
Abstract
Dialysis access represents a lifeline for the patient with chronic kidney disease requiring renal replacement therapy. The gold standard is well recognized as the autogenous arterio-venous fistula. The surveillance and maintenance of access is therefore crucial to avoid access failure and subsequent morbidity, particularly through central venous catheterization.
Ultrasound examination should involve a review of the clinical history and both physical and sonographic assessment. The interpretation of the acquired information can lead to accurate diagnosis and instigate timely and appropriate treatment of malfunctioning access.
The purpose of this pictorial essay is to describe the complete evaluation of a dialysis access and review the findings associated with the most common pathologies.
The prevalence of haemodialysis-dependent patients is increasing. 1 Arteriovenous (AV) fistulae are the preferred method of haemodialysis due to a low infection risk and longevity of function. 2,3 AV grafts are a secondary choice, utilized in the absence of suitable venous anatomy for fistula creation, and have a higher infection risk and shorter functional duration. 2 Both forms of dialysis access can develop stenoses and fail. Unfortunately, locations for autogenous fistula creation are limited, and therefore fistula preservation is of paramount importance.
Ultrasound is widely recognized as an effective diagnostic method for stenosis detection. 4,5 The advantages of sonography include non-invasiveness, the capability to interrogate both intraluminal and surrounding soft tissue structures, the avoidance of contrast medium and the quantification of function through flow rate assessment. 5–7 An effective surveillance programme has the potential to identify problems and initiate treatment prior to fistula malfunction or complete failure, prolonging the life of the access. 7–9 This approach reduces the need for complex thrombectomy cases, temporary line placement and new fistula creation. The medical history and clinical examination findings are vital and when combined with sonographic findings may reveal accurate diagnoses.
Here, we aim to provide a concise review of dialysis access pathologies, focusing on the role of ultrasound in their detection.
Fistula anatomy
The anastomosis of an artery to a vein, usually in an end vein-to-side artery configuration, creates a low resistance circuit with a sufficiently high flow volume for dialysis. The access can be interpreted in relation to its component parts (Diagram 1); an anastamosis, an inflowing artery (proximal to the anastamosis), an outflowing artery (distal to the anastamosis) and the outflowing vein. All autogenous fistulae will have a swingpoint, the point at which the vein is mobilized towards the artery during surgical creation of the fistula. It is typically located approximately 2–3 cm above the anastomosis. The length of vein between the anastomosis and the swingpoint is called the juxta-anastomotic or peri-anastomotic segment.
10
Desirable fistula qualities include a minimum flow volume of 600 mL/minute to allow for acceptable uraemic toxin removal, and a minimal lumen diameter of 6 mm, for adequate needle access.
2,11
A digital subtraction angiography image displaying normal fistula anatomy. Labels: (1) the arterial inflow, (2) arterial outflow, (3) anastamosis, (4) juxta-anastamotic section, (5) swingpoint and (6) outflowing vein
Graft anatomy
Polytetrafluoroethylene (PTFE) grafts are used in the absence of suitable veins or arteries, and can be used to replace segments of the fistula circuit where integrity is a concern. Well-recognized graft formations include the loop graft and the brachio-axillary graft; however, when venous real estate is poor, more creative surgery may be attempted. PTFE grafts must achieve a higher flow volume than autogenous fistulae to maintain patency, with the desirable flow volume being in excess of 800 mL/minute. 8
Waveform interpretation
An adequately functioning fistula will display a low resistance monophasic waveform (Figure 1). The level of resistance visible within the cycle will vary in the presence of pathology. A significant outflow stenosis will increase proximal resistance within the circuit producing spectral waveform changes that may range from subtly defined systolic peaks to a waveform with a sharp systolic upstroke and low flow in diastole, more typical of an arterial waveform. The outflowing vein can be turbulent due to tortuousity and aneurysmal segments, therefore waveform analysis is best observed in the arterial inflow where flow is generally laminar. The flow volume can be measured using the equation: Flow volume = Time averaged velocity × πd2/4.

Normal arteriovenous fistula Doppler waveform from the radial artery: note a sharp systolic upstroke and a gently sloping downstroke with continuous forward flow throughout diastole
Common pathologies
Outflow stenosis
Stenoses in AV fistulae develop due to the altered haemodynamic state brought about by introducing arterial flow into a vein. This can result in hyperplasia in the intima-media complex. 12 Stenoses most commonly develop at the anastomosis, the juxta-anastomotic segment, the swingpoint and the terminal arch of cephalic fistulae. 10,13,14 Other areas commonly associated with stenosis include the puncture zones, vein bifurcations, pre-existing sclerotic veins, remnant valves and the central veins. 12 Graft stenoses are typically located at the graft-vein anastomosis. 12,15
Signs and symptoms
Decreased urea reduction ratio, increased pressures during dialysis, prolonged bleeding postdialysis and arm swelling.
Clinical examination
There will be increased pulsatility proximal to the stenosis due to increased resistance, with a thrill felt at the stenosis due to the increased velocity through the narrow segment. 16
Ultrasound appearance
Fibrous stenosis and involution of the vein (Figure 2);
Intimal hyperplasia with reduction in luminal diameter (Figure 3);
Decreased flow volume (critical in all stenoses if the flow is below 600 mL/minute);
High resistance waveform proximal to the stenosis (Figure 4);
Colour aliasing at the stenosis ±tissue vibration artifact;
High velocity through the stenosis;
Retrograde filling of veins proximal to the stenosis;
Dilated collateral veins.
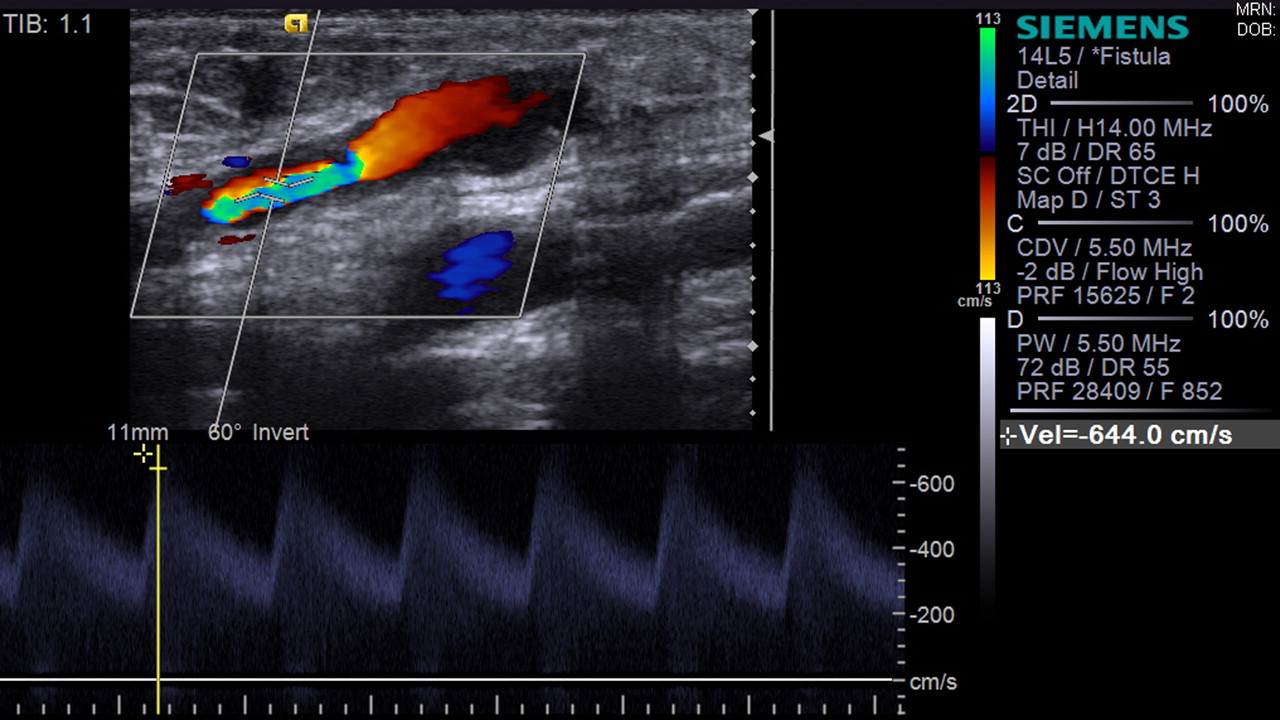
Axillary vein stenosis displaying aliasing in colour Doppler and a velocity in excess of 6m/s indicating a significant stenosis
Stenosis resulting from intimal hyperplasia

Arterial inflow monophasic waveform in the presence of an outflow stenosis. NB the systolic peaks are clearly defined due to increased resistance within the circuit
Useful information
When imaging in B-mode, a high gain setting is useful for the detection of intimal hyperplasia which can be echolucent on an otherwise optimal vascular setting. Once a stenosis has been identified, its significance should be quantified. Parameters including a diameter reduction of ≥50%, a diameter size of <2 mm and a peak systolic velocity of >400 cm/second are helpful when determining the significance. 7 Hyperechoic, slow, swirling flow alerts the operator to the risk of imminent occlusion and should instigate prompt fistuloplasty treatment.
Central vein stenosis
The haemodialysis population has a high incidence of central venous stenosis due to the placement of central venous catheters. The inability to visualize central vessels is a well-recognized failing of ultrasound. However, sonographic assessment of the access along with clinical findings can lead to accurate referral for further imaging and treatment.
Signs and symptoms
Decreased urea reduction ratio, ipsilateral limb swelling, prolonged bleeding postdialysis, dilated superficial chest collaterals, aneurysmal AV fistula, facial swelling (superior vena cava obstruction) which may be more prevalent in the morning after the patient has been supine.
Clinical examination
Pulsatile fistula, visible collateral network development, occasionally with a palpable thrill.
Ultrasound appearance
Pulsatile waveform;
Normal waveform in the presence of established collaterals;
Hyperechoic, slow flowing blood;
Retrograde or inhibited jugular venous flow;
Subcutaneous oedema;
Decreased flow volume.
Useful information
This is typically treated with venoplasty, with the potential use of stents where recoil stenosis is a concern. A history of previous central catheters and examination findings of arm or facial swelling can help guide intervention.
Inflow stenosis
Common aetiologies of renal failure include diabetes and hypertension. 15 Consequentially atherosclerotic disease and arterial calcification is prevalent in this population. The arterial supply to the fistula should be considered from the heart to the anastamosis when inflow disease is suspected. Arterial inflow disease can prevent fistula maturation, and results in access dysfunction due to poor flow volume. 15 In radiocephalic fistulae, inflow stenoses are physiologically compensated for by the ulnar artery that can supply the fistula via the palmer arch, reversing the flow direction in the outflowing radial artery. 17
Signs and symptoms
Failure to mature, difficulty needling.
Clinical examination
Small diameter access, impalpable or weak thrill, easily compressible outflow vein.
Ultrasound appearance
Calcified arterial walls ±visible stenosis;
Low flow volume (less than 600 mL/minute flow volume);
Low resistant outflow vein;
In radiocephalic fistulae, reversal of arterial outflow if the palmer arch is intact.
Useful information
Measure reversed outflow volume – this may be sufficient to support the fistula and dialysis;
When an inflow stenosis cannot be detected with ultrasound consider echocardiography ±CT angiography to determine the site of lesion.
Arterial inflow stenoses can be treated by balloon angioplasty, or alternatively by proximalizing the anastomosis surgically. Factors including the age of the access and severity of the stenosis will be considered when determining the most suitable form of treatment. When there are multiple treatment options available, a multidisciplinary team meeting allows consideration of all possibilities and selection of suitable treatment on an individual patient basis.
Thrombosis
Thrombosis of the fistula is caused by the increasing resistance and continuous flow reduction that occurs secondarily in the presence of an undetected significant stenosis. 8 Stenosis detection using ultrasound in the presence of thrombosis may be difficult, as differentiation between intimal hyperplasia and thrombus load may not be possible. However, fibrous stenoses should be easily recognized.
Signs and symptoms
Painful access, erythema, inability to dialyse.
Clinical examination
Loss of thrill, firm ‘rope like’ access.
Ultrasound appearance
Hyperechoic thrombus causing stenosis or occlusion (Figure 5);
High resistant arterial inflow waveform – triphasic in occlusion;
Hyperechoic, slow, swirling flow may be detected in the presence of imminent thrombosis;
Absence of flow on colour Doppler interrogation.

Thrombosed fistula
Useful information
The arterial inflow and outflow should be examined carefully for intra-arterial extension of thrombus as this may complicate interventional or surgical therapy. Infection must be excluded clinically before intervention.
Steal syndrome
Steal syndrome describes peripheral ischaemia in the presence of a more proximal fistula. It occurs as a result of preferential flow through the low-resistant fistula, causing reduced flow in the distal high-resistant arteries, and poor perfusion of the distal limb. 18 Steal syndrome can be caused by arterial inflow or outflow disease. 15,19 Steal syndrome should not be confused with the normal occurrence of retrograde flow found in the outflowing radial artery of radiocephalic fistulae, as 70% of radiocephalic AV fistulae receive blood from the ulnar artery via the palmer arch without detriment to the hand. 19 Ultrasound can be used to assess the fistula flow volume and assess the flow volume being received by the hand via the ulnar and radial arteries; it cannot, however, diagnose steal independently and should be used as an aid to clinical diagnosis.
Signs and symptoms
Cold hand, pallor, ischaemia, ulceration.
Clinical examination
Cold hand, normal AV fistula, reduced or absent distal pulses.
Ultrasound appearance
The fistula will exhibit normal function;
Small diameter radial and ulnar arteries;
Atherosclerotic arteries;
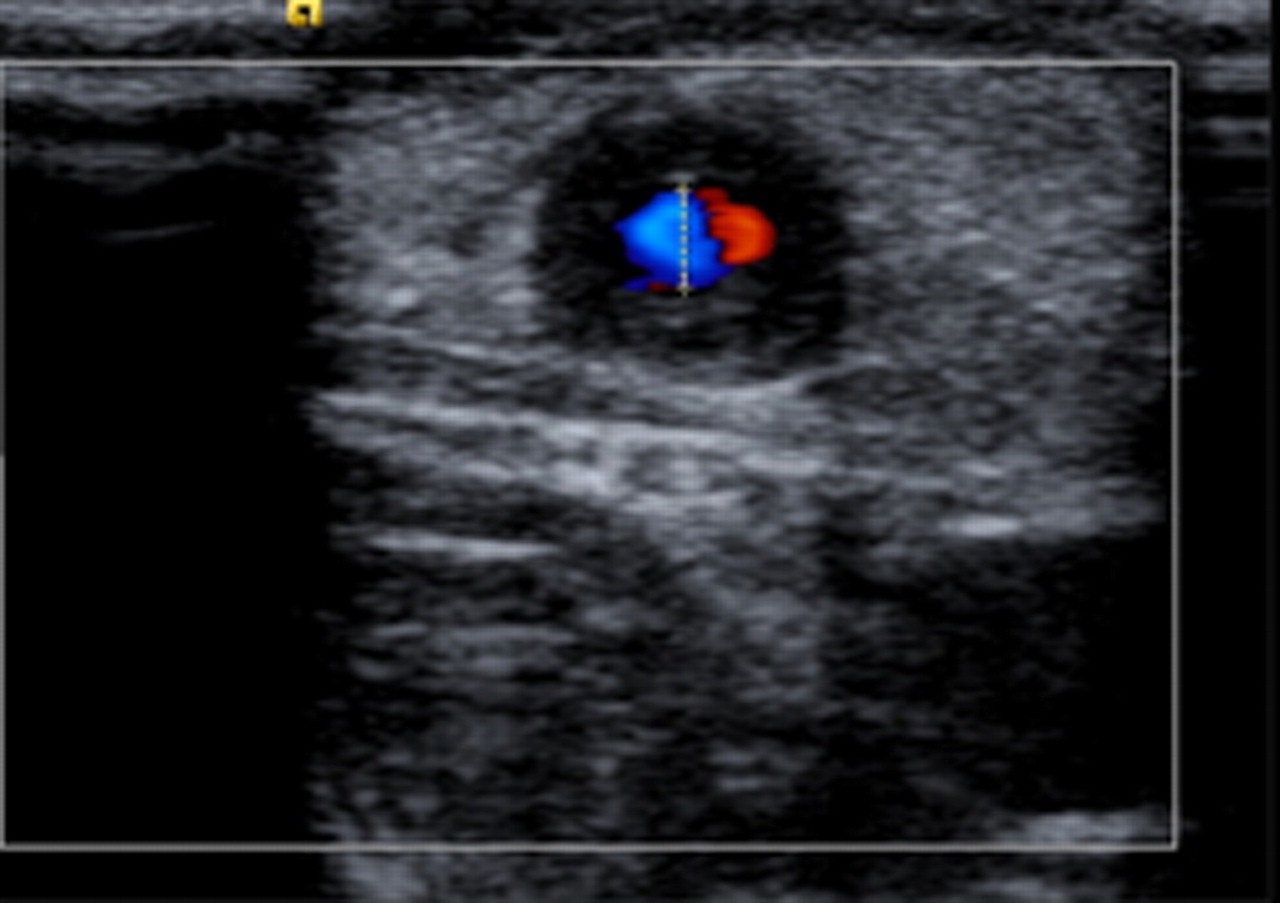
Damped flow in distal arteries (Figure 6).

Damped radial artery waveform in the presence of an upper arm fistula
Useful information
Check carefully the ulnar and radial arteries for an accurate flow volume and the direction of flow. Power Doppler may be useful in their identification when small or calcified. If colour Doppler fails to map the artery, spectral Doppler alone may produce a waveform. Compression of the access may revert the arterial outflow waveforms to normal.
Treatment is typically surgical involving arterial bypass or ligation of the access.
Pseudoaneurysm
A pseudoaneurysm is a complex haematoma which exhibits flow following the disruption of the vessel wall. It poses a great threat to the integrity of the fistula, especially in the presence of an outflow stenosis, where elevated pressures can result in rupture. Pseudoaneurysms may develop as a result of multiple cannulations, causing breakdown of the vessel wall. 12
Signs and symptoms
Sudden swelling over the access, possibly in association with traumatic needling or injury. Haemorrhage.
Clinical examination
It may be difficult to distinguish from a true aneurysm without ultrasound.
Ultrasound appearance
May arise from arterial or venous components;
Haematoma containing flow (Figures 7a and b);
There may be an associated needling tract.

(a) and (b): PTFE graft with breakdown and associated pseudoaneurysm
Useful information
The thickness of the overlying skin should be evaluated and assessed for signs of potential breakdown. The access should be examined for signs of compression as a result of the pseudoaneurysm. An outflow stenosis should be excluded, as its presence may prompt rapid treatment. Pseudoaneurysms may be dealt with interventionally with a stent graft and fistuloplasty of distal outflow stenoses, or by surgical excision and repair.
Tributary steal
Where there are multiple venous tributaries of similar diameter present at fistula formation, preferential maturation of a single vein may not occur, producing numerous low volume outflowing veins that are singly unsuitable for dialysis.
Signs and symptoms
Poor maturation of a single vessel. Problems needling.
Clinical examination
Multiple dilated veins in the arm.
Ultrasound appearance
Normal low-resistant arterial inflow volume;
Single or multiple tributaries causing flow division;
Tributaries can be of a similar calibre to the fistula or be multiple and small.
Useful information
Determine the flow volume in the departing tributaries. The offending vessels can be identified and treated by ligation or embolization. Observe fistula flow prebranch, within the branch(es) and postbranch to observe for signs of a significant re-direction of the flow.
Infection
Infection can occur in autogenous fistulae, but is more often associated with grafts. Careful interrogation of the graft/ fistula throughout its length is required, examining for interstitial fluid and/or collections of fluid surrounding the graft/fistula (Figure 7). Access breakdown is a serious complication of infection making accurate diagnosis crucial.
Signs and symptoms
Painful, hot, skin breakdown.
Clinical examination
The arm may be erythematous, hot, swollen and painful. In extreme cases there may be skin breakdown.
Ultrasound appearance
Anechoic region surrounding the graft indicating a collection;
Interstitial fluid;
Thrombus within the access;
Graft/fistula breakdown;
Sinus/tract;
Inflammatory changes surrounding the vessel (Figure 8).
Patent PTFE graft with surrounding infection, manifesting as a region of mixed echogenicity around the graft
Useful information
Infection can present with similar symptoms to thrombosis. Urgent therapy is required to avoid complications including haemorrhage, septicaemia and septic embolism.
Seroma
A seroma is described as a sterile collection of clear, ultrafiltered serum, surrounded by a non-secretery fibrous soft tissue pseudocapsule and is typically associated with AV grafts. Intermittent surveillance may be indicated to monitor seroma size. If left untreated they can resolve without the need for intervention. However, persistent seroma can become infected and can result in graft loss. 20
Signs and symptoms
Local swelling. If the seroma is infected there may be symptoms associated with infection and/or thrombosis.
Clinical examination
There may be no evidence of its presence during clinical examination. A localized swelling may be palpable. If it has become thrombosed or infected, the area will exhibit associated symptoms.
Ultrasound appearance
Anechoic region surrounding the graft, which may continue for the length of the graft (Figure 9).

PTFE graft with surrounding seroma
Useful information
Can be difficult to distinguish from a haematoma – must be ultimately decided clinically or by diagnostic aspirate.
Haematoma
Often a haematoma is identified clinically, with ultrasound being used to examine its extent, effect and exclude a pseudoaneurysm. Causes can include needle misplacement or movement during dialysis causing extravasation into the surrounding tissues.
Signs and symptoms
Pain, swelling and echymosis.
Clinical examination
The limb may feel under tension, making fistula palpation difficult.
Ultrasound appearance
Anechoic or mixed echo region surrounding the fistula;
Interstitial fluid;
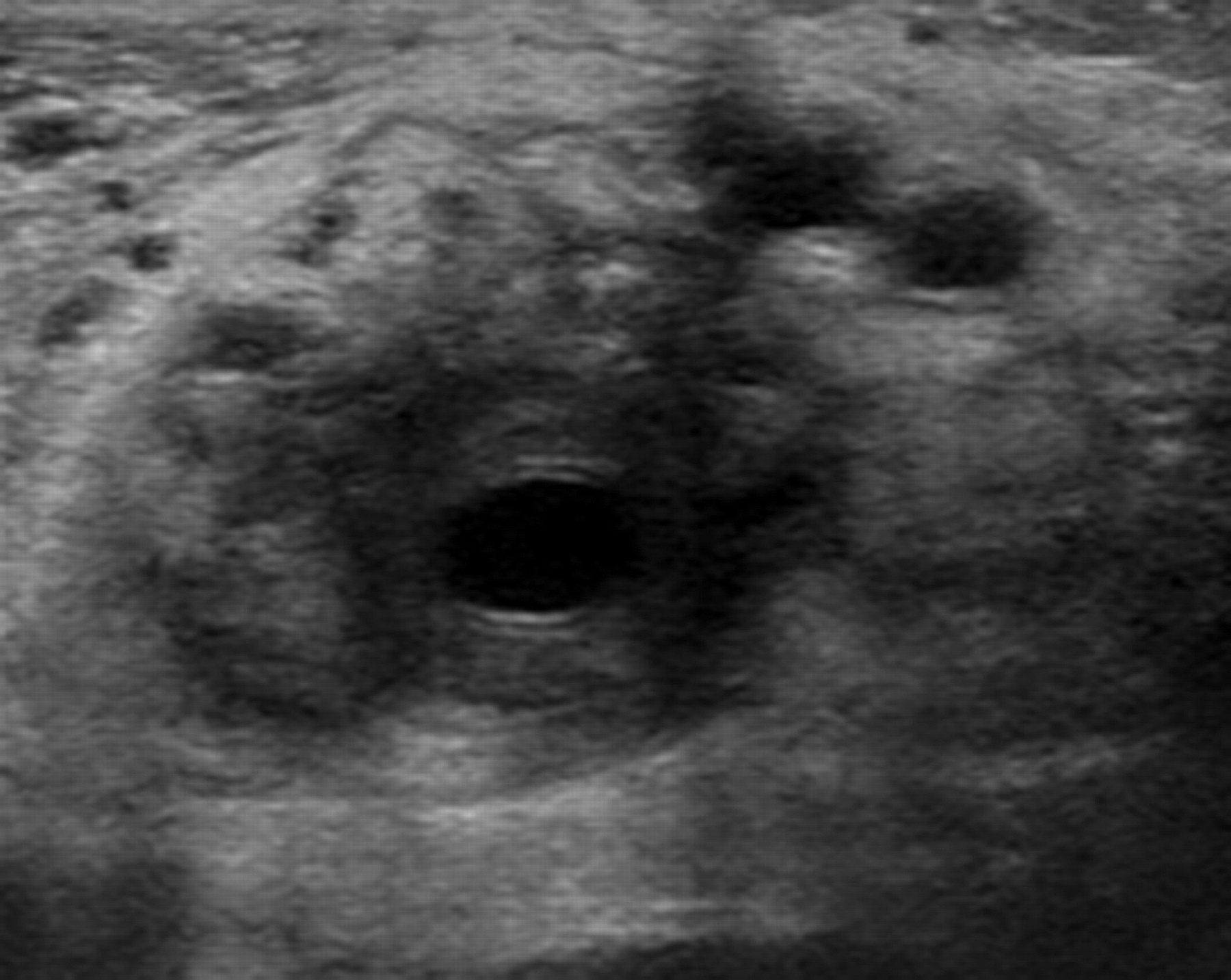
Possible compression of the access (Figures 10a and b).

(a) LS imaging cephalic fistula demonstrating compression caused by a haematoma. Luminal diameter measurements have been recorded in B-mode to exclude over-estimation of vessel diameter caused by tissue vibration artefact with colour Doppler. (b) TS imaging of fistula compression caused by haematoma
Useful information
Usually haematomas resolve spontaneously. Compression can lead to access thrombosis. Haematomas can become infected.
High output cardiac failure
This is a rare complication of the hyperkinetic state of high flow fistulae. Fistula formation results in reduced peripheral resistance and therefore increased cardiac output. 3,21 Fistula flow volumes of 1.5–2 L/minute have been associated with high output cardiac failure in several studies; however, these values cannot diagnose this pathology alone as optimally functioning fistulae can exhibit these values, making clinical correlation essential.
Signs and symptoms
Large calibre fistula, dyspnoea, orthopnoea, paroxysmal nocturnal dyspnoea and oedema. 22
Clinical examination
Large diameter access, elevated jugular venous pulse, breathlessness during exercise or at rest, tiredness and swollen ankles/feet.
Ultrasound appearance
Large diameter, high flow access (Figure 11).

High flow volume recorded in the inflowing artery
The most reliable flow volume is often found in arterial inflow as the outflowing vein will be dilated and often turbulent.
Useful information
High output cardiac failure is a clinical diagnosis. Patients can function with high flow fistulas without experiencing cardiac problems, therefore high flows are not pathognomonic. Surgical reduction of the fistula may be required if high output cardiac failure is confirmed.
Conclusion
A methodological approach to scanning and a thorough knowledge of the pathologies of dialysis access are required to ensure consistency of access surveillance and to allow prompt instigation of an appropriate therapy when indicated.
DECLARATIONS
The authors have no conflicts of interest to declare.