
Abstract
The management options for ganglion cysts include: observation, aspiration ± injection with steroid and surgical excision. One of the problems encountered during fine needle aspiration is the highly viscous cyst fluid being difficult to withdraw. We propose a modified technique, which improves the ease and speed of achieving complete aspiration of ganglion cysts by using local anaesthetic. Twenty-five patients who were referred from primary care and orthopaedic outpatients were diagnosed with ganglion cysts on ultrasound. The modified aspiration technique involves injecting a small volume of local anaesthetic into the cyst fluid prior to aspiration and was performed on all patients. All cysts were completely drained using this modified technique with no immediate complications and with minimal discomfort to the patient. Our adaptation to the technique of simple aspiration provides a method of achieving complete ganglion resolution with ease and in a time frame appropriate for a standard outpatient appointment. Low immediate complication rates are seen due to the adjunct of ultrasound and the local anaesthetic reduces patient discomfort during the procedure. This method has been particularly effective for large ganglions but can be equally effective for treating smaller lesions.
Ganglion cysts are benign, fibrous soft tissue swellings that can arise in the proximity of several joints or tendon sheaths throughout the musculoskeletal system. The majority (60–70%) of ganglions found in adults are seen in the wrist but they are also frequently found elsewhere. 1 The management options for ganglions include observation, as up to 50% may spontaneously resolve, 2 aspiration ± injection with steroid and surgical excision. We propose a modified technique, which improves the ease and speed of achieving complete aspiration of ganglion cysts by using local anaesthetic.
Background
Ganglions can be diagnosed clinically by their features and location, or by using imaging techniques including ultrasound and magnetic resonance due to their characteristic fluid content. They are usually noticed due to a swelling but can also cause pain or weakness due to pressure effects on local nerves. 1
The fluid found within ganglions is particularly viscous and several hypotheses have been put forward for the source of this fluid. Although ganglions have been found to be in connection with local joints in some cases, it is not believed that the fluid within them is synovial. It has been suggested that the fluid arises from myxoid degeneration 1 or from the cells found within the cyst wall. One of the reasons that ganglion fluid is so viscous is due to its high hyaluronic acid content, 3 which gives it a jelly-like consistency.
Despite some high recurrence rates seen with aspiration, 4 it provides instant relief from pressure symptoms and pain by reducing the swelling. It is, therefore, a good method with which to manage a ganglion that has not resolved spontaneously, prior to electing for surgical excision. Aspiration has a lower incidence of collateral nerve or vessel injury compared with surgery, 5 particularly when used in conjunction with ultrasound and can be performed easily in a clinic setting.
One of the problems encountered during fine needle aspiration is the highly viscous fluid being difficult to withdraw. Techniques such as injecting hyaluronidase into the cyst to depolymerize the hyaluronic acid was first described by Otu in 1992 with very low recurrence rates. 6 Further studies since then, which have compared aspiration alone with the use of hyaluronidase and with surgery, have also shown lower recurrence rates when using hyaluronidase; however, these have not been as low as initially seen by Otu or as those seen postoperatively. 3,7–9 Additionally, an equilibration period of up to 20 minutes is needed to allow the hyaluronidase to work. 9
Methods
Twenty-five patients who were referred from primary care and orthopaedic outpatients were diagnosed with ganglion cysts on ultrasound around the wrist, elbow, hand, shoulder, knee, ankle and foot. The maximum cyst diameter ranged from 1.8 to 7.2 cm (Table 1). The patient ages ranged from 21–59 years. Informed consent was obtained regarding the risk of neurovascular injury, infection and recurrence. The modified aspiration technique was performed on all.
Aspiration technique
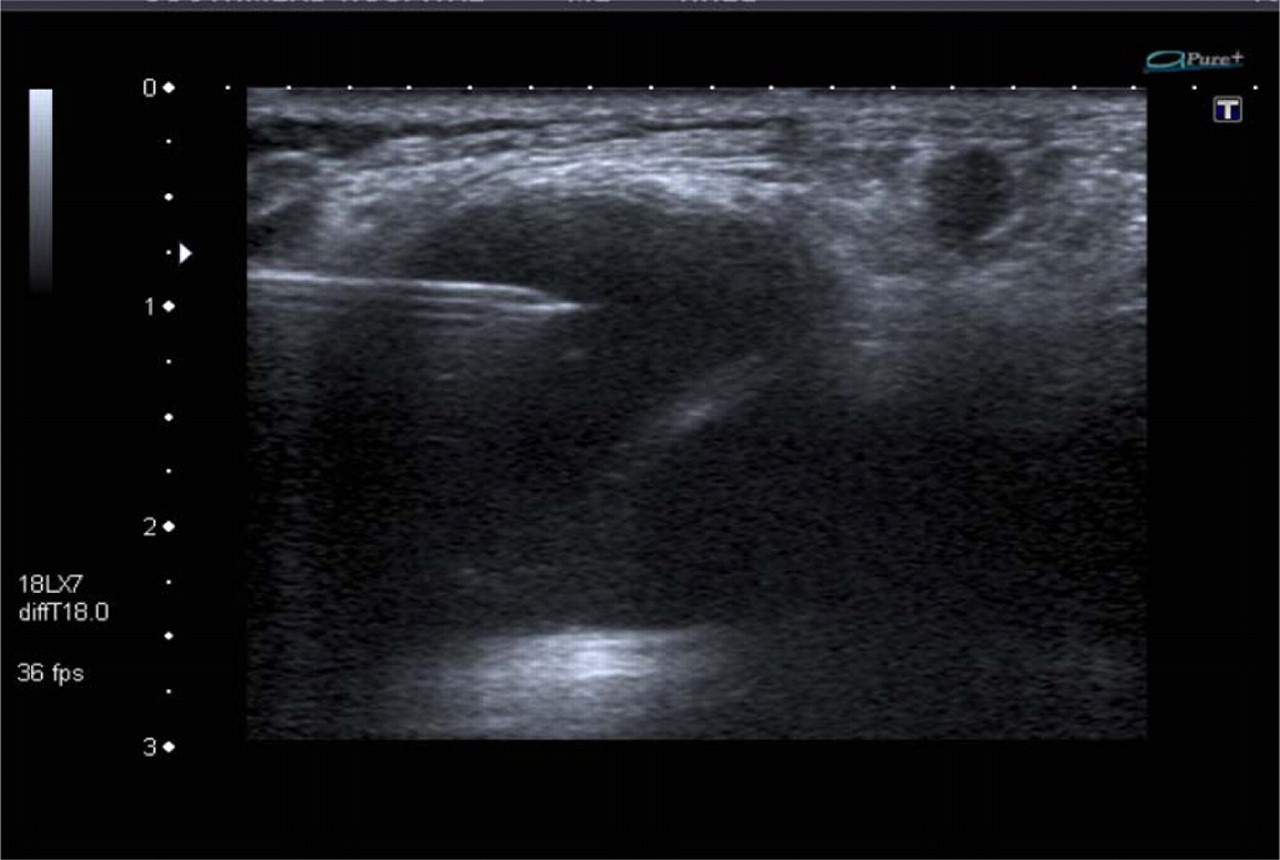
Below is a description of the technique that we used during outpatient ultrasound clinics. The images demonstrate the procedure being performed on a 18 × 15 × 25 mm cyst situated on the dorsum of a male patient's wrist:
The ganglion is located using a high-frequency linear ultrasound transducer, enabling a clear path for the needle to be defined, avoiding local neurovascular structures;
10
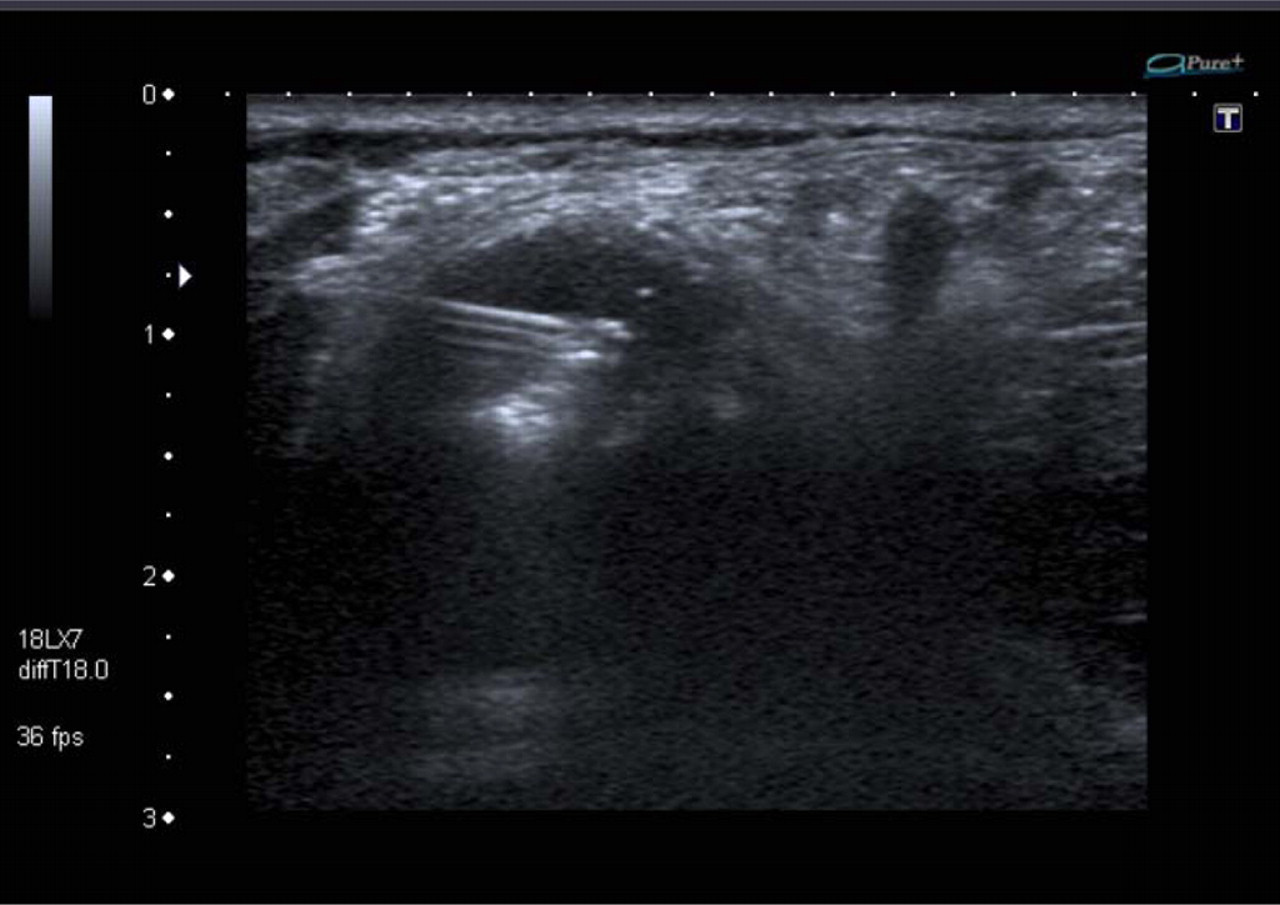
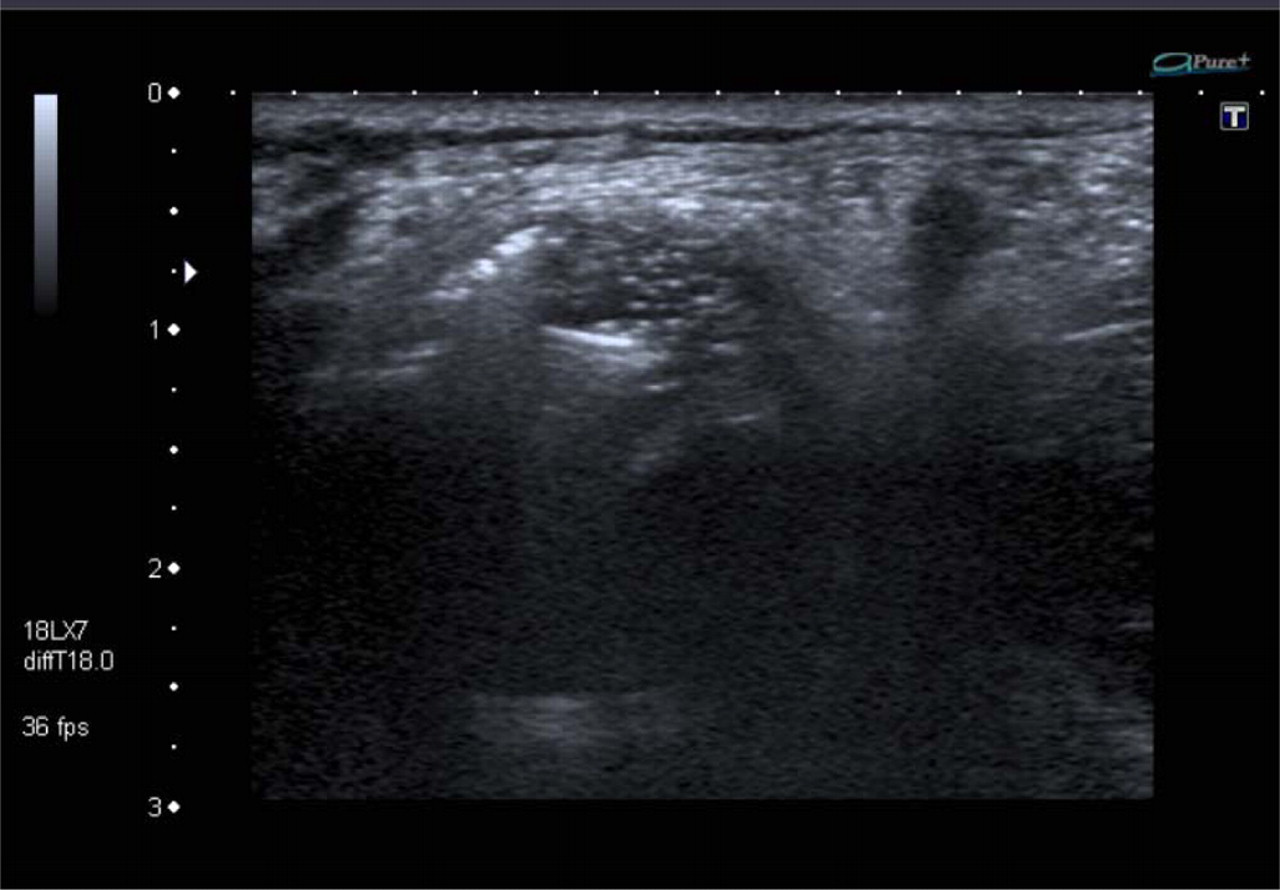
The patient's skin is then cleaned with antiseptic cleaning agent and a sterile cover is applied to the transducer. Sterile ultrasound gel is placed on the skin and using this aseptic technique, 1% lignocaine is infiltrated to the skin and subcutaneous tissues at the point chosen for aspiration; A new 19-gauge needle is passed into the cyst cavity (Figure 1), approximately 10–30% of the fluid is aspirated using a 20 cc syringe and discarded, leaving this needle in situ; The amount of fluid aspirated initially is then replaced by lignocaine from the syringe used to infiltrate the skin in step 2, via the 19-gauge needle in situ. When using ultrasound guidance, a swirling effect can be seen within the cyst cavity, which denotes mixing of the two fluids and, therefore, a decrease of the cyst fluid viscosity (Figure 2); The remaining ganglion contents are then aspirated. This process of lignocaine injection and aspiration can be repeated until complete aspiration is achieved and manipulation of the needle is particularly useful for mobilization of dependent cyst fluid (Figure 3) or that seen within loculations. We advocate using the needle bevel to puncture and score the inner cyst wall to encourage scarring (Figure 4) as described by Gude and Morelli.
2
After aspiration, corticosteroid may be injected as preferred;
3
the author uses up to 40 mg of non-diluted preparation of Triamcinolone (Kenalog). Ultrasound-guided puncture of a ganglion cyst on the wrist of a male patient Infiltration of local anaesthetic into the cyst fluid Mixing of local anaesthetic with dependent cyst fluid after the first aspiration Abrasion of the cyst wall with needle bevel and introduction of corticosteroid after complete aspiration

Results
In 23 of the cysts treated, the fluid was drained until no more could be detected. Multilocular cysts proved more difficult to drain completely and a small amount of residual fluid was seen in two of these. All lesions were treated with aspiration and cyst wall scoring followed by steroid injection.
Distribution and characteristics of ganglion cysts treated
No significant pain or discomfort was experienced by the patients during the procedure and no immediate complications were observed.
Discussion
Ultrasound-guided aspiration of ganglion cysts can achieve immediate and in some cases lasting resolution of symptoms with little risk of complication. This is a commonly used technique in the management of ganglions and avoids the potential risks of surgery that include infection, scarring, stiffness and neuroma. 2 In addition, patient satisfaction is often increased when this technique is employed. 11 Although recurrence rates are variable, complete aspiration of the cyst contents is more likely to be achieved if the cyst fluid's viscosity is reduced.
One percent of lignocaine was chosen for the technique described due to its physical, but also its anaesthetic properties, which are particularly beneficial during cyst wall abrasion. However, we have found that during the treatment of very large cysts, sterile water or saline with similar viscosity to local anaesthetic can be added for extra volume with good effect and reduced costs. The use of hyaluronidase has been shown to be effective in decreasing the viscosity of ganglion fluid but the equilibration period required to achieve this prolongs the consultation time. Other adaptations of the aspiration technique have included injecting sclerosant or passing a silk suture through the cyst to allow drainage of re-accumulated fluid and promote scarring. However, these methods were abandoned due to the possible passage of sclerosant into the joint and infection, respectively. 2 Our adaptation to the technique of simple aspiration, by injecting local anaesthetic prior to withdrawing the majority of the cyst fluid, provides a method of achieving complete ganglion resolution within a time frame appropriate for a standard outpatient appointment. Low complication rates are seen due to the adjunct of ultrasound and the local anaesthetic reduces patient discomfort during the procedure. This method is particularly effective for large ganglions such as those adjacent to the knee, one of which in our cohort required up to four cycles of aspiration and contained over 25 mL of fluid. We also found this technique equally effective for treating smaller lesions that are much more common, such as those seen around the wrist. However, we observed that the modified aspiration technique may not be beneficial in the treatment of cysts measuring less than 20 mm in maximum diameter as they are usually satisfactorily treated by one aspiration unless the fluid is particularly viscous. The operator should tailor this technique as necessary; if the fluid is of low viscosity and can be withdrawn easily, they may decide to aspirate as much as is feasible with the first cyst puncture, only using the local anaesthetic at the end of the procedure to mobilize residual-dependent fluid and complete the drainage.
Long-term recurrence rates of ganglions managed non-surgically are varied and though up to 50% resolve spontaneously 2 this can take several years. We acknowledge that we have no data regarding recurrence or non-immediate complication rates for our patient cohort and that these could strengthen our study significantly. Future evaluation of this technique with follow-up data would be appropriate.
Despite the condition being benign, patients often seek treatment due to cosmesis or secondary pressure symptoms, for which aspiration can achieve excellent results and is, therefore, used commonly in preference to surgery. Our method provides a quick and effective way of performing this with minimal patient discomfort.