
Abstract
I am writing in response to the article published in the February 2010 edition of Ultrasound, entitled ‘Let's all jump on the ultrasound bandwagon: further debate on the use of ultrasound’ by Hazel Edwards. 1
I agree with the author that ultrasound (US) is a useful adjunct for some clinicians, and it seems very easy to do. In fact, US is a very important tool for neonatolgists, particularly in a Neonatal Intensive Care Unit (NICU), for the diagnosis of cranial haemorrhage and for monitoring white matter damage. The interpretation of US images can sometimes be too subjective, for example the variable interpretation by different operators of cranial sonograms in premature babies for assessing white matter damage. Both inter-observer and intra-observer reliability and accuracy is a problem. 2,3 A possible solution is rigorous US training courses with high-level didactic methods (in Australia there is the Certificate in Clinician Performed Ultrasound). The quality of such courses can be maintained and improved by asking participants to complete feedback questionnaires. Second, regular ultrasound meetings in each NICU and among different NICUs is a perfect forum for discussing images, technique and cases.
In 2009, I organized an international neonatal ultrasound course in Italy, which included abdomen, brain and urogenital tract in the newborn. The course was aimed at paediatricians, neonatologists and paediatric radiologists. The lecturers were three paediatric radiologists from Austria, France and the USA. Participants were invited to complete a short anonymous questionnaire at the beginning of the course so that I could gauge their level of US experience. There were 47 doctors (10 paediatric radiologists, 37 paediatricians/neonatologists) from 11 European countries including Portugal, Spain, Italy, Norway, Macedonia, Estonia, Greece. Twenty-six (55%) were experts (more than three years ultrasound experience), 16 (34%) were less experienced (1–2 years) and five (11%) had no experience.
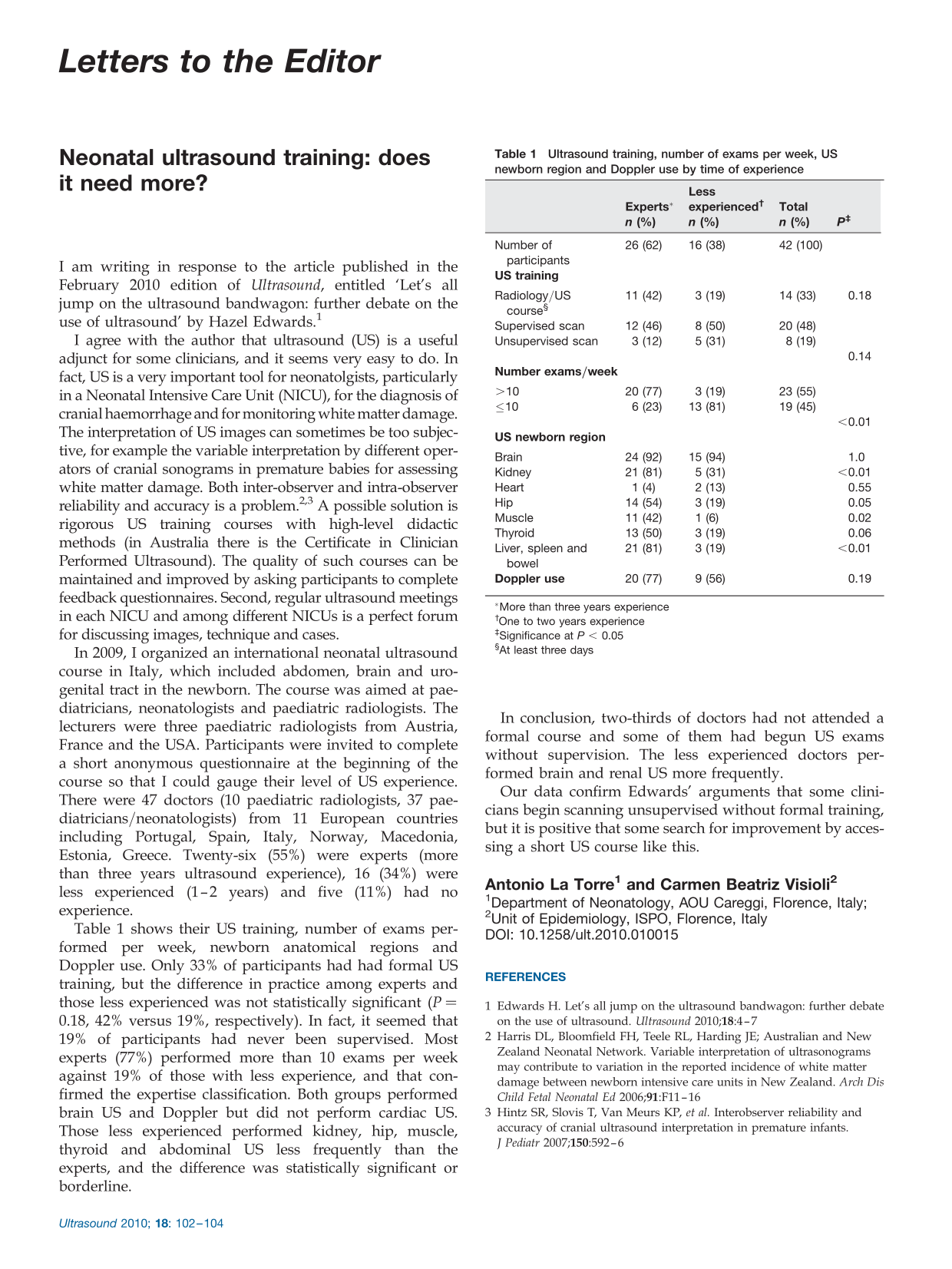
Table 1 shows their US training, number of exams performed per week, newborn anatomical regions and Doppler use. Only 33% of participants had had formal US training, but the difference in practice among experts and those less experienced was not statistically significant (P = 0.18, 42% versus 19%, respectively). In fact, it seemed that 19% of participants had never been supervised. Most experts (77%) performed more than 10 exams per week against 19% of those with less experience, and that confirmed the expertise classification. Both groups performed brain US and Doppler but did not perform cardiac US. Those less experienced performed kidney, hip, muscle, thyroid and abdominal US less frequently than the experts, and the difference was statistically significant or borderline.
Ultrasound training, number of exams per week, US newborn region and Doppler use by time of experience
*More than three years experience
†One to two years experience
‡Significance at P < 0.05
§At least three days
In conclusion, two-thirds of doctors had not attended a formal course and some of them had begun US exams without supervision. The less experienced doctors performed brain and renal US more frequently.
Our data confirm Edwards' arguments that some clinicians begin scanning unsupervised without formal training, but it is positive that some search for improvement by accessing a short US course like this.