUS avoids the use of ionizing radiation and is more pathophysiologically informative in these circumstances.
Discussion
Visceral artery aneurysms are uncommon with an estimated incidence of 0.1% but they represent a clinically important grouping. 1–4 The hepatic artery is the fourth commonest site of intra-abdominal aneurysm, representing approximately 20% of all visceral aneurysms. Most (80%) are extra- and 20% are intrahepatic, and 4% involve both right and left hepatic arteries. 5–7 In many cases they remain undetected up to the time of rupture due to lack of specific symptomatology. 2,7
There are various aetiologies of hepatic artery aneurysms; most frequently they result from atherosclerosis (30%) and fibromuscular dysplasia (24%).
Less commonly they occur in necrotizing vasculitis, allergic granulomatosis, post-liver transplantation and hepatic tumour. 7–9
The increased use of non-invasive imaging techniques such as ultrasound and MRI reveals these aneurysms during the asymptomatic period, thereby assisting in choosing early and appropriate treatment options. 2
Ultrasound is established as a non-invasive method for detecting these aneurysms, which are revealed as masses of mixed echogenicity varying in their proportions of cystic and solid components depending on the extent of thrombosis. Colour Doppler ultrasound and CEUS can differentiate aneurysms from other vascular abnormalities such as arterio-venous fistulae.
The full evaluation of hepatic artery aneurysms requires detailed interventional angiographic input, which confirms diagnosis and identifies other aneurysms.
Elective treatment is indicated if the diameter of the aneurysm is >2 cm due to the increased risk of rupture. 4
The surgical approach remains an option, but catheter embolization is preferred for aneurysms located intrahepatically. 10 Regression of arterial aneurysms, for example in cases of necrotizing vasculitis following immunosuppressive treatment, has already been described in the literature. 11 This reported reduction in size of the aneurysms, and tendency to thrombosis (particularly so in smaller aneurysms) was mirrored during the care of our patient. Beside clinical parameters, ultrasound, including CEUS, is an important diagnostic tool for monitoring the further course of disease.