
Abstract
Persistent Müllerian duct syndrome (PMDS) is a rare anomaly characterized by the presence of a combination of Müllerian derivatives, including a uterus, fallopian tubes, cervix or vagina in otherwise normally differentiated men. The female form of PMDS is particularly uncommon, making up only 5–10% of the 150 reported cases. In this case, PMDS was not diagnosed until the patient was well into the fifth decade of life. He presented with haematuria and haematospermia and was referred for sonographic examination. During the transrectal prostate ultrasound examination the Müllerian remnants were discovered, including uterus, cervix and vagina. In this report we describe the sonographic and magnetic resonance appearances of PMDS and discuss management via laproscopic hysterectomy and bilateral ovotestectomy.
Case report
A 56-year-old man was referred for sonographic examination of the prostate gland because of haematuria and haematospermia. His past medical history included bilateral cryptorchidism and a unilateral inguinal hernia. The plan at the time of his birth was to repair the hernia at age 3 or 4 years. Unfortunately, the hernia repair was not done nor was there recognition of the bilateral cryptorchidism until he was much older. At the age of 22 years, he was diagnosed with bilateral inguinal hernias and underwent bilateral hernia repair surgery at which time the cryptorchidism was recognized. Surgical exploration for the undescended testes was unsuccessful. When he was 30, the patient noticed a change in his chest hair distribution; specifically, it was thinning. When blood tests showed his testosterone level was negligible, he was prescribed testosterone. The patient was inconsistent in his use of the testosterone. At age 43 he developed gynaecomastia for which he underwent bilateral gynaemastectomy. Despite the evidence of gonadal dysfunction, imaging was not performed.
On physical examination, this man showed normal development of secondary sexual characteristics, with a normal phallus and scrotum; however, there were no palpable testes. He had a normal XY karyotype. He had been taking testosterone sporadically for 26 years; however for the six-month period prior to imaging, he began to take it regularly. This led to a series of episodes of haematuria and haematospermia.
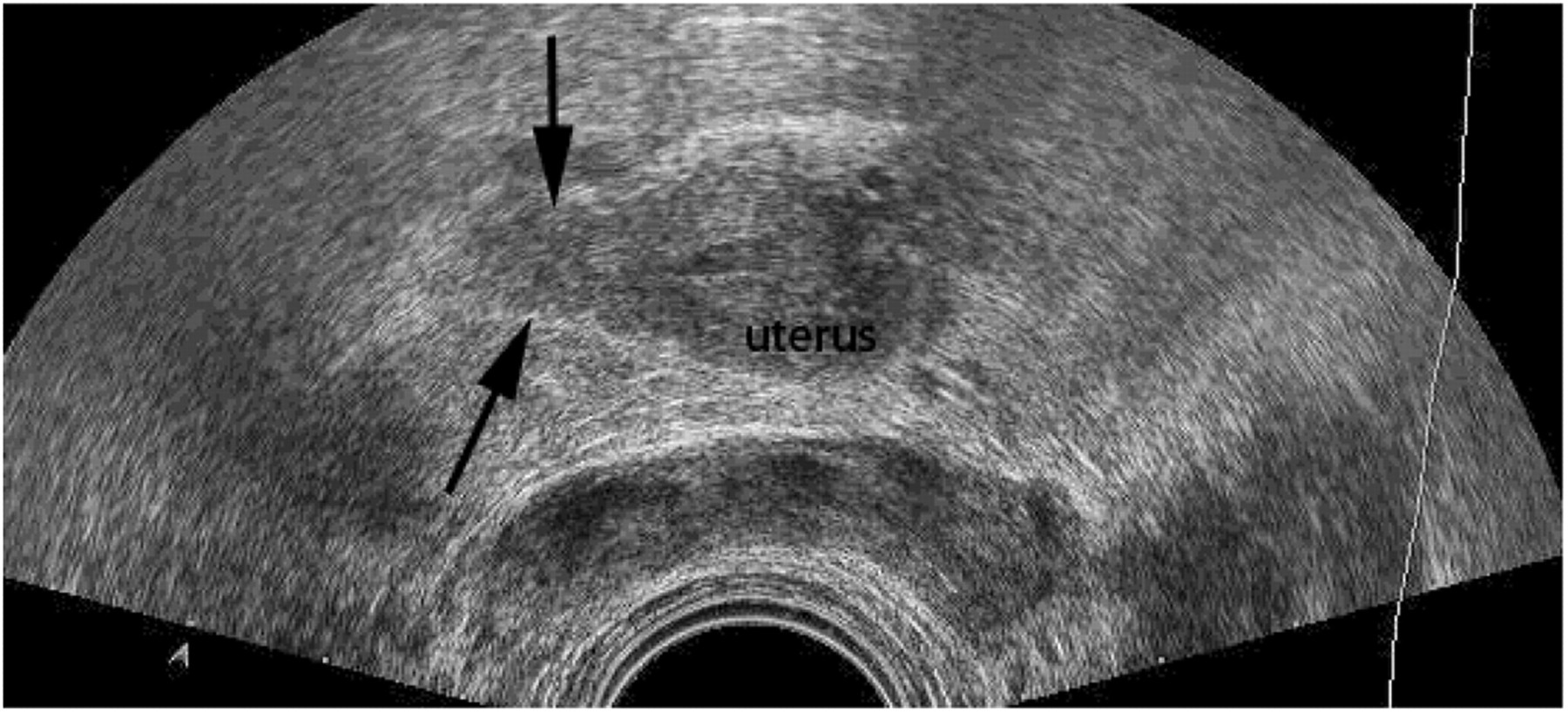
A transrectal and transvesical sonographic examination of the prostate was performed. The prostate was unremarkable. However, superior to the prostate, between the seminal vesicles was a solid, tubular structure measuring 6 cm in length, 2.7 cm in anteroposterior dimension and 2.5 cm in transverse diameter (Figure 1). The structure was hypoechoic to the surrounding bowel, and had a central tubular portion bordered by a hyperechoic rim and which appeared to be fluid-filled. It was adjacent to the bladder and appeared continuous with the superior end of the prostate. The inferior end of the structure demonstrated a beak-like narrowing and it was suspected to be continuous with the prostate (Figure 2). This had the appearance of a uterus and cervix filled with blood. A solid oval structure was seen in transverse plane during transrectal sonogram, which was thought to represent an ovotestis (Figure 3).

Transrectal sonogram of the prostate gland demonstrates a structure that is uterine in appearance, with an internal architecture that was suspected to be an endometrium (e). There is haematometra as well as blood seen in the endocervical canal and vaginal remnant

Transrectal sonogram demonstrates haematocolpos, and the communication between the vaginal remnant and the prostatic portion of the urethra
Endorectal sonogram of uterus in transverse axis. Arrows point to an oval shaped solid mass, which may represent an ovotestis
Transabdominal songraphy revealed normal kidneys and bladder; however, in the pelvis, a uterus and cervix posterior to the bladder and superior to the prostate were identified (Figure 4). A search for the undescended testes was unsuccessful by sonography.

Transabdominal sonogram demonstrating the uterine tissue posterior to the urinary bladder
Magnetic resonance (MR) imaging was performed with a 1.5 T magnet and confirmed the findings (Figures 5 and 6).

Sagittal T2-weighted HASTE MR image of the pelvis demonstrates the uterus (arrow) and cervix (curved arrow) posterior to the bladder, leading towards the prostate. Both structures are distended with high-signal fluid, representing the haematometra. HASTE MR, half Fourier acquisition single shot turbo spin echo magnetic resonance

Sequential transverse T2-weighted HASTE MR images of the pelvis show the adnexal location of bilateral testicles (arrows). Note the central uterus (curved arrow)
At surgery a rudimentary bicornuate uterus, bilateral fallopian tubes, two ovotestes, a cervix and vagina were found (Figure 7). The cervix and vagina were connected to the superior portion of the prostate tubercle, as was suspected on ultrasound and MR. When the cervix was excised, a mucous plug with bloody content drained quickly and was presumably under some pressure (Figure 8). A complete hysterectomy and bilateral salpingo-oophorectomy was performed laparoscopically. The patient recovered well, and the symptoms of haematospermia and haematuria resolved. A transrectal ultrasound-guided biopsy was not considered necessary. The patient's PSA remained normal.

Laparoscopic image of the pelvic area. Arrows indicate the rudimentary bicornuate uterus. An ovotestis was found in each adnexum
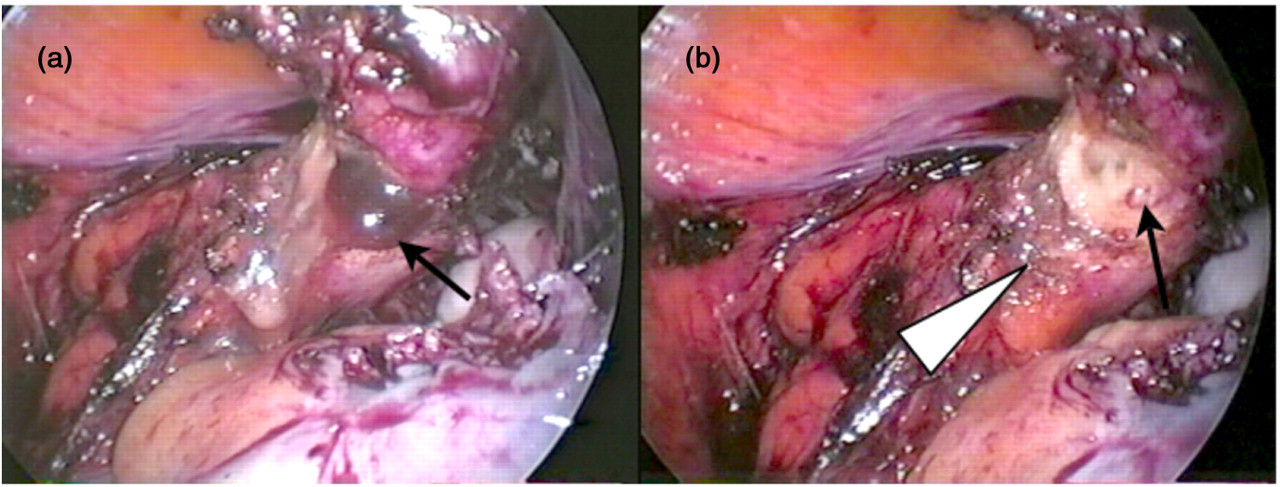
Laparoscopic image of the persistent Müllerian structures. (a) cervix (arrow) with the bloody mucous plug. (b) Arrow points to the endocervical canal visible once the mucous plug was suctioned. Arrowhead indicates the vagina
Discussion
Persistent Müllerian duct syndrome (PMDS) is a rare disease that is often missed at birth. There are two anatomic variants of PMDS, the male and the female type. The most common is the male type, seen in approximately 80–90% of cases, and characterized by unilateral cryptorchidism with a contralateral inguinal hernia. The male type has two subtypes, the first being hernia uteri inguinalis, characterized by a descended testis, with herniation of the ipsilateral uterus and fallopian tube into the inguinal canal. In the second type, there is crossed testicular ectopia, where herniation of both testes and the uterus and both fallopian tubes herniate into the inguinal canal.
The female variant of PMDS is characterized by bilateral 1 cryptorchidism with the remnants of the Müllerian duct, uterus, fallopian tubes and ovaries, or in some cases ovotestes are embedded in the round ligament. 2 In both variants, the normal masculine external genitalia are present, making this a difficult diagnosis.
Patients with PMDS have a normal male phenotype and are assigned to the male sex at birth without hesitation. However, thorough examination of the newborn may reveal genital abnormalities. One or both testes may not be palpable in the scrotum and in the case of unilateral cryptorchidism, the contralateral scrotal sac may contain a hernia, in addition to the testis. Diagnosis of PMDS is difficult, and unless an elder brother has been diagnosed with the condition, the persistence of Müllerian derivatives, uterus and fallopian tubes is typically only discovered at surgery to correct cryptorchidism. PMDS is a form of male pseudohermaphroditism in which the Müllerian ducts fail to regress during fetal development. This can be caused by insufficient Müllerian inhibiting factor (MIF) being released by the fetal testes by the eighth week of gestation, or by an end-organ resistance to MIF. 3 Approximately 45% of PMDS patients possess a mutation of the MIS gene while 39% possess a mutation in the MIF receptor. In 16% no mutation for either the MIF gene or receptor can be found. 4 These findings can be seen sonographically or by MR imaging.
Spermatogenesis is impaired in these patients, even in the normally descended testicle. 5 Treatment of PMDS is exclusively surgical and aims to correct cryptorchidism. The blood supply of the vas deferens and Müllerian structures is embryologically common and, therefore, surgical manipulation could lead to devascularization of the vas deferens on one or both sides. Careful dissection is required to avoid harming the excretory ducts. Fertility is rare in PMDS patients and is reported to be approximately 11%. 6 This is most likely explained by a lack of proper communication between the testes and excretory ducts and lesions at orchidopexy.
A variety of germ cell tumours have been associated with PMDS with an incidence as high as 10%. 7,8 Bilateral intraabdominal cryptorchidism occurs in only 10% of cases with PMDS and it presents a dilemma; there is some controversy over whether surgical treatment should be carried out. The persistent Müllerian structures are often tethered, limiting mobilization of the testicles without removing the uterus. While some have recommended removal of the remnants of Müllerian structures at the time of orchiopexy, 5,9 others advocate leaving these organs in place. 10 Malignant degeneration of Müllerian structures has been reported just once as a clear cell adenocarcinoma of the Müllerian duct in PMDS in a 67-year-old man. 11
In our patient, we suspect that some of the prescribed testosterone was converted to estrogen and, therefore, was responsible for the sloughing of the endometrial cavity, presenting as haematuria and haematospermia. In essence, the hormonal therapy had induced menstruation in the rudimentary uterus which was communicating with the prostate and prostatic urethra.
To conclude, sonographic examination of the male pelvis in cryptorchidism may reveal rather unexpected structures. PMDS involves complex anatomy, which can be easily seen by ultrasound or MR.
DECLARATIONS
The authors have no conflicts of interest to declare.