
Abstract
We are at risk of teaching our trainees to be ‘image-seekers’. Sonoanatomy is easily demonstrated but teaching the practical skills of ultrasound-guided nerve block constitutes a greater challenge. Participants may return to their institutions after attending educational courses as proficient ‘image-seekers’, yet still unsure about performing nerve blocks. Safe ultrasound-guided regional anaesthesia (USGRA) requires integration of several skills. These are correct image acquisition, accurate needle guidance and appropriate spread of local anaesthesia. Most educational courses cannot combine all these skills. We describe realtime nerve blocks on cadavers to teach USGRA. Unembalmed cadavers offer more realistic imaging and tactile needle feedback than other models. We evaluated participants' perceptions of cadavers for training, their impact on confidence and whether subsequent change in practice occurred. Fifty participants completed pre- and post-training questionnaires and were followed up at three months. Confidence was scored on a five-point scale. Complete data-sets were received from 42 participants (84%). Most (98%) found the cadavers to be of educational benefit and 86% found the imaging and tissue properties comparable to clinical practice. Mean (±SD) confidence score increased from 1.7 (±0.92) precourse to 4.3 (±0.65) postcourse (P < 0.0001). At three-month follow-up, 84% considered they had received sufficient training to introduce ultrasound into their clinical practice and 87% (27% precourse) now used ultrasound routinely. Only four participants had not made a change to their practice.
We are at risk of teaching our trainees to be ‘image-seekers’. Sonoanatomy is easily demonstrated but teaching the practical skills of ultrasound-guided nerve block constitutes a greater challenge. Participants regularly return to their institutions after attending educational courses as proficient ‘image seekers’, yet still feel untrained and unsure about performing nerve blocks. They are able to find and demonstrate the nerves, but struggle to translate this theory into actual nerve blocks on patients. Practice on phantoms can improve hand–eye coordination skills, but this is still often insufficient to encourage the wary novice to perform their first few nerve blocks. Newer echogenic needles can improve confidence in visualization, 1 but safe and successful invasive procedures require the integration of both the newly acquired theory and the practical skills to achieve it. Most training courses cannot combine all these skills meaning patients have been the ‘training ground’ for development and refinement of techniques. Given the ethical implications associated with this we need to look at other ways with which we can improve our techniques in a realistic environment before involving patients. 2 Unfortunately, there are few realistic simulators that assist novices to gain realtime experience of ultrasound-guided regional anaesthesia (USGRA). An assessment of the ability to use Thiel-embalmed cadavers for teaching USGRA has recently been published. 3 We hypothesized using fresh cadavers would improve confidence in performance of USGRA and lead to a sustained change in clinical practice at three-month follow-up.
Method
The use of cadavers to teach USGRA was conducted following ethical approval from the Fresh Frozen Cadaver Committee of The University of Western Australia. A two-day course was designed and conducted at the Clinical Training and Evaluation Centre (CTEC) of the Faculty of Medicine, Dentistry and Heath Sciences of The University of Western Australia. This is a purpose-built facility with a high-fidelity simulation suite and a cadaver-based surgical workshop with 10 fully equipped operating tables.
Cadaver preparation
Cadavers are assessed on presentation for their suitability to be fresh frozen. Surgical scars are identified and appropriate imaging for joint prostheses and pelvic viscera performed. The cadaver is washed with dilute chlorhexidine solution and the head shaved. The cadaver is frozen in a body bag at –20°C over approximately 3–4 days, and then stored until needed. During the thawing process (4–5 days), the cadaver is left in a normal temperature room (18–20°C) by day and then placed in a refrigeration room overnight (5°C). This staged approach to thawing has been empirically developed over an 18-month period. We believe that the smoother gradient of temperature gain contributes to reduced rigidity and near-live properties in our cadavers.
In an effort to overcome the problems associated with lack of vascular anatomy, we have trialed perfusing the vascular system with a dyed gelatin suspension via both superficial femoral arteries. The gelatin concentration was such that 238 g of gelatin were added to 3 L of saline and dissolved by stirring at 70°C for 30 minutes. Alizarin red dye was added (5 mL/L) to colour the solution red for the benefit of vascular surgeons using the cadaver subsequently. The gelatin solution was infused via gravity feed from a height of 1 m and required 2.75 L. The cadaver was then frozen as previously described. This technique has restored the appearance of vascular anatomy and allows realistic imaging especially in areas such as the brachial plexus (Figure 1). Participants have rated this perfused cadaver very highly and all future cadavers we use will be preprepared in this manner. A second cadaver perfused after initial thawing proved not to be as good, presumably because the vessels had collapsed completely and did not allow perfusion to occur to the same degree. Others have restored pulses using a pneumatic device. 4
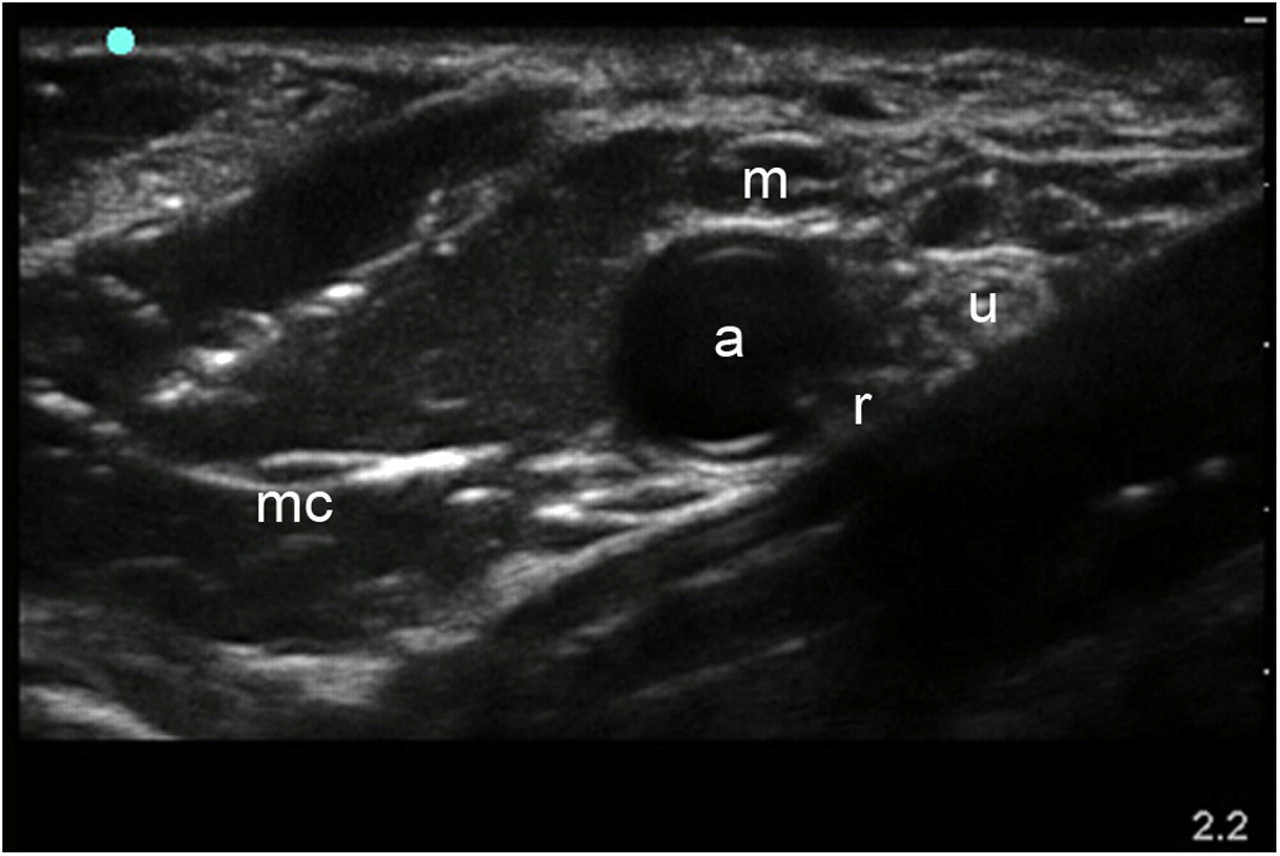
Ultrasound image of the axillary brachial plexus in a fresh cadaver demonstrating restoration of normal vascular anatomy following gelatin perfusion. Labelled structures are median nerve (m), ulnar nerve (u), radial nerve (r), musculocutaneous nerve (mc) and axillary artery (a)
Cadavers are eviscerated after the first thaw, creating a significant air interface at the peritoneum. This affects the sonographic image for transversus abdominus plane blocks with the transducer positioned anteriorly. However, good images can still be obtained if the transducer is moved posteriorly towards the location of the transversalis plane block as more recently described. 5 Even with this limitation, the tissue planes can be identified sufficiently well to allow practice needle and local anaesthetic placement between the internal oblique and transversus abdominus muscles that is required to achieve analgesia in patients (Figure 2).

Ultrasound image showing the abdominal wall tissue planes in a fresh cadaver following evisceration. Labelled structures are external oblique muscle (e), internal oblique muscle (i), transversus abdominus muscle (t) and the air artefact (a) that alters the appearance of the lower right half of the image
Course design
Our training consisted of small group hands on workshops, lectures and debate sessions. It was open for anyone to register. We trained 50 specialist anaesthetists at a time, due to size constraints in the anatomical workshop. Ten general practitioner anaesthetists also attended the course but owing to differing professional development requirements from the Royal Australian College of General Practitioners, they were evaluated in a different way from the remainder of the group. Individual nerve blocks were taught using multiple modalities by 12 anaesthetists experienced in USGRA.
A sound knowledge of anatomy is crucial to safe regional anaesthesia. Dissected anatomical prosections were, therefore, examined to revise the important relationships relevant to nerve blocks. Realtime hands on scanning of live models provided experience at locating the anatomical structures. The ergonomics required for safe and effective block performance were emphasized. Participants then had an opportunity to practise the newly acquired skills on realistic human tissue. Saline was injected during some cadaveric practice blocks to simulate the desired spread of local anaesthesia. Where the use of cadavers was not possible, open pig thoraces were used to practise intercostal and paravertebral blocks. Dye was injected to visually track the spread of the injections into porcine tissue. Safe needle practice was emphasized and universal precautions were observed throughout the course. Photography was prohibited and appropriate consideration given to the human donors.
Course evaluation allows the determination that an educational event is meeting the needs of its participants. As part of our standard evaluation, participants completed pre- and post-training questionnaires to assess prior experience and confidence. Due to voluntary registration for this education, consent to participate was implied. A five-point Likert scale was used with one indicating the lowest score and five indicating the highest. All participants were followed up at three months using a web-based survey to determine whether changes in practice had occurred following the course (
Results
Interest greatly exceeded the capacity showing a demand for this type of teaching. The course filled rapidly and is now a regular event on the CTEC calendar. Complete data-sets were received from 42 anaesthetists (84% response). Most (90%) were practising in teaching hospitals and 80% were specialist anaesthetists. Many were experienced anaesthetists (mean 10.5 years, range 4–25 years); however, 70% described themselves either as beginners or had no previous experience with USGRA. Fifty-eight per cent of participants had attended other regional anaesthesia courses. Eight (19%) had previously used cadavers for training for other procedural skills. Most (98%) agreed that the inclusion of cadaveric block practice was beneficial to the educational experience and 86% found the cadaveric imaging and tactile needle feedback comparable to clinical practice.
Participants almost unanimously found the anatomical prosections (95%), live model ultrasound scanning (98%) and cadaveric block practice (98%) to be of educational benefit. Only 51% felt that expert debate sessions had been beneficial and this has been removed from subsequent courses.
Mean (±SD) confidence score increased from 1.7 (±0.92) precourse to 4.3 (±0.65) postcourse (P < 0.0001) for all nerve blocks combined. Data for individual nerve blocks are shown in Table 1. Precourse confidence at performing femoral nerve blocks was already high. This may reflect the fact that this is a commonly performed nerve block in our region. Postcourse confidence was lowest for infraclavicular block possibly reflecting the relative difficulty of this approach to the brachial plexus compared with others demonstrated.
Confidence scores for individual nerve blocks
Only nerve blocks taught on the course are listed. Results expressed as median (95% confidence intervals)
We received 31 replies to the Internet-based survey at three-month follow-up (62% response rate). This was less than hoped but is in keeping with most survey-based research. Most (84%) felt the course had provided sufficient training to start using USGRA in clinical practice and 87% now used USGRA as their technique of choice compared with 27% precourse. Four participants had not made a sustained change to their practice. The most common reason was a lack of clinical opportunity or inadequate equipment.
Discussion
Ultrasound-guided techniques have been described for the majority of nerve blocks. Increasing availability of portable ultrasound machines, providing high-quality imaging, is fast making it the technique of choice. It has already been labelled the gold standard, 6 although this may be debated by some. Despite early evidence of improved outcome using ultrasound, 7–13 we are all still on the learning curve, albeit rapid. 14 Multiple training courses are available but these may not cover the practical issues of performing nerve blocks once participants return to their own institutions. Without the support of a colleague experienced in the techniques, clinicians may be reluctant to start using their newly acquired knowledge and these skills may rapidly fade. We devised, implemented and evaluated a multimodal regional anaesthesia course in an effort to bridge this gap in education. We did not objectively score competence during the course as there remains no reliable and valid assessment tool. 15 Competence cannot be assessed on a single observation during a training workshop. Neither were we able to determine whether the cadaveric practice blocks would have been successful, other than by observing spread of injectate in the cadaver. Rather the workshop was designed to increase confidence and technical skill. By using cadavers to simulate participants' initial nerve blocks, under expert supervision, we aimed to reduce learner anxiety and accelerate the adoption of USGRA techniques on return to their institutions. The measure of course success was demonstrated by perceived increases in confidence immediately following the course but also by the sustained changes in clinical practice that had occurred at three-month follow-up. Most people are likely to report increased confidence immediately following an intensive period of instruction but this can rapidly disappear once the participant returns to their own institution without the support and guidance of experts surrounding them. We felt that by three months, participants either would have made a change and progressed, or would have lost the confidence to start.
Cadaver-based workshops for regional anaesthesia are not new but have been infrequently utilized.
16
This is in contrast to other specialties which have used cadavers for procedural training over many years with reported improvements in clinical outcome.
17–27
Several regional anaesthesia societies recognize the use of cadavers to enhance experience
28
or as a mandatory requirement for a diploma (see
There are limitations to the use of unembalmed cadavers for teaching regional anaesthesia. Availability can be limited, and few centres are routinely using them for training purposes. The ethical issues regarding the use of a rare resource have to be considered. Fresh frozen cadavers can be thawed twice before the remains are cremated or interred. Maximum utilization has to be a priority. Our course is scheduled to coincide with a surgical one so that each cadaver is utilized multiple times during each thaw. Cadavers can remain thawed for up to one week before re-freezing. Not all blocks can be performed, especially where vascular structures are used as a key landmark unless some method of restoring anatomy is used such as in our description.
However, unembalmed cadavers offer near normal tissue properties and more realistic tissue feedback during needle placement. Some nerves are much easier to image as demonstrated in Figure 3 showing the sciatic nerve after dividing into the tibial and common peroneal components.
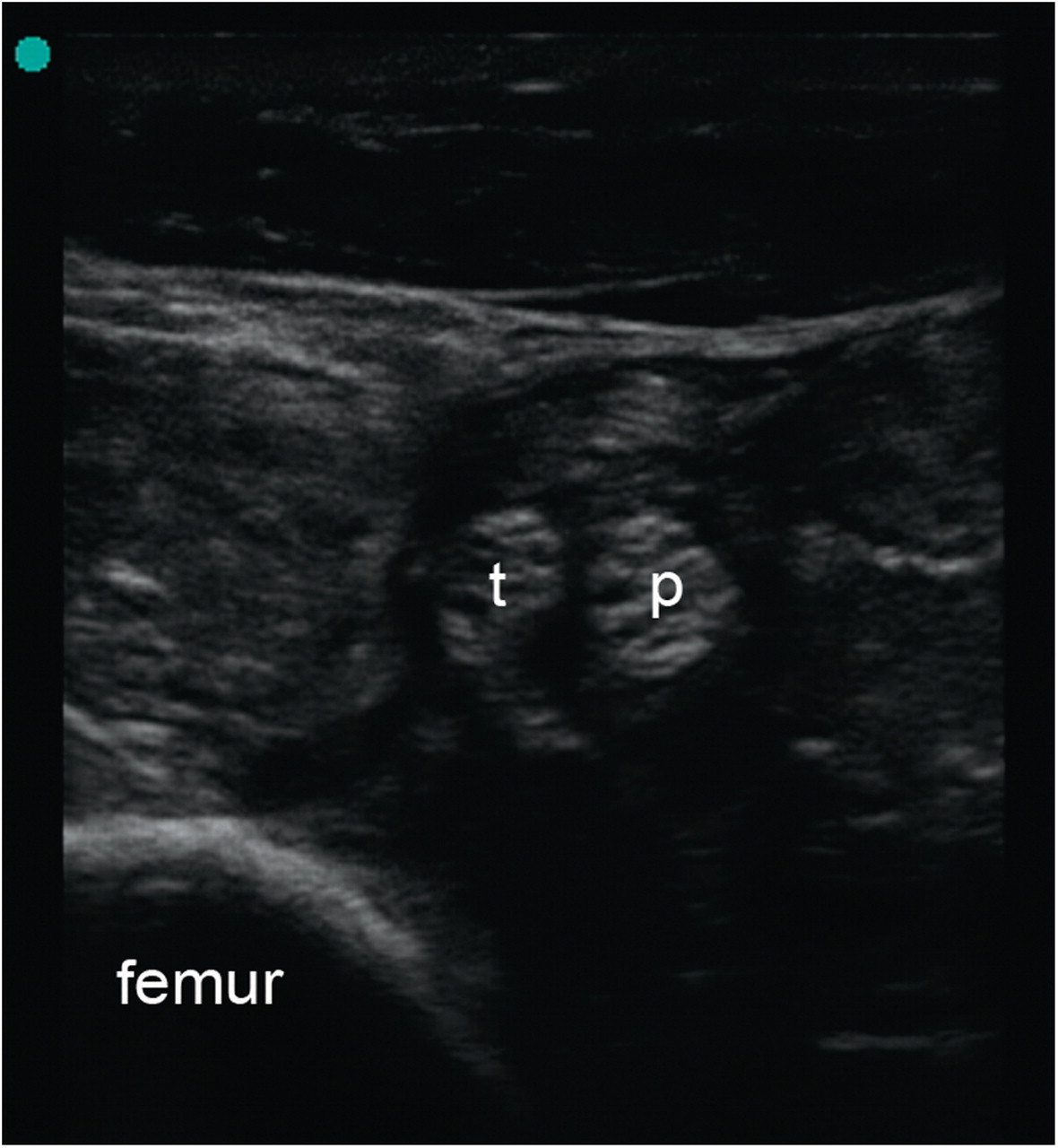
Ultrasound image showing the common peroneal nerve (p) and tibial nerve (t) proximal to the popliteal fossa in a fresh cadaver
It is probably no longer considered acceptable to practise on our patients. Increasing litigation behooves us to find better ways to learn skills, such that we are more experienced by the time we approach our patients. Using unembalmed cadavers can help bridge the gap between learning how to obtain an appropriate sonographic image and actually perform a nerve block. The ability to practise in a stress-free, non-clinical environment without time pressure or fear of patient discomfort enhances confidence and can lead to a sustained change in clinical practice as part of a multimodal USGRA course.
Footnotes
ACKNOWLEDGEMENTS
The authors wish to thank Dr W Weightman for his assistance with data preparation and analysis and SonoSite for the loan of ultrasound equipment. We would also like to thank the staff at the Clinical Training and Evaluation Centre, The University of Western Australia for their assistance in making the course possible (see
DECLARATIONS
The authors have no conflicts of interest to declare.