
Abstract
Ultrasound is the imaging modality of choice in the delineation of scrotal pathology and readily differentiates testicular from extratesticular disease. Primary testicular malignancy is widely recognized; metastatic disease within the testes is a relatively unusual occurrence arising most frequently in patients with lymphoma or disseminated prostate or bronchial cancer. Testicular metastases secondary to malignant melanoma is a particularly rare finding, which is invariably confined to postmortem examinations. We present the ultrasonic appearances of a rare case of malignant melanoma with bilateral testicular metastases which arose during the course of the illness.
Case history
An 80-year-old man presented with a changing pigmented lesion on the upper, anterior abdominal wall. This was fully excised and histology confirmed superficial spreading malignant melanoma. After a period of three months, he developed several cutaneous lesions that were confirmed on biopsy to be metastatic melanoma. Re-staging investigations six months following the initial diagnosis demonstrated diffuse disease in the skin, lungs, peritoneum and axillae. A solitary, asymptomatic brain metastasis was also present. At this stage, the man developed bilateral testicular masses, on a background of chronic bilateral hydrocoeles. Scrotal ultrasound (Philips 5000 [ATL]; L12-5 transducer – standard small part settings; Doppler optimized to low-velocity settings – velocity scale 4.4 cm/s) demonstrated multiple, irregular hypoechoic lesions throughout both testicles with hypervascularity on colour Doppler imaging in keeping with bilateral metastatic deposits (Figures 1 and 2).
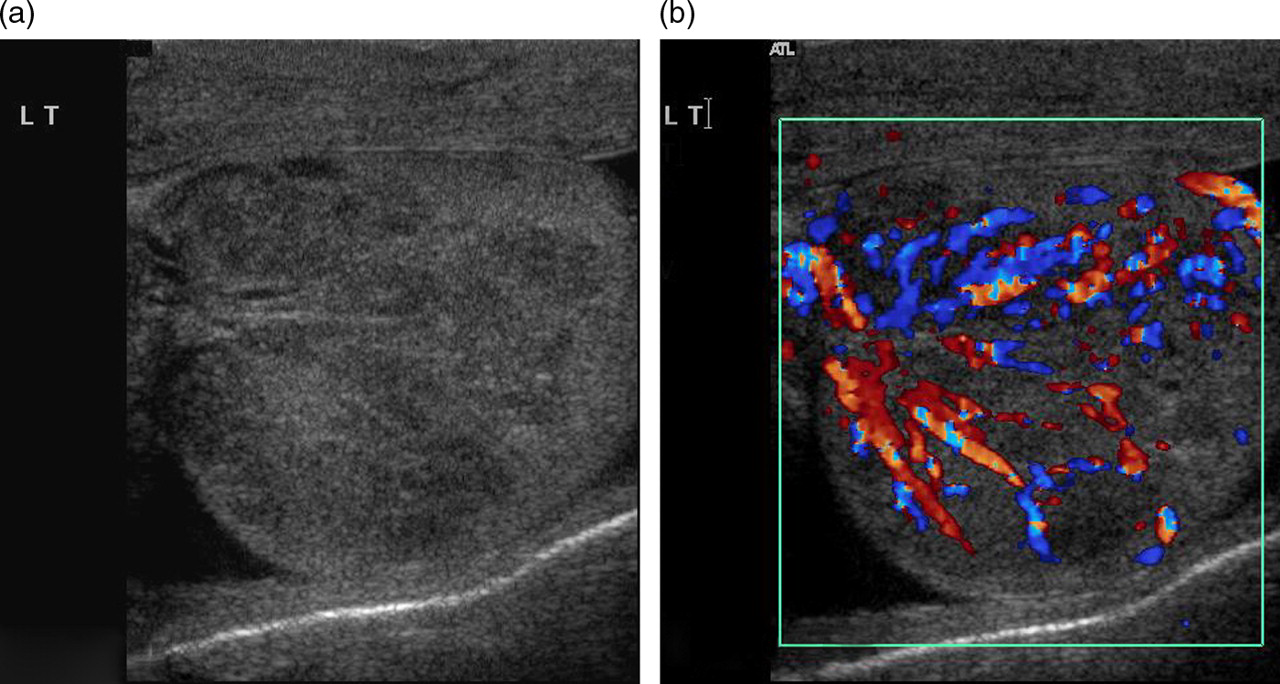
(a) Transverse B mode longitudinal image of the left testicle demonstrating multiple hypoechoic lesions highly suspicious of tumour deposits. (b) Corresponding colour Doppler image illustrating hypervascularity of the abnormal hypoechoic areas consistent with blood flow within areas of tumour infiltration

(a) Transverse view of right testicle demonstrating multiple focal hypoechoic regions with similar ultrasonic appearances to those in the contralateral testis; bilateral disease confirmed. (b) Longitudinal colour Doppler image depicting hypervascularity of the tumour deposits within the right testicle
Throughout his illness, the patient had refused systemic therapy and died eight months following initial diagnosis from complications of his peritoneal disease.
Discussion
Melanoma is a malignant neoplasm derived from melanocytes and usually arises from the skin. The incidence has risen rapidly over the last two decades to become one of the most common cancers in young and middle-aged adults. The Scottish Melanoma Group demonstrated an incidence per 100,000 of population in 1998 of 10.6 for men and 13.1 for women. 1 Caucasian women are at greatest risk, with positive family history and sun exposure representing important contributory factors.
Initial diagnosis is primarily based upon clinical examination with subsequent skin lesion biopsy and histopathological assessment. According to recent UK guidelines, the use of radiological imaging should be reserved for patients with an intermediate to high risk of disease recurrence (minimum of Stage IIb disease: tumour depth 2–4 mm without ulceration or >4 mm with ulceration), with the type of investigation being directed by patient symptoms. 2
The most common sites of metastatic disease are regional lymph nodes, skin, lung, head and neck, the eye and the liver. Disease spread to the genitourinary tract is also recognized, with melanoma representing the third most frequent tumour metastasizing to the kidney. 3
Overall, metastatic disease involving the testes is a relatively unusual occurrence and most frequently exists in the context of widely disseminated malignancy. Invariably, these lesions are discovered at postmortem examination, having been a subclinical abnormality during the course of illness. However, in a small proportion of cases, metastatic testicular lesions are discovered clinically in patients with known malignancy, although such lesions representing the initial clinical presentation of an extratesticular malignancy is particularly rare. 4 The frequency of individual tumours metastasizing to the testes is highly variable. Review of the literature yields little definite agreement, although lymphoma appears to be the most common primary tumour, spreading to the testes in less than 3% of cases. 5 These patients are also more likely to have diffuse bilateral gonadal disease. Secondaries from prostate and bronchial malignancies are also documented, accounting for approximately 35% and 20%, respectively, of testicular metastasis cases in one review. 6
The incidence of testicular melanoma metastases appears to vary widely, ranging from 2% in one case series of 248 patients to 41% in a 22 patient cohort. 7,8 Although invariably observed at autopsy (13–23% in one study 9 ), testicular metastases can become apparent during the course of disease, as an incidental finding or less commonly as the presenting metastatic site. Reported cases of testicular metastases secondary to melanoma include testicular disease which has been unilateral, bilateral, unifocal and multifocal. 6,9 In the majority of series, testicular deposits are associated with synchronous or metachronous metastases elsewhere.
In this particular case, the testicular abnormality became symptomatic during the course of the patient's illness, some six months after the initial diagnosis of malignant melanoma. Based on clinical examination findings, an ultrasound scan of the scrotum was performed which demonstrated multiple ill-defined, hypoechoic lesions replacing normal testicular parenchyma (Figures 1a and 2a). Diffuse and focal deposits were identified throughout both testicles, with generalized hypervascularity on colour Doppler imaging (Figures 1b and 2b). Appearances were deemed most likely to represent diffuse bilateral metastatic disease, which was proven on subsequent pathological analysis.
While the characterization of testicular lesions based on ultrasound appearances alone has been proposed, this is not a reliable approach given the wide ranging appearances of malignant testicular lesions on ultrasound and histology is invariably required. Admittedly, in this particular case the imaging features were thought to be most indicative of malignancy, with the diffuse and infiltrating nature of the deposits being a major factor in this assessment. Clearly, solitary or focal testicular lesions can present a greater diagnostic challenge and subsequent pathological correlation should always be sought.
The patient's reluctance to undergo systemic therapy following initial diagnosis will almost certainly have contributed to the degree and extent of his metastatic disease – it is unclear as to whether such therapy would have prevented the testicular disease from manifesting as a clinical finding during the course of the illness.
Conclusion
Ultrasound is an invaluable tool in the assessment of suspected testicular abnormalities. Its superb spatial resolution is ideal for identifying focal disease, which may be primary or secondary. In patients with uni- or bilateral testicular changes in whom there is a known primary lesion, metastatic testicular disease is rare but should be considered. Despite being well-recognized in other malignancies such as lymphoma, testicular metastases secondary to malignant melanoma is a very rare finding, which is not just confined to postmortem examinations.