
Abstract
This case report describes the unusual condition of Lemierre's syndrome diagnosed in the first trimester of pregnancy. The diagnosis was made by ultrasound and magnetic resonance imaging. The patient was treated with intravenous antibiotics and was anti-coagulated.
Case
A 37-year-old para 1 woman presented to the obstetric department at nine weeks gestation with a two-week history of vomiting, painful neck swelling and fever. Her only past medical history was a partial tonsillectomy in childhood.
On presentation she was pyrexial and tachycardic but normotensive. Examination revealed tender swelling in the anterior triangle of the right side of the neck with bilateral enlargement of the tonsils. There were no otological symptoms and examination of the ear was normal. Blood was taken for culture, blood count and C-reactive protein (CRP). The white cell count was 12.3 × 109/L while the CRP was markedly raised at 233 mg/L.
She was admitted and treated with intravenous fluids and broad-spectrum intravenous antibiotics.
An ultrasound of the neck demonstrated tender lymphadenopathy in the right anterior triangle of the neck, but no focal abnormalities within the adjacent glands or fluid collection (Figure 1), and further cross-sectional imaging was advised in light of the clinical picture. Pelvic ultrasound confirmed a viable pregnancy.
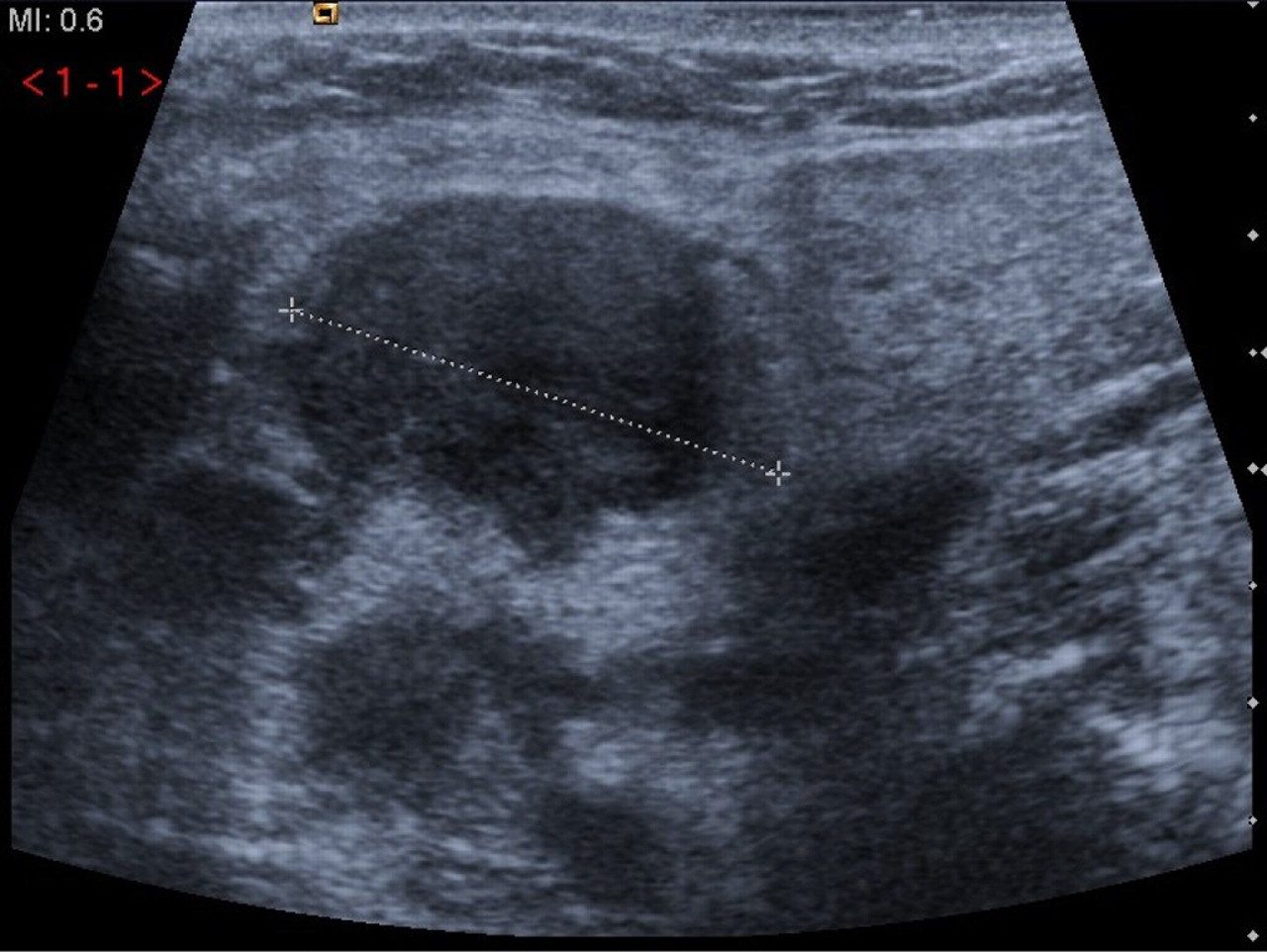
Ultrasound showing 22 mm right digastric node
Over the following 24 hours, the pyrexia settled but the neck swelling increased and she developed headache and odynophagia. Her case was discussed with ears, nose and throat (ENT) team. Magnetic resonance imaging (MRI) of the neck demonstrated diffuse soft tissue swelling and adenopathy on the right side of the neck, subsequent obstruction of the right internal jugular vein with thrombus (Figures 2 and 3), and soft tissue swelling involving the anterior mediastinal fat, consistent with mediastinitis (Figure 4). The internal jugular thrombosis, radiological evidence of distant metastatic infection, and clinical signs and symptoms confirmed the diagnosis of Lemierre's syndrome.
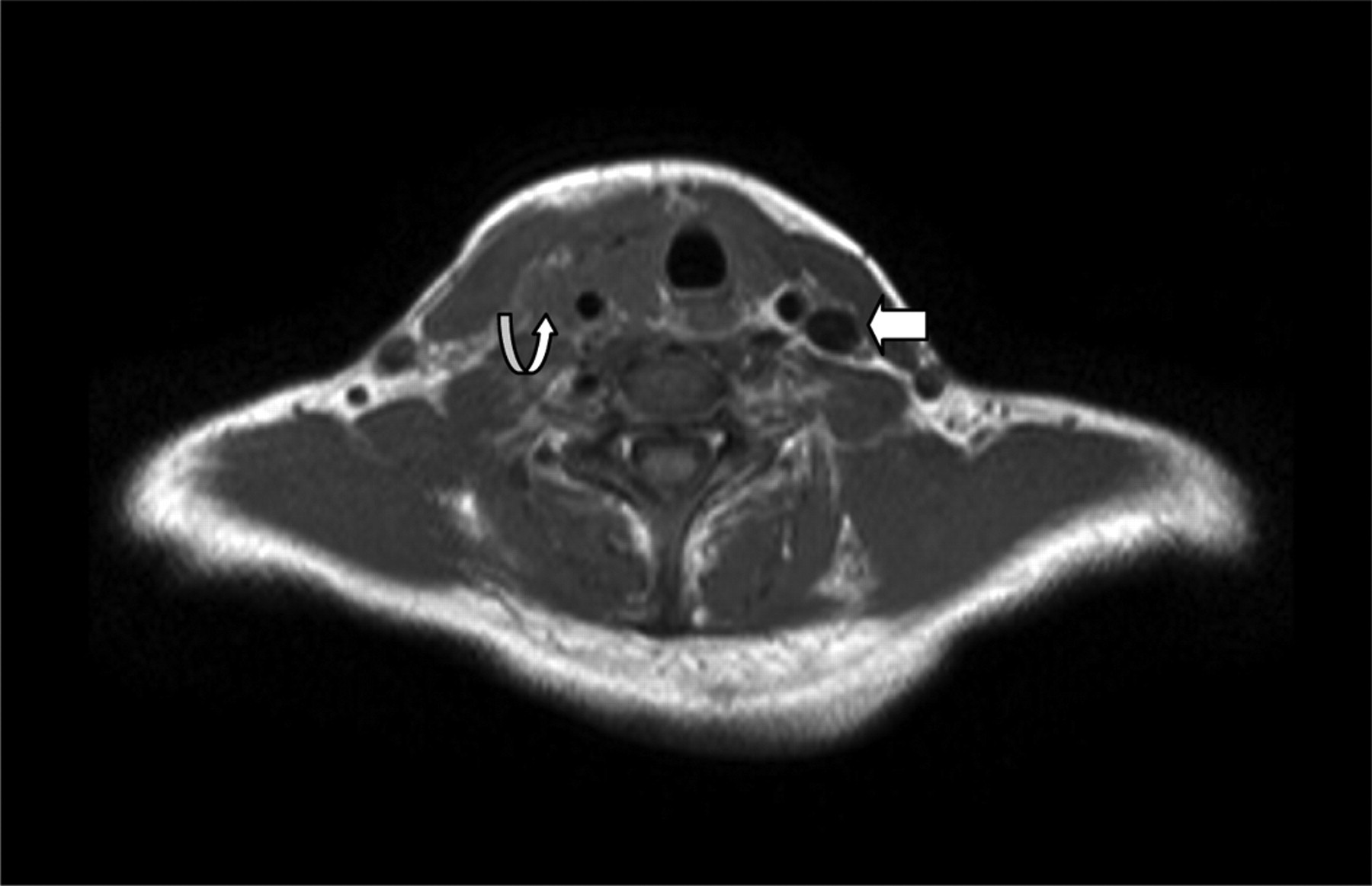
MRI, axial T1 weighted, showing patient's left internal jugular vein (arrow) and thrombosed right internal jugular vein (curved arrow). MRI, magnetic resonance imaging

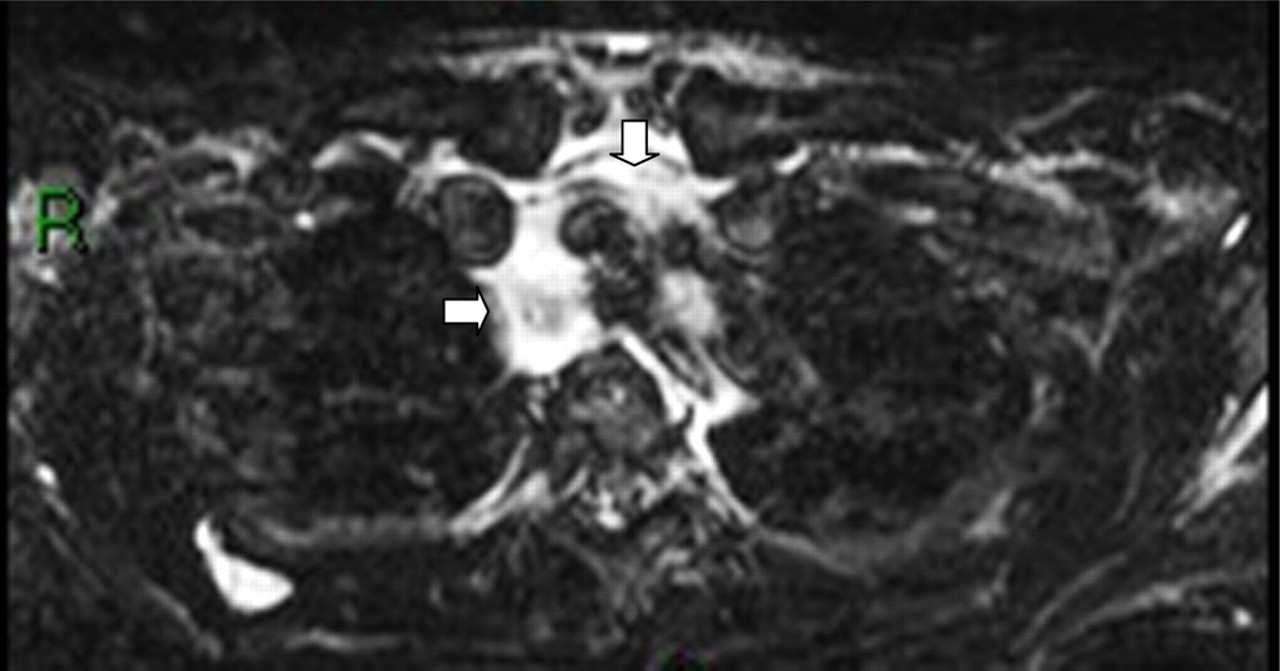
MRI axial STIR (short TI inversion recovery), showing extensive right-sided adenopathy and soft tissue oedema (curved arrow). MRI, magnetic resonance imaging
MRI axial STIR showing oedema and inflammatory change in the mediastinum (arrows). MRI, magnetic resonance imaging; STIR, short TI inversion recovery
Direct visualization by ENT at endoscopy demonstrated bilateral swelling and erythema of the tonsils, with no other focus of infection.
Streptococcus pyogenes grew on blood cultures and due to the risk of propagation/extension of infection locally, the antibiotic regimen was changed to intravenous benzylpenicillin and metronidazole.
The patient was transferred to High Dependency Unit for monitoring due to the risk of acute airway obstruction and treatment with intravenous unfractionated heparin was commenced because of the risk of thrombotic embolus. Due to her ongoing headache, computed tomography (CT) venogram was performed. This confirmed venous patency above and below the level of the thrombus and excluded intra-cranial complication (Table 1). Her oxygen saturation remained satisfactory and at no point did she complain of chest pain.
Radiological features of Lemierre's syndrome
Over the following two weeks she improved clinically. Her pyrexia settled, and the neck swelling and pain resolved. She was changed to treatment dose subcutaneous enoxaparin, which was continued until six weeks postpartum. Intravenous antibiotics were converted to oral after 14 days.
Discussion
Lemierre's syndrome was first reported by Courmont in 1900 1 and subsequently named by Lemierre 2 in 1936. This unusual disorder is most commonly seen in teenagers and young adults. Four criteria are used for diagnosis (Table 2).
Diagnostic criteria for Lemierre's syndrome
Before the introduction of antibiotics, Lemierre's syndrome was common, with a mortality rate of 90%. 3 It is now described as ‘the forgotten disease’, with an incidence of only 0.8 per million. 4 From 1974 to 1989, only 23 cases were reported worldwide. 4 Interestingly, a recent resurgence in Lemierre's syndrome has occurred with increasing numbers of published reports since the 1990s. 5 It has been suggested that this may be due to a growing reluctance of doctors to prescribe antibiotics for sore throats. 5
The diagnosis of jugular vein thrombosis and distant septic metastasis, and hence Lemierre's syndrome, relies heavily on cross-sectional imaging such as CT and MRI. Although ultrasound can be a useful non-ionizing method of assessing venous patency and inflammatory change, it does have limitations. General soft tissue swelling may attenuate the vein and hinder assessment of compressibility, and fresh, hypoechoic thrombus may be difficult to appreciate. See Table 1 for local ultrasound features of Lemierre's syndrome.
Contrast-enhanced CT of the neck and chest is, however, gold standard in the diagnosis of Lemierre's syndrome. Its major benefit is its sensitivity and ability to identify additional pathologies, which may be secondary to metastatic infection. Complications may arise from the local spread of infection in the form of parapharyngeal or paratracheal abscesses, as a result of septic micro emboli resulting in distant sepsis in the lungs, joints, soft tissues or abdomen or due to thrombotic complications. 5
Blood cultures usually reveal a commensal bacterium, Fusebacterium necrophorum; however, other anaerobes including streptococci and bacteroides have been reported. 6
There are no definitive management guidelines in the literature. Previous cases have been managed using extended courses of intravenous broad-spectrum antibiotics. Traditionally, penicillin was the agent of choice but beta-lactamase producing penicillin-resistant strains have since been isolated. 6 Consequently, combination antibiotics are now suggested as best practice.
The use of heparin to treat Lemierre's syndrome is controversial and many cases have been successfully treated without it. 6 Some studies suggest that anticoagulation may extend the infection. 7 The physiological changes that occur in pregnancy, however, result in a hypercoagulable state and, therefore, the risk of embolus in this case was significant.
Only two cases of Lemierre's syndrome in pregnancy have been reported in the literature. This is surprising, given that the condition is most common during the reproductive years. The first was in a 23-year-old who delivered a premature infant at 26 weeks gestation. 8 This case was, however, complicated by maternal pericardial tamponade and pericardial effusion. Studies have demonstrated that 13.6% of women who experience preterm labour have a positive amniotic fluid culture with Fusobacteria, so the possibility of a link between Lemierre's syndrome caused by Fusobacteria and premature labour may be significant. 9
The second case was a 23-year-old who presented at 22 weeks gestation with headache, cough and fever. 10 She was diagnosed and treated promptly. Fetal ultrasound examination suggested intrauterine growth restriction and she underwent induction of labour at 37 weeks gestation and gave birth to a healthy baby. 10 This case offers reassurance that good fetal outcomes can be achieved with prompt and appropriate treatment.
The presentation of life-threatening maternal conditions during pregnancy forces difficult diagnostic and therapeutic decisions to be made, as demonstrated by this case. Diagnosis of this syndrome has previously relied upon ionizing radiation which is best avoided or reduced, in pregnancy, and it is in this circumstance that ultrasound can be a valuable tool for both diagnosis as well as ongoing assessment during treatment.
As far as treatment is concerned, the fetal effects of many high-dose intravenous antibiotics are unknown and there is risk of intrauterine bleeding resulting in miscarriage, abruption, premature labour or intrauterine death with heparin. However, delaying treatment or providing suboptimal management carries significant risk to the mother on whom the fetus is entirely reliant.
In conclusion, although Lemierre's syndrome and its potential complications are a rare and serious condition, it is entirely treatable once the diagnosis is made. The potential fetal complications of both investigation and management must be considered while maximizing treatment for the mother, and it is vital that a diverse multidisciplinary team is involved. Ultrasound is very useful in initial assessment and diagnosis, especially in the pregnant patient, and the resurgence of this disease should be considered when imaging and treating unwell patients with otolaryngological symptoms.