
Abstract
Bedside, focused or point-of-care ultrasound (PoCUS) is becoming an established technique within emergency and critical care medicine to answer time-dependent, focused clinical questions. Bedside sonography is not a complete radiological investigation, rather an extension of the clinical examination to rule in or rule out key diagnoses in specific clinical settings. PoCUS is geared to addressing highly time-dependent and focused questions, and in general most focused scans become more obviously positive as the patient becomes increasingly unwell. In the hypotensive patient, one of the first questions a clinician must address is whether the patient requires emergency fluid resuscitation. That is, is the patient under-filled or overloaded? So, how can we use ultrasound to add value to our clinical assessment of filling in the hypotensive patient?
Question
Among patients presenting to the emergency department with non-traumatic hypotension, how can point-of-care ultrasound (PoCUS) be used to identify hypovolaemia and accurately guide fluid resuscitation?
Introduction
Bedside ultrasound, or PoCUS, is becoming an established technique within emergency and critical care medicine to answer time-dependent, focused clinical questions. Bedside sonography is not a complete radiological investigation, rather an extension of the clinical examination to rule in or rule out key diagnoses in specific clinical settings. 1 PoCUS is geared to addressing highly time-dependent and focused questions, and in general most focused scans become more obviously positive as the patient becomes increasingly unwell.
In the hypotensive patient, one of the first questions a clinician must address is whether the patient requires emergency fluid resuscitation, i.e. is the patient under-filled or overloaded? So, how can ultrasound be used to add value to the clinical assessment of filling in the hypotensive patient?
Hypotension evident in the emergency department is a predictor of in-hospital mortality, with rates as high as 25%. 2 It is also known that clinical assessment can fail to determine the correct cause, with one study showing that the correct aetiology in patients with undifferentiated hypotension is identified in only 24% of cases. 3 Determining the underlying haemodynamic process in a timely and accurate fashion should allow successful goal-directed therapy. Invasive monitoring techniques can be time-consuming, costly, and are not always easily performed in the emergency department. Non-invasive techniques, such as ultrasound, are rapid and within the remit of most emergency physicians.
Inferior vena cava (IVC) measurement and its collapsibility have been shown to correlate with central venous pressure (CVP) 4–7 with the strongest correlation seen at extremes of the values in low or high volume states. 5,6
Protocols for goal-directed sonography have been proposed and have been shown to result in fewer viable diagnostic aetiologies and a more accurate physician impression of final diagnosis in the evaluation of non-traumatic, symptomatic, undifferentiated hypotension in adult patients. 8,9 In hypotensive patients, the rapid non-invasive assessment of intravascular filling pressures and identification of possible aetiologies for shock helps to refine and guide the initial resuscitation, further investigations and interventions. It is vital that the pursuit of the underlying aetiology does not delay supportive therapy and appropriate early resuscitation, and this is where focused scanning of the venous capacitance vessels, especially the IVC, can help.
Case example
A 25-year-old obese man with a past history of significant massive pulmonary emboli presented to the emergency department with a three-day history of significant haemoptysis. He was not currently anticoagulated. He was initially hypotensive (75/40 mmHg) with evidence of air hunger. He responded to initial fluid resuscitation. A chest radiograph showed findings that could have been consistent with either an infarct or infection. He was too large for the computed tomography scanner. Thrombolysis was considered; however, a focused ultrasound examination of his IVC as part of an ACES scan (abdominal and cardiac evaluation with sonography in shock) revealed an under-filled, small, collapsing IVC. This evidence, along with other ultrasound findings of a hyperdynamic heart with normal right ventricular size, and no evidence of femoral thrombosis, guided the initial resuscitation efforts away from thrombolysis and towards fluid resuscitation and treatment for septic shock secondary to pneumonia.
Further fluid boluses improved his condition and subsequent investigation confirmed sepsis secondary to pneumonia as the cause for his presentation.
In the emergency setting, time critical interventions are essential, and resuscitation of the hypotensive patient often cannot wait until formal cardiac imaging or invasive monitoring is available. Measurement of the IVC and its collapsibility has been shown to be a valuable method of predicting fluid responsiveness. 10 Fluid responsiveness describes the significant increase in cardiac output that results from volume expansion. 11
The IVC is a major capacitance vessel, facilitating consistent venous return to the right heart. As such, it changes its diameter in a non-linear fashion in response to the filling status of the patient, increasing in diameter with increased filling pressure and volume. As well as the changes in the absolute diameter with changes in volume, in a haemodynamically normal, spontaneously ventilating patient, the IVC collapses slightly on inspiration. This is reversed in a mechanically ventilated patient where there is an increased diameter in the abdominal IVC during inspiration.
The collapsibility of the IVC (or collapse index) is calculated as the change in diameter during ventilation (either spontaneous or mechanical) divided by the maximal diameter (Table 1). This measurement is also used to assess the filling status of the patient.
The examination
The IVC can be visualized by ultrasound using either a curvilinear or phased array transducer, in both the longitudinal and the transverse planes using a subcostal, or a transhepatic window (Figure 1). The IVC is identified lying posterior to the liver receiving hepatic veins ventrally before it passes through the diaphragm and into the right atrium (Figure 2). M (motion) mode measurements of minimal and maximal diameter can be made across the proximal IVC (Figure 3).
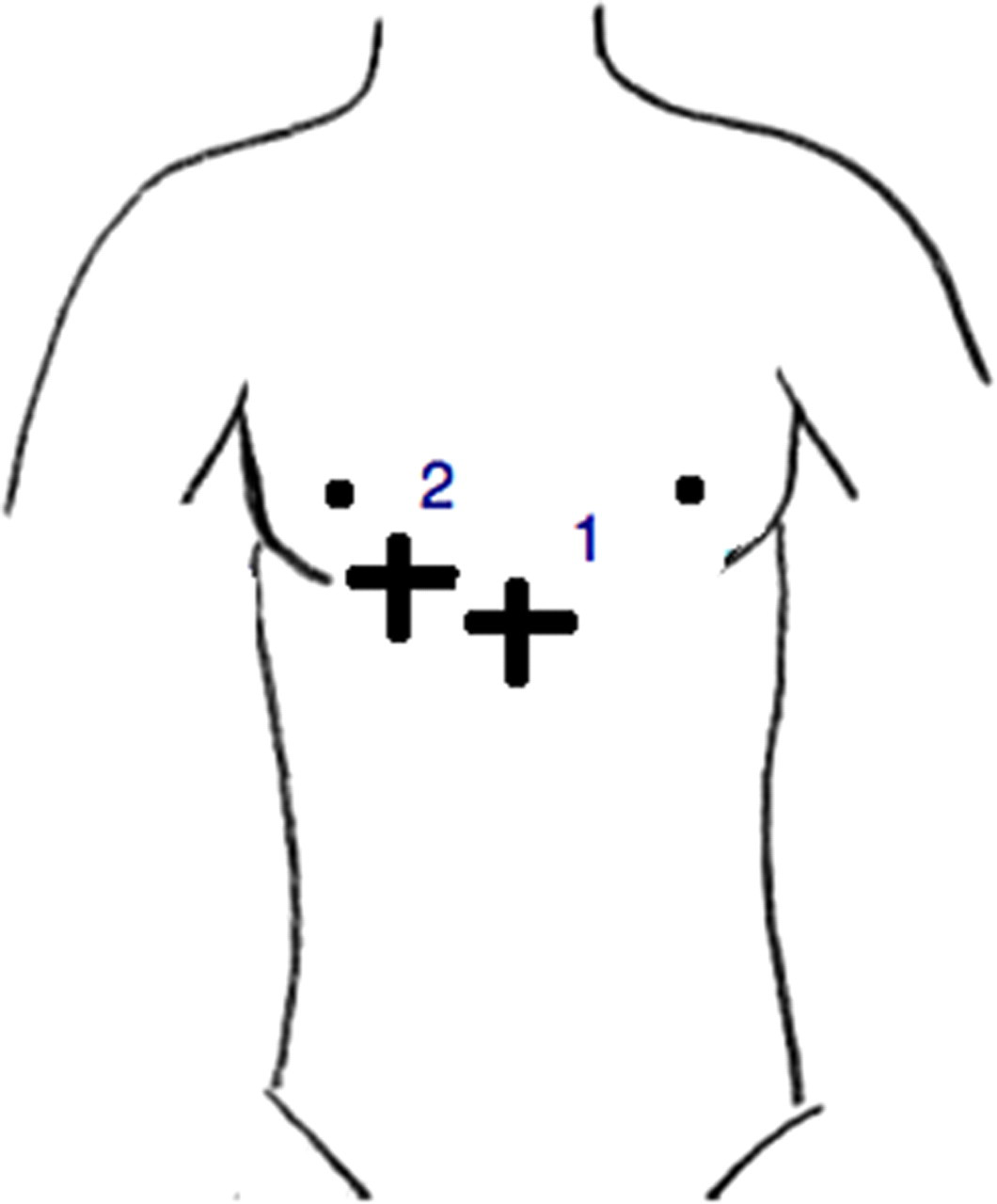
Longitudinal and transverse inferior vena cava views, either in the subcostal or in the transhepatic windows

Subcostal longitudinal view (cardiac orientation) of the inferior vena cava in expiration (a) and inspiration (b) demonstrating inspiratory collapse

Subcostal longitudinal view (abdominal orientation) of the inferior vena cava with M-mode measurement of inspiratory collapse
Does the transducer or patient position matter? There is evidence that movement of the diaphragm can influence the IVC measurement at the right atrial junction, and therefore measurements should not be made at that point. 12 Preferred sites are the junctions of the IVC with the hepatic veins and the junction at the left renal vein. Diaphragmatic movement may cause the IVC to move in and out of the longitudinal plane leading to a false impression of collapse.
While it may be more useful to measure trends of IVC diameter and collapsibility in response to fluid resuscitation, there is evidence for cut-off values which indicate an under or overfilled status. A maximal IVC diameter of less than 2 cm with inspiratory collapse of more than 40–50% indicates a right atrial pressure of less than 10 mmHg. Conversely, a diameter of greater than 2 cm with collapse of less than 40–50% suggests a pressure of greater than 10 mmHg (Table 1). 13,14
In terms of filling and fluid resuscitation, an initially small IVC diameter with significant or complete collapse indicates a low volume status that would respond to volume loading. A large dilated IVC with no, or minimal, collapse implies high CVPs and a state that would not respond to volume resuscitation alone. Further investigation and the use of other agents would be required to improve the cardiovascular status. 15 Again, these measurements should be repeated during resuscitation to guide optimal volumes and rates of intravenous fluid administration.
IVC size and collapse must be considered in association with ventricular size, wall motion and the presence or absence of pericardial fluid. A small chamber size with hyperdynamic wall motion on the cardiac view is consistent with hypovolaemia. Potential causes of hypovolaemia can be diagnosed by further ultrasound views of the right and left flanks, pelvis and lungs, aiming to detect significant haemoperitoneum or haemothorax, and of the abdominal aorta to identify the presence of abdominal aortic aneurysm. As such, PoCUS of the IVC is often incorporated into a shock protocol such as ACES. 15
Potential pitfalls
Caution is required when comparing PoCUS measurement of the IVC to CVP measurements, as this itself is a surrogate marker for filling status and may be unreliable as a guide. A systematic review to assess the techniques available for assessing intravascular volume found no correlation with circulating blood volume and stated that CVP did not predict fluid responsiveness. 16 It is important to interpret these IVC signs within the clinical context and not as a definitive measure of right atrial pressure or intravascular volume, as there is lack of high level evidence in the setting of critical illness.
How easy is it to obtain adequate views? In studies reporting IVC scanning in hypotensive patients in the trauma, emergency and ICU settings, the number of patients where the IVC could not be visualized ranged from 3% to 11% of their study population. The level of ultrasound experience was high; all of the sonographers had prior experience of bedside ultrasound and most had had specific additional didactic teaching on the technique. 4–7,17,18
Are the actual measurements made in the emergency setting accurate? When comparing emergency physician IVC measurement with formal ECHO, there was agreement in only 68.1% of patients (κ = 0.41). 19 These emergency physicians were all certified as proficient in ultrasound. 19 This finding may be specific to the individuals' training, or may indicate the difficulties encountered in the emergency setting. It is important to remember this limitation which again emphasizes the need to correlate ultrasound and clinical findings and to repeat measurements and to ensure visualization of the vessel in more than one plane.
How long does the measurement take? No studies have formally assessed the time taken to perform IVC measurement; however, anecdotal experience reported three minutes. The purpose of the scan is to be an adjunct in the first few minutes of assessment of the hypotensive patient.
It is also important to be aware of disease processes that will make it difficult to accurately interpret IVC measurements, e.g. moderate/severe tricuspid regurgitation, atrial fibrillation and raised intra-abdominal pressures. IVC compliance decreases with age with a recent study showing a decrease in the maximal diameter of the IVC with age and subsequently a greater IVC collapsibility; however when analysed the range was still within normal parameters. 20
Conclusion
IVC measurement seems to have most value as part of a goal-directed protocol. The ACES protocol and the similar Rapid Ultrasound in Shock (RUSH) exam 15,21 both include elements of the FAST (focused assessment with sonography for trauma) examination and a focused ECHO with IVC measurement included. There is evidence that early use of PoCUS shock protocols result in fewer possible diagnostic aetiologies and a more accurate physician impression of the final diagnosis. 8
Assessment of CVP can also be estimated by the height of the jugular venous column (ultrasound measured JVP), and this can be useful in a patient who is able to sit at 45°. 22 This approach is less useful in the hypotensive patient who is also supine.
Integration of PoCUS of the IVC into a clinical algorithm is essential. Figure 4 provides a possible (unvalidated) approach. When a patient with undifferentiated shock presents, resuscitation is initiated following a standard ‘ABC’ approach. A focused IVC ultrasound scan is performed, with measurement of the diameter and collapsibility if there is diagnostic uncertainty. If the diameter is normal or reduced (<2 cm) and the collapsibility index is greater than 50%, resuscitation with fluids for a hypovolaemic state is commenced. If the diameter is increased, with minimal collapsibility, then other causes of hypotension should be sought. While IVC measurement is a useful part of the assessment of the shocked patient, it is likely that it will be most useful as part of a bedside focused ultrasound protocol.

Proposed algorithm for integration of point-of-care ultrasound of the inferior vena cava (IVC) into clinical assessment of the hypotensive patient. VTE, venous thromboembolism
DECLARATIONS
The authors have no conflicts of interest to declare.