
Abstract
This case began as an investigation using computed tomography of a gluteal tuberculous (TB) abscess. This revealed an incidental testicular lesion that was subsequently evaluated with ultrasound. Ultrasound showed a well-defined testicular lesion, ipsilateral epididymal calcification and a hydrocoele. The presence of tuberculosis at other extrapulmonary sites combined with a positive response of the testicular lesion to anti-TB treatment made it possible to establish a diagnosis of TB epidiymo-orchitis. A reduction in the size of the testicular lesion on ultrasound surveillance enabled conservative management avoiding the need for orchidectomy or biopsy.
Tuberculous (TB) epididymo-orchitis is a form of genitourinary tuberculosis usually developing primarily in the epididymis with extension to the testis at a later stage of the disease. 1 Unfortunately, diagnosis and treatment of extrapulmonary tuberculosis are often delayed when the symptoms are non-specific and TB infection of the scrotum can be difficult to distinguish from tumour and infarction. 2
This case describes a patient with multifocal extrapulmonary TB. It highlights the role of ultrasound in the diagnosis and follow-up of an incidental testicular lesion identified on a pelvic computed tomography (CT) scan.
Case report
A 27-year-old man, originally from the Indian subcontinent, was admitted to the orthopaedic ward complaining of increasing right hip and back pain, night sweats and weight loss.
Biochemical and haematological tests showed C-reactive protein (CRP) elevated to 219 mg/L (normal range 0–10 mg/L). Recent diagnosis of tuberculosis in the left ankle raised the clinical suspicion that TB may also be the cause of the patient's hip and back pain.
Magnetic resonance imaging of the spine and pelvis revealed a large fluid collection overlying the right greater tuberosity. Further investigation with CT showed a 5.1 × 7 × 3 cm abscess behind the right hip extending into the adductor muscles that was subsequently drained under ultrasound guidance. A sample was sent for microbiological analysis resulting in a diagnosis of acid-fast bacilli of Mycobacterium tuberculosis. The consultant radiologist reporting the CT scan also noted a 5 mm dense nodule in the left testis (Figure 1), and recommended further evaluation of this lesion with ultrasound.
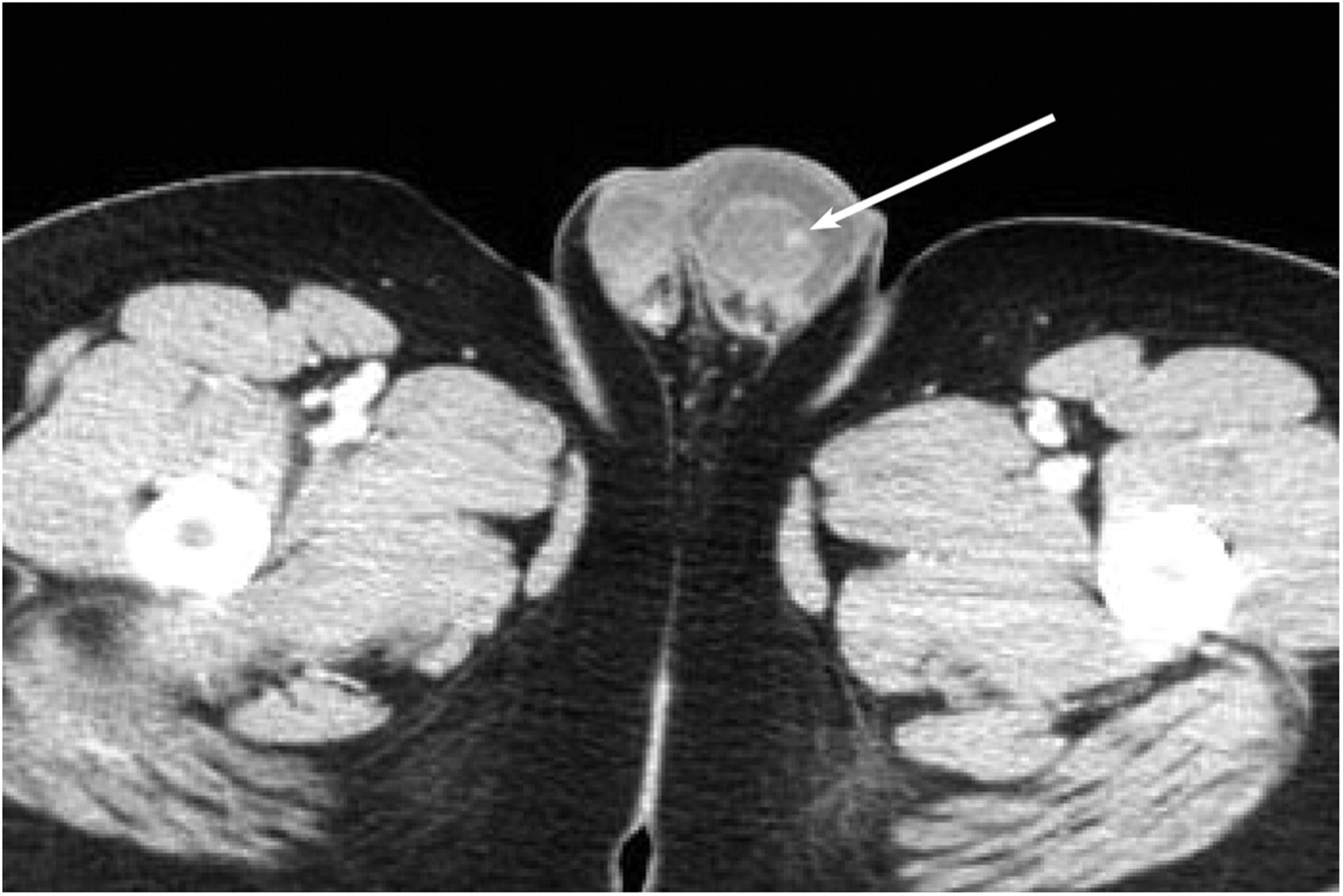
Axial computed tomography through the inguinal region and scrotal sac demonstrating a left testicular mass (arrow)
Testicular ultrasound was performed by a highly experienced sonographer seven days after the CT scan using a Philips HDI 5000 ultrasound machine (Philips Healthcare, Guildford, UK) with a 12–5 MHz linear array transducer. This showed a 6 mm echopoor lesion within the left testis (Figure 2) with peripheral vascularity (Figure 3). A large left hydrocoele and foci of benign calcification in the head of the left epididymis were also demonstrated.

Transverse section of the left testis with a 6 mm lesion and a hydrocoele
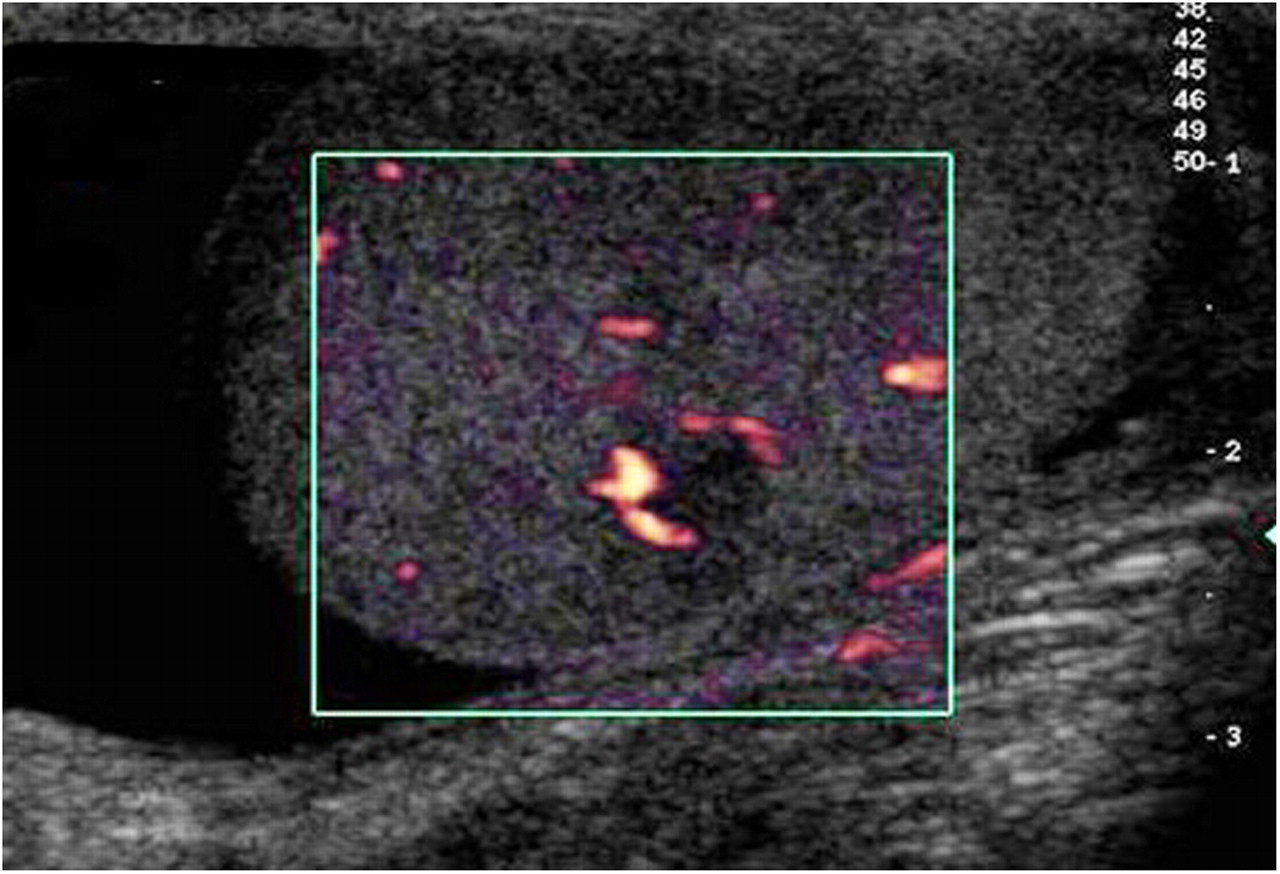
Peripheral vascularity of the left testicular lesion with power Doppler
The ultrasound report from this examination suggested that the left testicular and left epididymal appearances were most likely due to TB infection but testicular malignancy could not be excluded.
The patient was then seen by a urologist; tumour markers were requested which were normal: alpha-fetoprotein = 1 kU/L (normal values <7 kU/L), total beta-human chorionic gonadotropin = 2.0 U/L (normal values <5 U/L) and lactate-dehydrogenase = 381 IU/L (normal values 160–430 IU/L).
The patient was started on anti-TB antibiotics and follow-up ultrasound was advised by the urologist to ensure that the testicular lesion was resolving. The surveillance ultrasound examinations were performed by a consultant radiologist using an Acuson S2000 (Siemens Medical Solutions, Mountain View, CA, USA) ultrasound machine with a 14–5 MHz linear array transducer. The lesion had decreased in size to 4.7 mm after one month (Figure 4) and to 3 mm after four months.

Left testicular lesion showing a reduction in size to 4.7 mm
The patient has now completed his induction phase of anti-tuberculosis treatment and the CRP levels have returned to normal. No evidence of a pulmonary lesion was found on CT or chest radiograph and investigation for HIV was negative. Unfortunately, infertility may be a consequence of tuberculosis in this patient as he has been diagnosed with azoospermia.
Discussion
Tuberculosis is a disease caused by the bacterium M. tuberculosis. The bacillii are acquired by the inhalation of droplets from an infected person. In 80% of people the bacterium is destroyed by the immune system. Some people will become sick with the disease and in others TB can remain dormant until the immune system is compromised; this is seen in patients with AIDS and HIV infection. 3,4 According to the World Health Organization, the largest number of new cases of TB in the world in 2008 occurred in South-East Asia; the patient in this case had recently arrived in the UK from India.
TB infection can spread from the lungs via the blood or the lymphatic system to other organs in the body. Genitourinary tuberculosis is a severe form of extrapulmonary TB representing 2–4% of all cases of tuberculosis and 15% of all non-pulmonary manifestations. It is the most common form of non-pulmonary TB in the UK and can be found simultaneously with pulmonary or other forms of extrapulmonary TB; 2 in this case it was coexisting with musculoskeletal TB.
Tuberculosis infection of the scrotal contents results from retrograde extension from the prostate and seminal vesicles. Infection usually starts in the epididymal tail as it has the best blood supply and is the first part to be involved in urinary reflux. The inflammatory process may either regress and heal often with calcifications, or may spread to the rest of the epididymis and eventually to the ipsilateral testis. Epididymal calcification was evident on ultrasound in our patient. Bilateral symmetrical TB involvement of scrotal contents is described in 25% of cases. TB orchitis from haematogenous spread without epididymal involvement is rare. 5
Ultrasound is the best imaging modality for evaluation of scrotal contents and the sonographic patterns of tuberculosis in the scrotum are varied and dependent on the stage of the disease.
In the epididymis different ultrasound patterns of TB epididymitis have been described: (a) enlarged, diffusely homogeneous and hypoechoic; (b) enlarged, diffusely heterogeneous and hypoechoic; (c) nodular, enlarged heterogeneous and hypoechoic. The heterogeneity is thought to be due to caseation necrosis. Nodular lesions present at a later stage in the disease process with the formation of granuloma and fibrosis. 6
In the testis the ultrasound patterns of TB orchitis are similar to those in the epididymus and include: (a) diffusely enlarged homogeneous hypoechoic testis; (b) diffusely enlarged heterogeneous hypoechoic testis; and (c) nodular enlarged heterogeneous hypoechoic testis. The pattern of multiple nodules in the enlarged testis has been described as a miliary type and a specific feature of tuberculosis orchitis. 6
The addition of Doppler ultrasound to the examination may help differentiate TB nodules from other lesions. Focal peripheral hypervascularity of a testicular TB nodule is typical; this pattern of vascularity is demonstrated in our patient (Figure 3). Corresponding pathological findings show that the central part of the TB nodule is a granuloma with caseation necrosis, whereas the periphery of the lesion has vessels. 7
Other scrotal findings on ultrasound in TB include thickened scrotal skin, hydrocoele, intrascrotal extratesticular calcification, scrotal abscesses and scrotal sinus tract. 6,8
Clinical symptoms of TB epididymo-orchitis include enlarged painful or painless scrotum and are not specific; it is, therefore, difficult to differentiate scrotal TB infection from testicular cancer, metastases, torsion and bacterial epididymo-orchitis. 2 The ultrasound appearances may also be misleading as bacterial epididymo-orchitis, infarction and testicular cancer can have similar findings to those of TB. 8
In this case the patient had no scrotal symptoms; the testicular lesion was visualized on a CT scan of the hip. Despite normal tumour markers, the clinicians were unable to exclude testicular cancer until surveillance ultrasound scans showed a positive response to antituberculous treatment. The testicular nodule reduced in size over several months and no further intervention with orchidectomy or surgical biopsy was required.
This patient is also under investigation for infertility with diagnosed azoospermia. TB epididymo-orchitis is known to cause infertility because the production of sperm is reduced or absent due to anatomical obstruction by granulomas or fibrotic distortion of the normal anatomy of the reproductive tract. 9 This may be an unfortunate consequence of TB in this patient.
Conclusion
In this case ultrasound contributed significantly to the initial assessment and future management of the patient with follow-up scans ensuring positive response to treatment thereby avoiding surgical intervention.
Although extrapulmonary TB is still rare, it is an important consideration in the differential diagnosis especially in immunocompromised patients.
Footnotes
Acknowledgements
The authors would like to thank Dr H Bardgett, Bradford Teaching Hospitals Foundation Trust for his help in compiling this publication.