
Abstract
Working hours of UK trainee doctors have recently been reduced to 48 hours per week, reducing exposure to clinical cases. As such, there is widespread acceptance that trainees need to train in environments other than the ward or operating theatre in order to gain practical skills. Formalin-fixed cadavers demonstrate gross muscle and nerve anatomy but needle insertion under ultrasound guidance is poor. In contrast, a new development in medical simulation is the use of Thiel-embalmed cadavers, developed by Professor Thiel of the University of Graz, Austria, using a novel preservation technique that retains full flexibility of the limbs. Thiel cadavers have been used to successfully simulate laparoscopic surgery, neurosurgery and oral surgery. This paper investigates, for the first time, the application of ultrasound-based regional anaesthesia to the Thiel cadaver by tracing the course of peripheral nerves, injecting local anaesthetic around nerves, and reproducing inadvertent intraneural injection by injecting preservative directly into the nerve. The Thiel cadaver provides good conditions for anaesthetists to simulate regional anaesthetic block techniques using ultrasound.
Regional anaesthesia is the subspecialty of anaesthesia concerned with nerve blocks and extended postoperative pain relief. Nerve blocks performed with needles under ultrasound guidance provide excellent long-lasting postoperative pain relief, 1 and contribute to accelerated rehabilitation and improvements in quality of life. However, the side-effects of regional anaesthesia may be traumatic and long-lasting. Inadvertent intravascular injection may result in convulsions or cardiac arrest, while intraneural injection may lead to permanent nerve damage and loss of function. 2 Acquiring the level of skill necessary to provide these benefits and avoid side-effects requires a great deal of clinical experience; subspecialty training in regional anaesthesia should develop appropriate knowledge, attitudes and skill, such that at the end of a 12-month fellowship, a trainee should be capable of independent regional anaesthetic practice. However, many factors are preventing anaesthetic trainees from gaining sufficient clinical experience: European legislation has reduced trainee working hours to 48 hours per week, shift systems predominate and emergency cover is now directly supervised by consultants. Thus, there is widespread acceptance that trainees need to train in environments other than the ward or operating theatre in order to gain essential practical experience.
Understanding this, anaesthetists have looked for a suitable model on which to simulate the passive and dynamic components of nerve block such as nerve anatomy, needle movement, fascial penetration, perineural fluid injection and inadvertent intraneural injection.
One approach to the simulation of regional anaesthesia training is the use of cadaveric models in Anatomy Departments or Surgical Skills Centres. In fact, a bi-annual regional anatomy/ultrasound course is run at Ninewells Hospital & Medical School at the Cushieri Surgical Skills Centre, which is recognized by the European Society of Regional Anaesthesia for higher medical training. Nevertheless, training opportunities are still limited. Whereas formalin-fixed cadavers are useful in the gross demonstration of nerve anatomy, ultrasound images are poorer and access to nerves is restricted because the limbs and muscles are fixed.
A potential development in medical simulation is the use of Thiel-embalmed cadavers, developed by Professor Thiel of the University of Graz, Austria, using a novel preservation technique that retains full flexibility of the limbs. Thiel cadavers have been used to successfully simulate laparoscopic surgery, 3 neurosurgery 4 and oral surgery. 5 A recent study 6 has compared the suitability of fresh and Thiel bodies for ultrasound-guided regional anaesthesia of the cervical region. The present study extends this evaluation to more locations and a wider range of procedures.
The Centre for Anatomy and Human Identification, University of Dundee was the first unit in the UK to prepare Thiel cadavers, and, based on initial evaluations such as this, has decided to routinely adopt the Thiel embalming method for cadaver preparation.
As a consequence, an opportunity existed to assess their suitability for simulating regional anaesthesia. Therefore, the primary aim of this pilot project was to scan the brachial plexus, interscalene and sciatic nerves and compare the ultrasonic image quality with images obtained from student volunteers undergoing the same procedures. The secondary aims of the project were to trace the course of the nerves, mimic a regional block by injecting around the nerves and reproduce inadvertent intraneural injection by injecting preservative directly into the nerve.
Method
Scanning of two Thiel cadavers (F and H) was undertaken at the Centre for Anatomy and Human Identification, University of Dundee under the supervision of an anatomist (RE). Age at death was 76 years for F and 89 years for H. Before imaging, cadavers were placed in the same position as would be used in a live patient.
Scanning of nerves used the same probes used for clinical anaesthesia; scanning of the brachial plexus and interscalene region was performed with a 10–5 MHz linear probe, while scanning of the sciatic nerve was undertaken with a 9–3 MHz curvilinear ultrasound probe. To ensure sterility both probes were covered with a long sterile sheath. Images were recorded on a Zonare Ultra ultrasound machine (Zonare, CA). Once the best image site was identified and recorded, a regional block needle was inserted and Thiel's moistening solution injected around the nerves, in order to mimic regional block. Finally, this solution was injected into the sciatic nerve in order to mimic inadvertent intraneural injection.
Assessment
All structures were assessed for echogenicity, the ability to reflect incident sound waves. Ultrasonographic visibility of nerves was ranked using the Vienna score; an ordinal scale from 1 to 4 where 1 = internal structure of the nerve visualized; 2 = nerve visualized as circular or oval-shaped bright halo; 3 = nerve visualized as reflection determined by anatomy of the surrounding tissue; and 4 = anatomical position of the nerve shows no response to ultrasound beam.
Results
Positioning
Both cadavers allowed rotation of the neck for interscalene block, external rotation of the shoulder for brachial plexus block, and hip and knee flexion for sciatic block.
Image quality
The volunteer ultrasound image highlights the standard positions of the peripheral (brachial) plexus nerves around the axillary artery (Figure 1). Compared with this standard, the Thiel images were of good quality (Figure 2: cadaver F; Figure 3: cadaver H), as the internal structure of the nerve could be visualized. In both images the internal structure of the nerve can be visualized easily (Vienna score 1). In both cadavers, the radial nerve (at 6 o'clock), median nerve (at 9 o'clock) and musculocutaneous nerves (at 7 o'clock) are clearly seen. The axillary artery is hypoechoic. In cadaver H, fascicles can be clearly seen within the radial nerve.

Standard positions of the peripheral (brachial) plexus nerves around the axillary artery
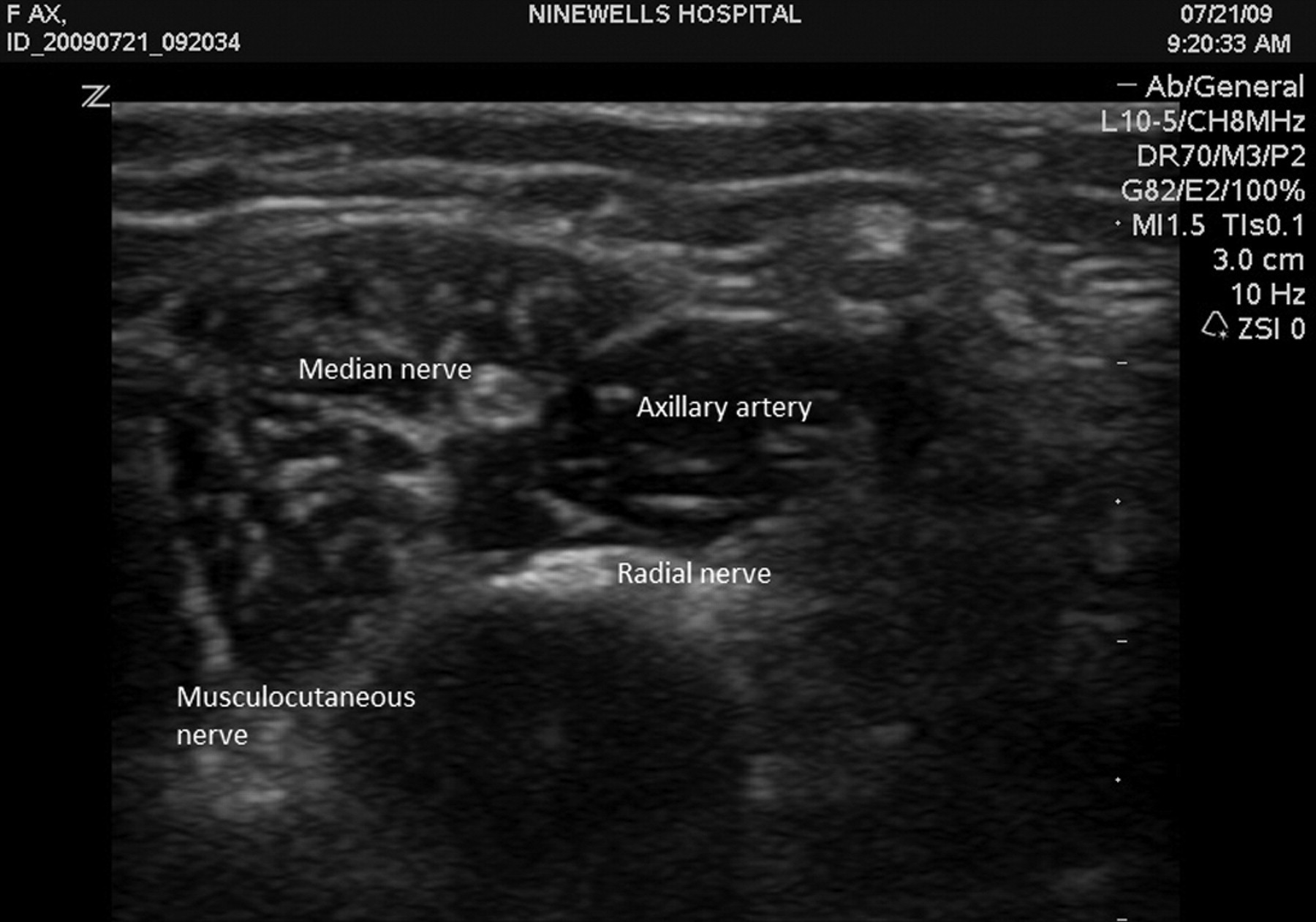
Cadaver F
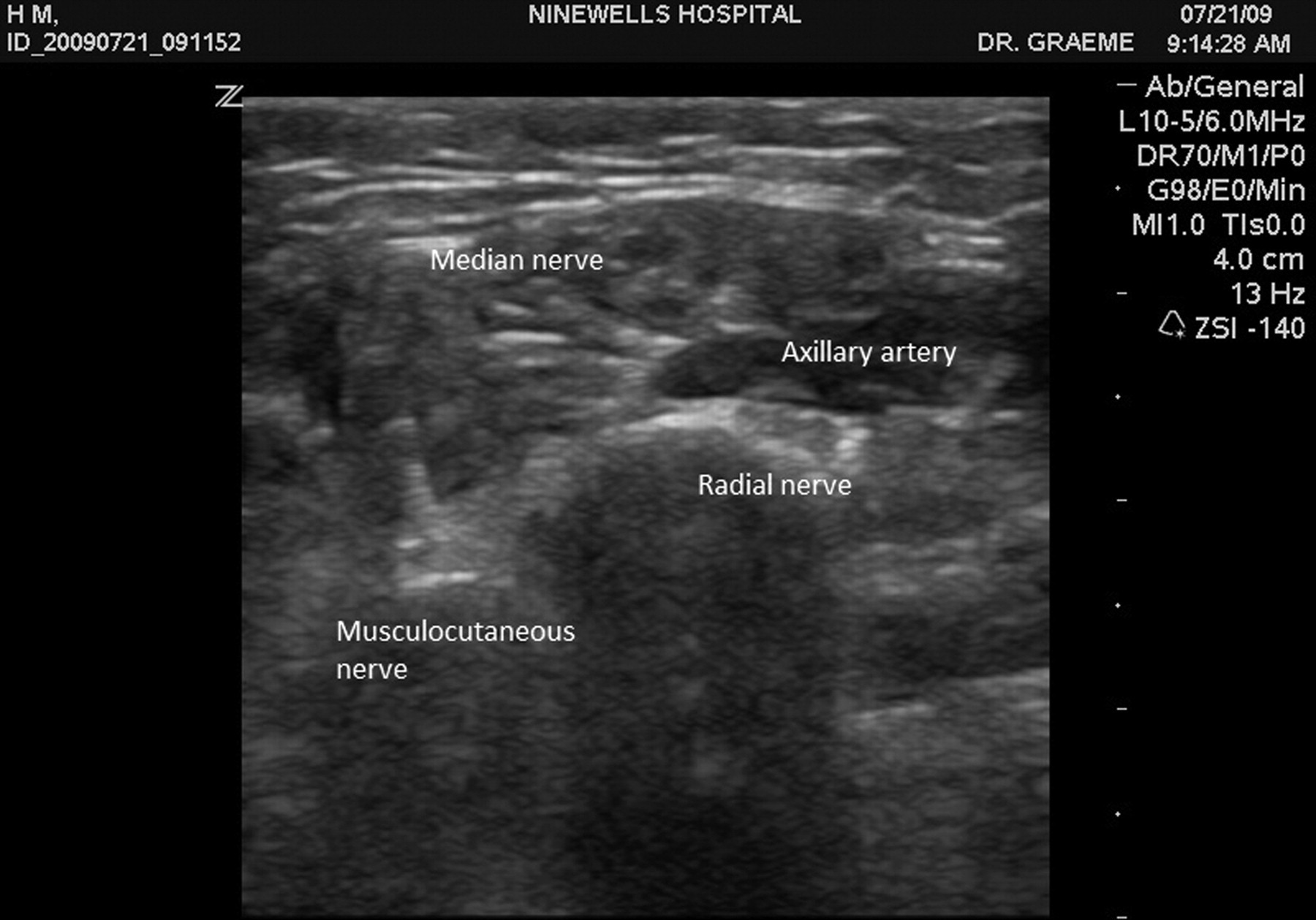
Cadaver H
Spread of solution
The volunteer interscalene image illustrates well the position of the roots and trunks of the brachial plexus between the scalene muscles (Figure 4). In contrast, in the Thiel cadavers (Figure 5) the anterior and median scalene muscles are difficult to see, although the image depth is 2 cm compared with the 3.5 cm of the volunteer. A round mass with three white dots is seen with dark areas spreading medially and laterally and can be graded as Vienna score 2. Injection splits the middle and inferior trunks of the brachial plexus.

Position of the roots and trunks of the brachial plexus between the scalene muscles
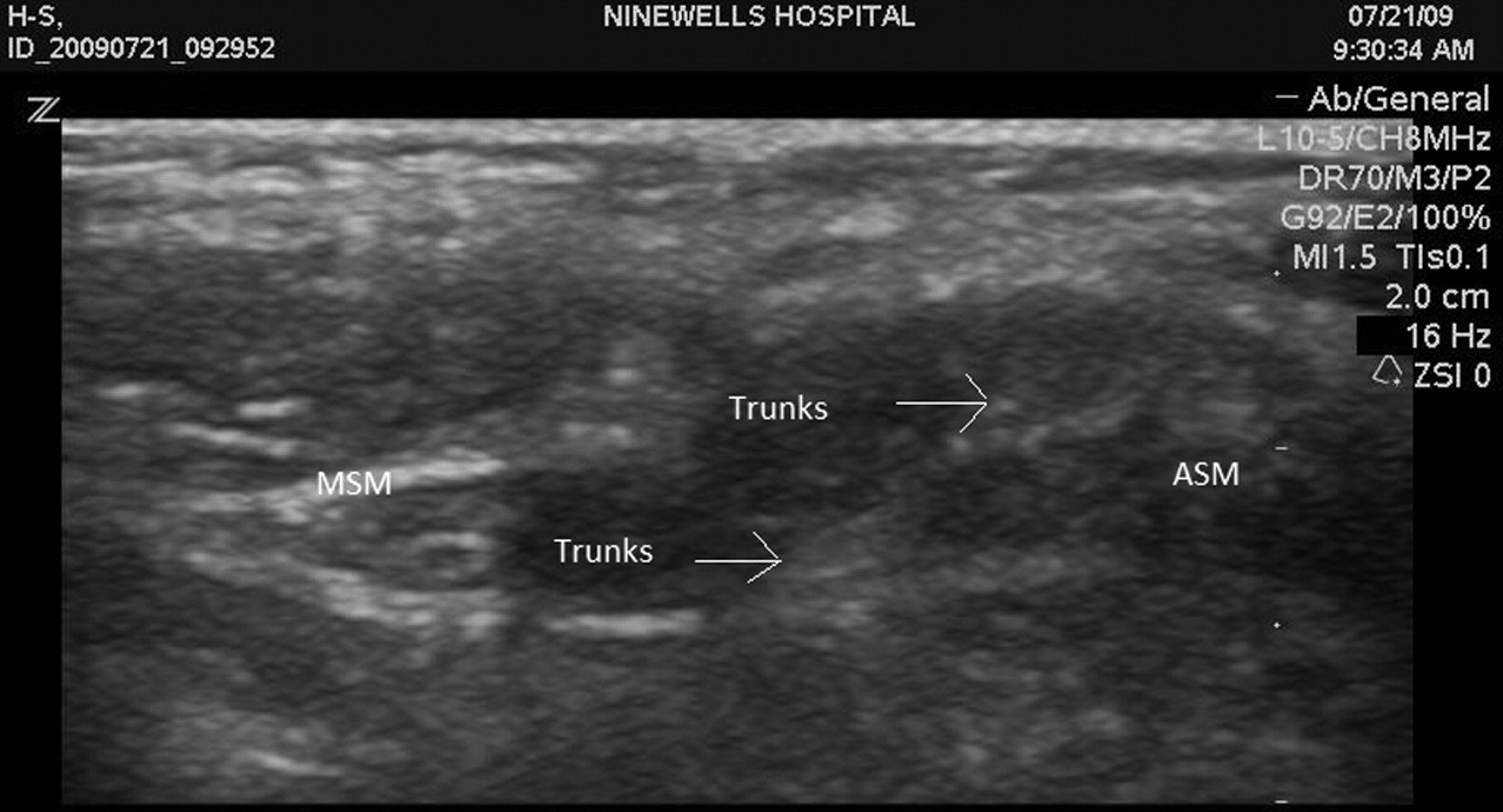
In the Thiel cadavers the anterior and median scalene muscles are difficult to see
Tracing of nerves
Previous work tracing the sciatic nerve 7 has shown that the optimum regions for sciatic block are the popliteal and mid-thigh regions: this is clearly shown in the volunteer sciatic images (Figures 6 and 7). Using the 9–3 MHz probe, tracing of nerves was straightforward in each Thiel cadaver. It was possible to follow the sciatic nerve from the popliteal fossa to the subgluteal area in the groove, which separates biceps femoris laterally and semitendinosus medially. In cadaver H (Figure 8) the sciatic nerve is split into its constituent components – tibial nerve medially and common peroneal nerve laterally – 5 cm above the popliteal fossa. In contrast, the division is not seen in the mid-thigh region (Figure 9) in cadaver F. In both images the internal structure of the nerve can be visualized easily (Vienna score 1). The popliteal artery and vein lie 1–2 cm medial and deep to the sciatic nerve and form a recognizable landmark: the artery lies medial to the vein.

Position of sciatic nerve in popliteal fossa
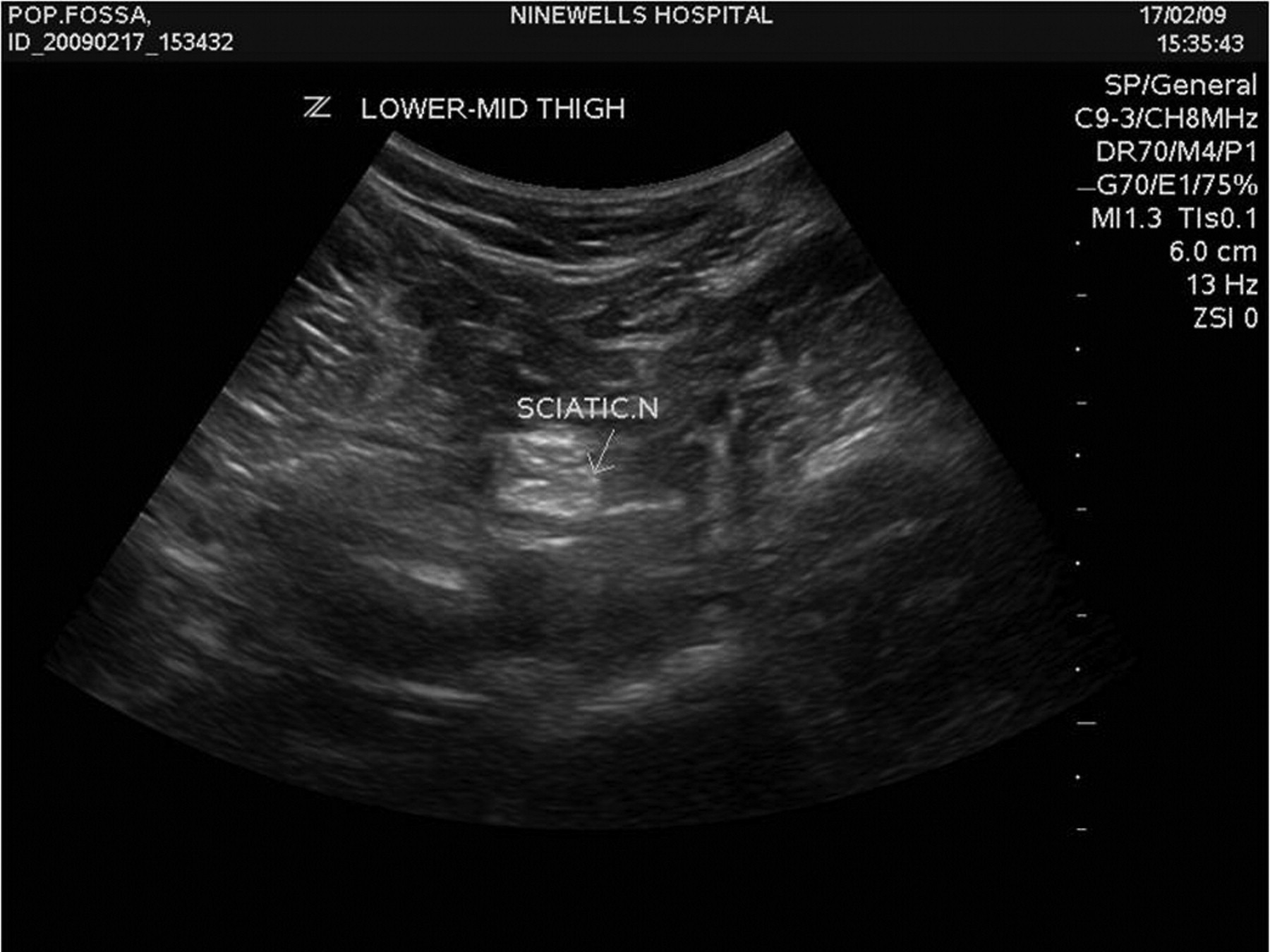
The optimum regions for sciatic block are the popliteal and mid-thigh regions
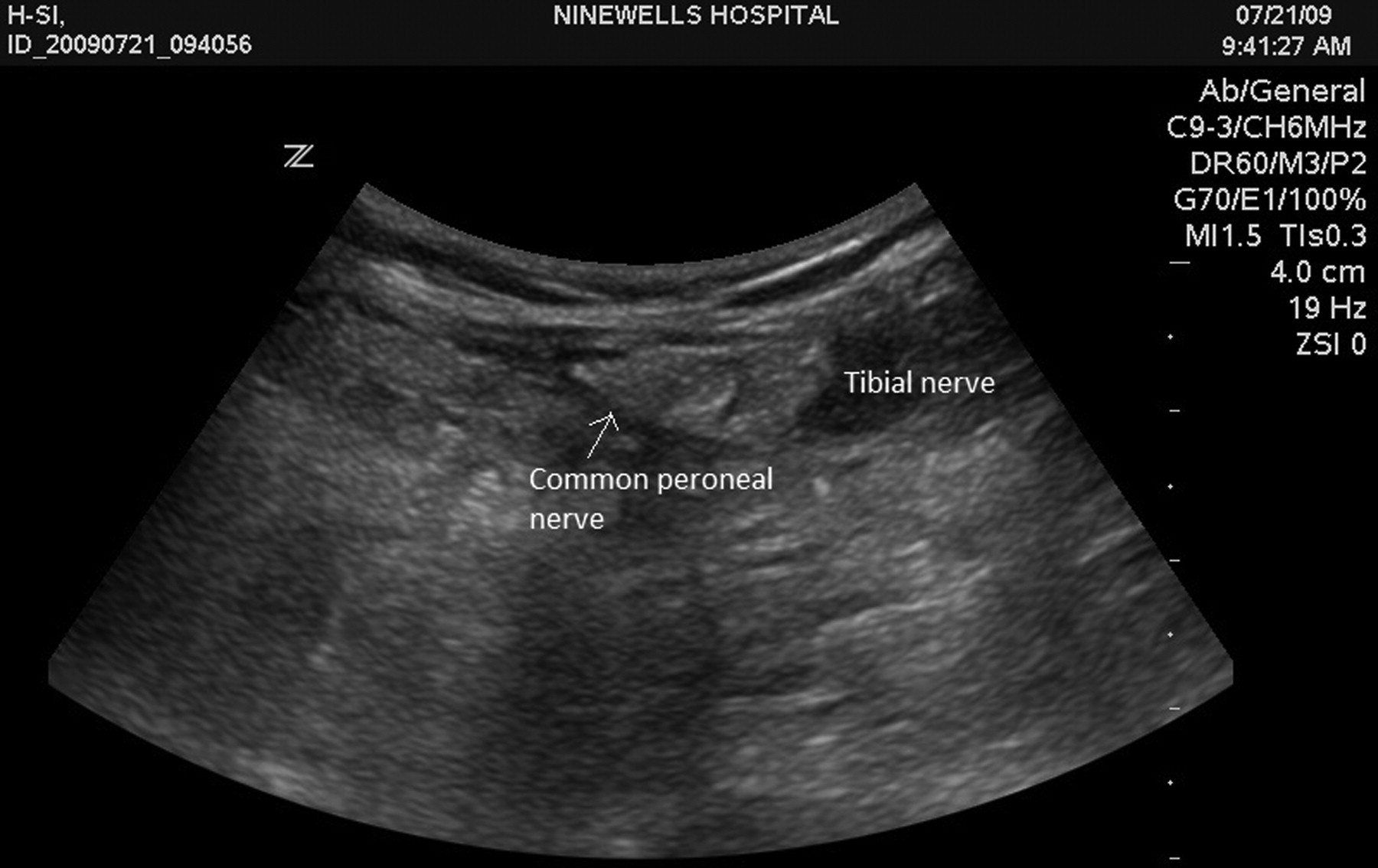
The sciatic nerve is split into its constituent components

The division is not seen in the mid-thigh region
Recognition of complications
The sciatic nerve of cadaver F was deliberately entered in order to visualize an accidental intraneural injection. The sciatic nerve in cadaver F (Figure 10) shows a needle breaching the epineurium, splitting the sciatic nerve and extruding contents after injection of 1 mL fluid.

The sciatic nerve in cadaver F shows a needle breaching the epineurium
Discussion
This pilot study has shown that the Thiel cadaver preparation should be considered for further development as a simulator for regional anaesthesia training.
The advantages noted during this study were that positioning of the upper and lower limbs was easy, tactile feedback was realistic and inadvertent intraneural injection could be readily observed.
The laxity of Thiel cadavers allows easy access to the axilla for ultrasound-guided block of the median, ulnar, radial and musculocutaneous nerves, unlike rigid formalin-embalmed cadavers. In addition, the Thiel cadaver provides an excellent model for anaesthetic simulation by replicating the sensation of fascial puncture during needle passage through subcutaneous tissues. Ultrasound of peripheral nerves is often poorer in the elderly due to poor reflection from tissues. Nevertheless, our images of peripheral nerves from the Thiel cadaver compared well with the images taken from student volunteers.
Within our practice, nerve scanning from the popliteal crease to the subgluteal region is performed before sciatic block. Tracing a nerve is a good training exercise, but also helps differentiate the sciatic nerve from tissue artefacts that may pass for nerve. Our recent work has shown that the depth to the nerve reduced in an almost linear fashion from the subgluteal to popliteal regions, but that the best images are seen in the popliteal and mid-thigh regions. Interestingly, this rather complicated relationship between depth and image quality was reproduced well in the Thiel cadaver, and augers well for training preanaesthesia scanning.
Surveys report the incidence of nerve damage secondary to regional anaesthesia to vary from 0.03% to 0.3%. 8,9 Thus the simulation of inadvertent intraneural injection is of utmost importance in order to train anaesthetists well and avoid potentially, disabling neurological damage. Injection of 1 mL increments of embalming fluid into the Thiel cadaver sciatic nerve was associated with high resistance to injection, swelling of the nerve and extrusion of contents/embalming fluid, replicating human intraneural injection.
The disadvantages of the study were that visibility of the nerve and needle were not optimal. During placement, the needle was difficult to see and only tissue distortion was detected as it passed towards its target. However, this is consistent with the poor clinical visibility of needles when passed in plane during the majority of nerve blocks. When positioned in plane the needle was clearly visible. However, our group of engineers and clinicians is investigating various applications of ultrasound technology and needle technology with the aim of improving image quality.
Broader advantages of the Thiel preparation concern safety. Traditional cadavers are preserved with formaldehyde, a known carcinogen, absorbed easily through skin and mucous membranes, and non-embalmed cadavers, such as fresh cadavers, increase the risk of exposure to infection. Thiel's embalming mixture is a water-based mixture of salts for fixation, boric acid for disinfecting, glycol, chlorocresol and ethanol, morpholine as colour preservative, and a small amount of formaldehyde. The biocidal properties and low exposure to carinogenics of this mixture have been demonstrated. 10
In conclusion, the ultrasound images from both Thiel-embalmed cadavers were good, and almost matched the quality seen in patients. Nerves could easily be identified, needles tracked, fluid visualized easily around nerves after injection and accidental intraneural injection identified. Even at this early stage of assessment, it would appear that the Thiel cadaver provides good conditions for anaesthetists to simulate regional anaesthetic block techniques using ultrasound.