
Abstract
Dermoid cysts (mature cystic teratoma) are the commonest germ cell neoplasm and in some series the most commonly excised ovarian tumour. They are composed of tissue from at least two of the germ cell layers and often contain hair, sebum and teeth. These tumours show a wide range of ultrasonic appearances because of their variable composition. On account of this they may mimic a variety of other pelvic masses. In many cases, however, the ultrasonic appearance can be distinctive, and a number of sonographic signs characteristic of dermoid cysts have been described. Typical appearances include a shadowing echodensity or dermoid plug; diffuse or regional high amplitude echoes; the tip of the iceberg sign; dermoid mesh; fat–fluid levels and intracystic floating balls. When two or more characteristic signs are present, a high positive predictive value and a confident sonographic diagnosis can be achieved.
We present a pictorial review of the characteristic sonographic signs helpful in making the diagnosis of ovarian dermoid cyst. We also discuss the pitfalls of making an ultrasound diagnosis, and illustrate some of the conditions that may mimic dermoid cysts. We include correlation with computed tomography and magnetic resonance imaging where appropriate.
Keywords
The dermoid cyst or mature cystic teratoma is the commonest germ cell tumour, accounting for up to 25% of all ovarian tumours. 1 These masses are composed of tissue from at least two of the three germ cell layers (ectoderm, mesoderm and endoderm), but the composition is variable and this results in a wide range of possible sonographic appearances. They are often cystic, sebum being liquid at body temperature, and often contain hair or teeth. They are usually found in women of reproductive age, with an average age of 30 years, but may be found at any age from infancy to old age, and they are the commonest ovarian tumour in children. 2 Ovarian teratomas are bilateral in 10% of cases. The rate of malignancy found in pathological series varies from 0.17% 3 to 3%. 4 Dermoid cysts are often asymptomatic and discovered incidentally 1 although abdominal pain, distension or other non-specific symptoms may be present. The potential for complications, which include torsion, rupture and malignant transformation, means that surgical treatment is often necessary 1 although the surgical techniques used differ significantly from those performed for malignant ovarian neoplasms. This makes the distinction between dermoid cysts and malignant neoplasms very important.
The variability of sonographic appearances and the potential diagnostic pitfalls due to features that may mimic other pathologies have led to some authors describing difficulty in diagnosing dermoid cysts with ultrasound (US). 5 However, mature cystic teratomas often show characteristic features, including the dermoid plug, tip of the iceberg sign and dermoid mesh. When two or more characteristic features are present in combination, a confident sonographic diagnosis is possible and a very high positive predictive value may be achieved. 6
Here we review and illustrate the characteristic features of the ovarian dermoid cyst which are helpful in making a sonographic diagnosis.
Characteristic signs
Shadowing echodensity (Rokitansky nodule or dermoid plug)
This is the commonest manifestation present in cystic teratomas. 7 At US this appears as a focal, usually rounded hyperechoic protuberance from the wall which projects into the low echogenicity cyst cavity, often but not always with dense acoustic shadowing posteriorly. Hair usually arises from this area, and when teeth and bone are present they are usually found in this area. 8

(a–c) Dermoid plug/Rokitansky nodule. A rounded hyperechoic focus casting a dense acoustic shadow, typical of a Rokitansky nodule, is seen arising from the wall of a dermoid cyst (a). T1 weighted (b) and fat saturation (c) magnetic resonance images confirm the presence of fat
Diffuse or regional high amplitude echoes
This is the second commonest manifestation. Increased echogenicity within a mass is common to many dermoid cysts and the diagnosis should be considered when this feature is seen. A diffuse or focal hyperechoic area is often present which causes sound attenuation. This is due to the presence of mixed sebaceous material and hair 8 and this can result in the tip of the iceberg sign. The increased echogenicity may be diffuse and seen throughout the mass (see Figures 2a–d), or may be more focal. When focal this may be nodular in distribution (see Figure 3), or may be seen in association with compartments of different echogenicity which can be due to layering (Figures 4a–d).

(a–d) Diffuse high echogenicity. High level echoes throughout a left adnexal mass, with associated posterior acoustic shadowing (a). T1 weighted (b), T2 weighted (c) and fat saturation sequences confirm left adnexal dermoid cyst and simple right ovarian cyst

(a–c) Peripheral nodular bright echoes with little acoustic shadowing (a), T1 (b) and FS (c) magnetic resonance sequences confirm fat within these nodules

Fat–fluid levels. Hyperechoic and cystic components within masses, separated by a linear interface, are in keeping with a fluid/sebum layer, but in isolation on ultrasound, a layered appearance is not specific for dermoid cyst. Mass with anterior anechoic component and dependent more hyperechoic component (a). Sagittal T1 weighted (b) and axial fat saturation (c) confirm the fatty sebum floating above more complex fluid. (d) Linear interface within a partly hyperechoic mass, in this case with a hyperechoic superior component, and with focal echogenicity in keeping with hair floating at the interface
Tip of the iceberg sign
This is a specific sign of a dermoid cyst. The tip of the iceberg refers to the presence of a hyperechoic mass with deep beam attenuation which obscures the posterior border of the mass, making the deeper aspect of the mass difficult to appreciate. The extent of the mass may thus be underestimated (see Figures 5a and b). This feature is particularly important to consider when there is a palpable mass present clinically. Recognition of this sign reduces the chance of a false-negative interpretation and confusion with a ‘bowel gas pattern’. 9
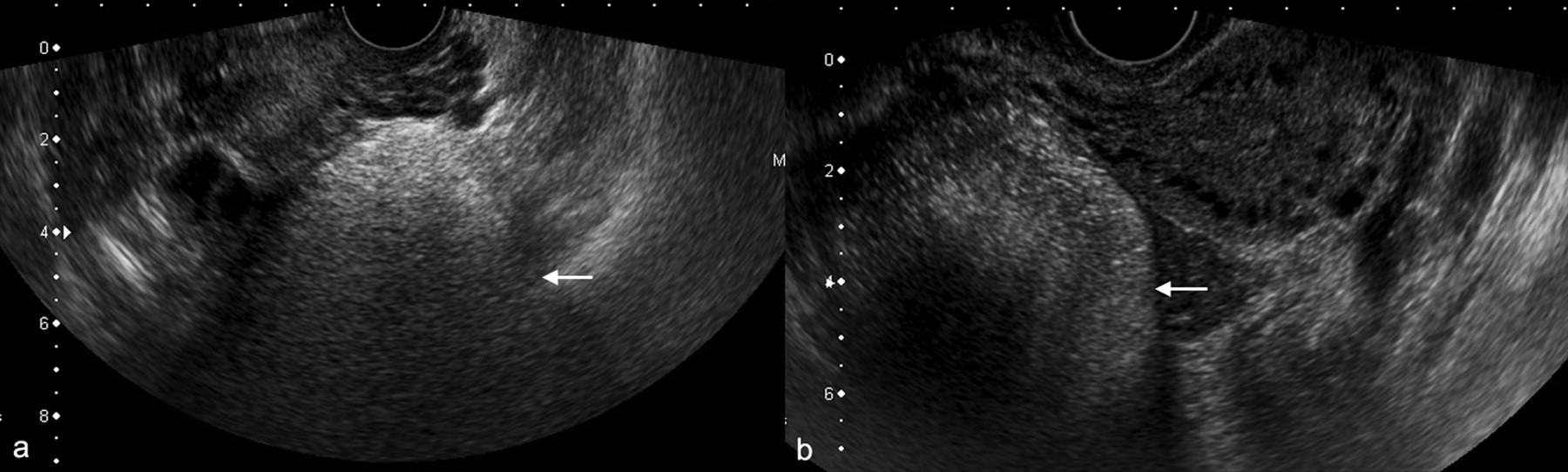
Tip of the iceberg. Two examples (a, b) where posterior acoustic attenuation from a hyperechoic mass makes the deep aspect of the mass difficult to appreciate
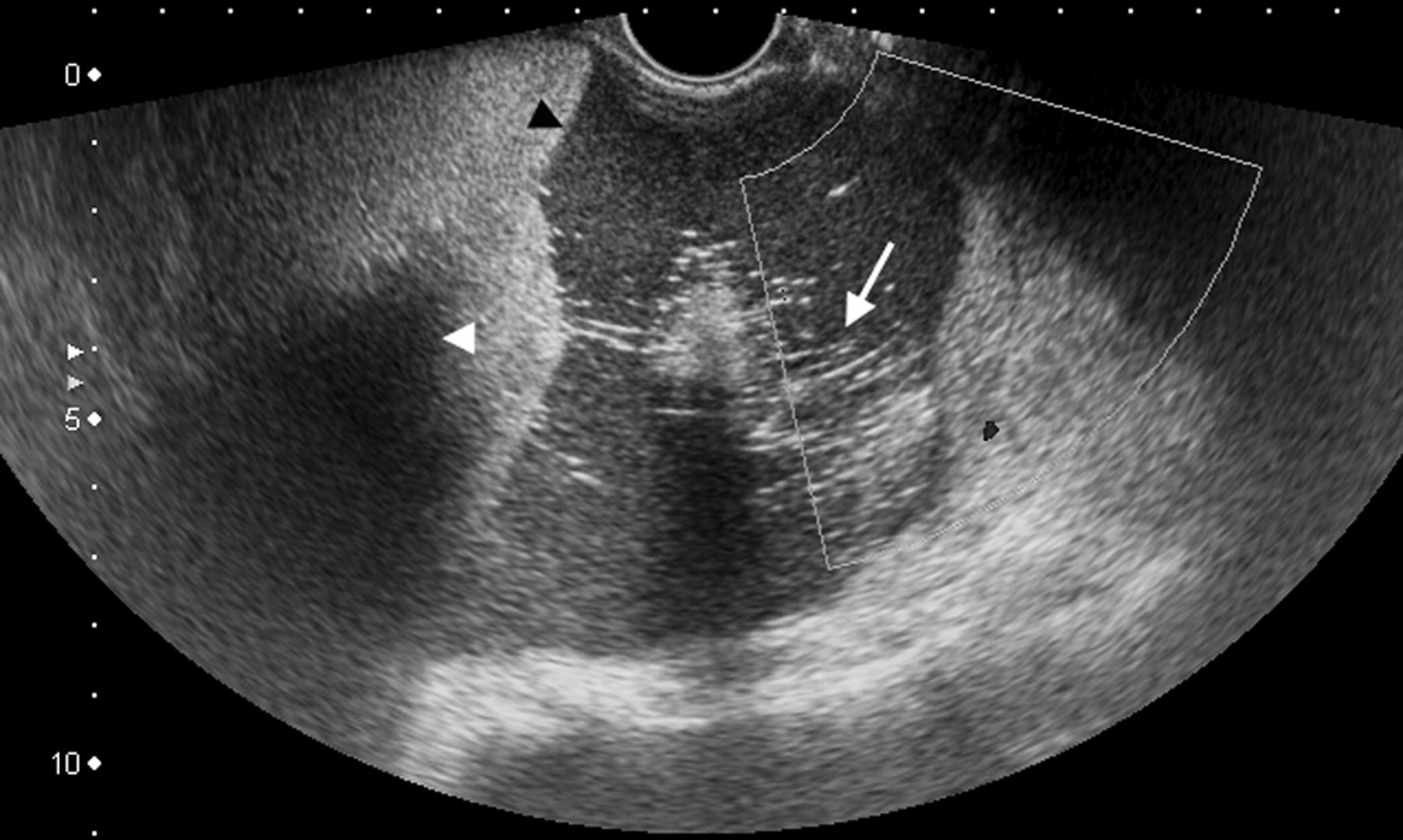
Dermoid mesh
This is the third commonest sonographic manifestation of a dermoid cyst. The term refers to the presence of hyperechoic linear echoes and dots, which are thought to be due to the presence of hair floating within the cyst. 10 At US this is seen as high reflectivity lines and dots which can be present throughout the mass or focally within the cyst (see Figure 6). This finding has been shown to be associated with a very high positive predictive value and is very commonly found in association with another characteristic finding. 6

Dermoid mesh. High reflectivity lines and dots thought to be due to the presence of hair floating within the cyst
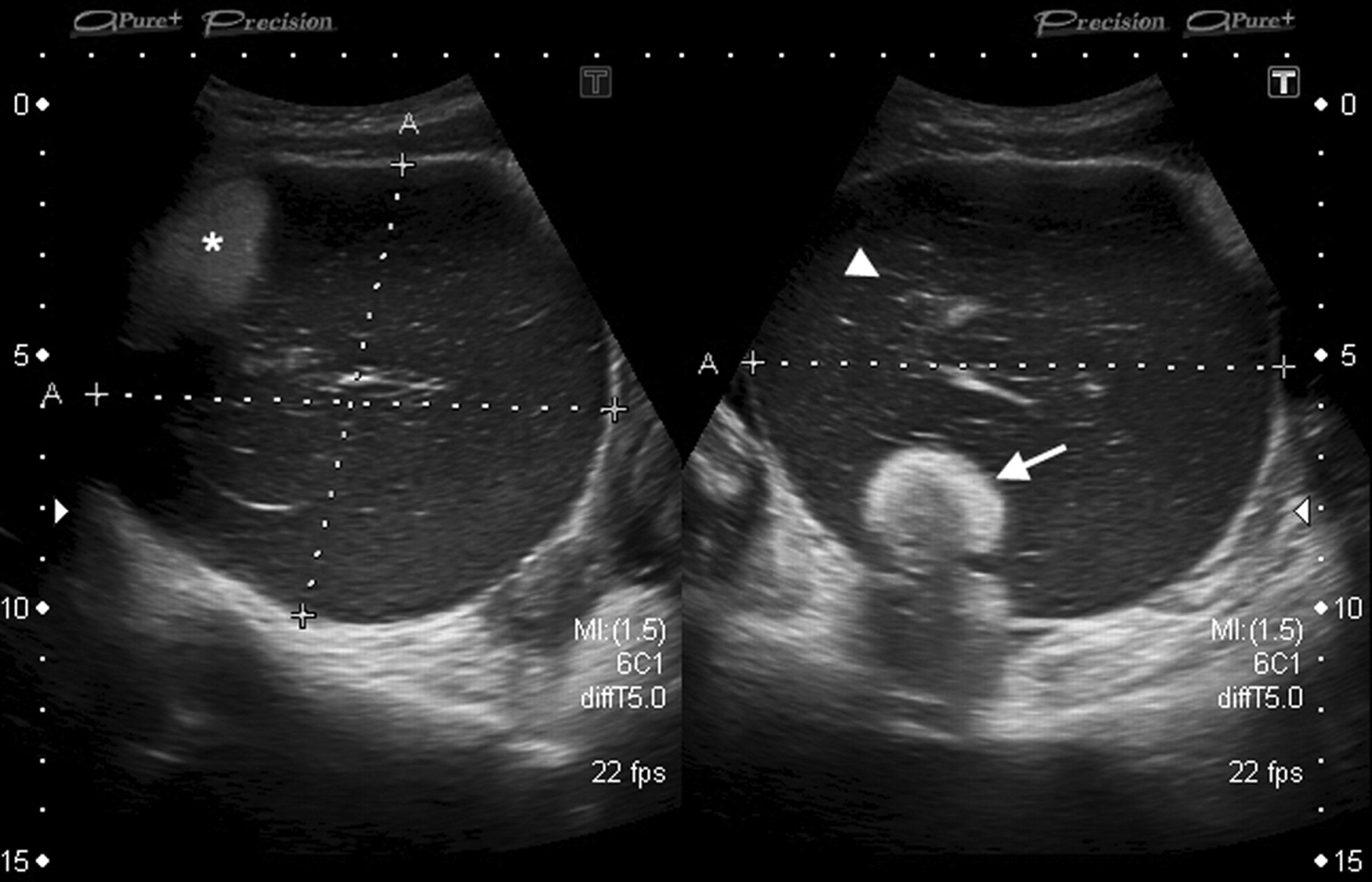
Intracystic floating balls
Numerous intracystic hyperechoic floating balls are an uncommon finding but are thought to be pathognomonic for mature teratoma. The size of the balls is variable. The balls are thought to form due to aggregation of sebaceous materials around a focus of debris, squamous material or fine hair. The balls often float within the mass (Figure 7). When assessing this feature, advantage should be taken of the dynamic nature of the US investigation, as the balls may be shown to move with changes in patient position. These features and the absence of blood flow within the balls will usually allow differentiation from solid mural nodules. 11

Intracystic floating balls. Uncommon but pathognomonic sign. Multiple hyperechoic balls float within the cyst cavity: (a) ultrasound and (b) computed tomography
Fat–fluid or fluid–fluid levels
As an isolated feature (ie in the absence of other characteristic signs), fat–fluid or fluid–fluid levels cannot be used to reliably distinguish dermoid cysts from other adnexal pathologies 6 but when other signs suggestive of a dermoid are present, the presence of a fat–fluid level may be seen as a separate but less powerful discriminator. A floating mass of hair can sometimes be seen at the interface 8 (Figure 4d). The commonest orientation is for anechoic sebum to float atop a more hyperechoic aqueous/debris-containing layer, but less frequently, the anechoic layer may be dependent with a hyperechoic supernatant. 12,13
Table 1 is a suggested guide to the degree of confidence which can be ascribed to particular features.
Degree of confidence ascribed to particular features in making a sonographic diagnosis
In many cases multiple features are seen in combination. Figures 8 and 9 demonstrate typical examples, demonstrating dermoid mesh, shadowing echodensity and linear interface (Figure 8) and regional high echogenicity, dermoid mesh and shadowing Rokitansky nodule (Figure 9).
Multiple features: dermoid mesh, shadowing echodensity and linear interface
Multiple features: regional high echogenicity, dermoid mesh and shadowing Rokitansky nodule
Pitfalls
Atypical dermoid cysts
Dermoid cysts may rarely appear as purely cystic (anechoic) masses, this finding being more common in adolescence, which can be a cause of diagnostic difficulty. 14 A search for hyperechoic foci will often be fruitful but there will be a few that still demonstrate purely cystic features (see Figure 10).
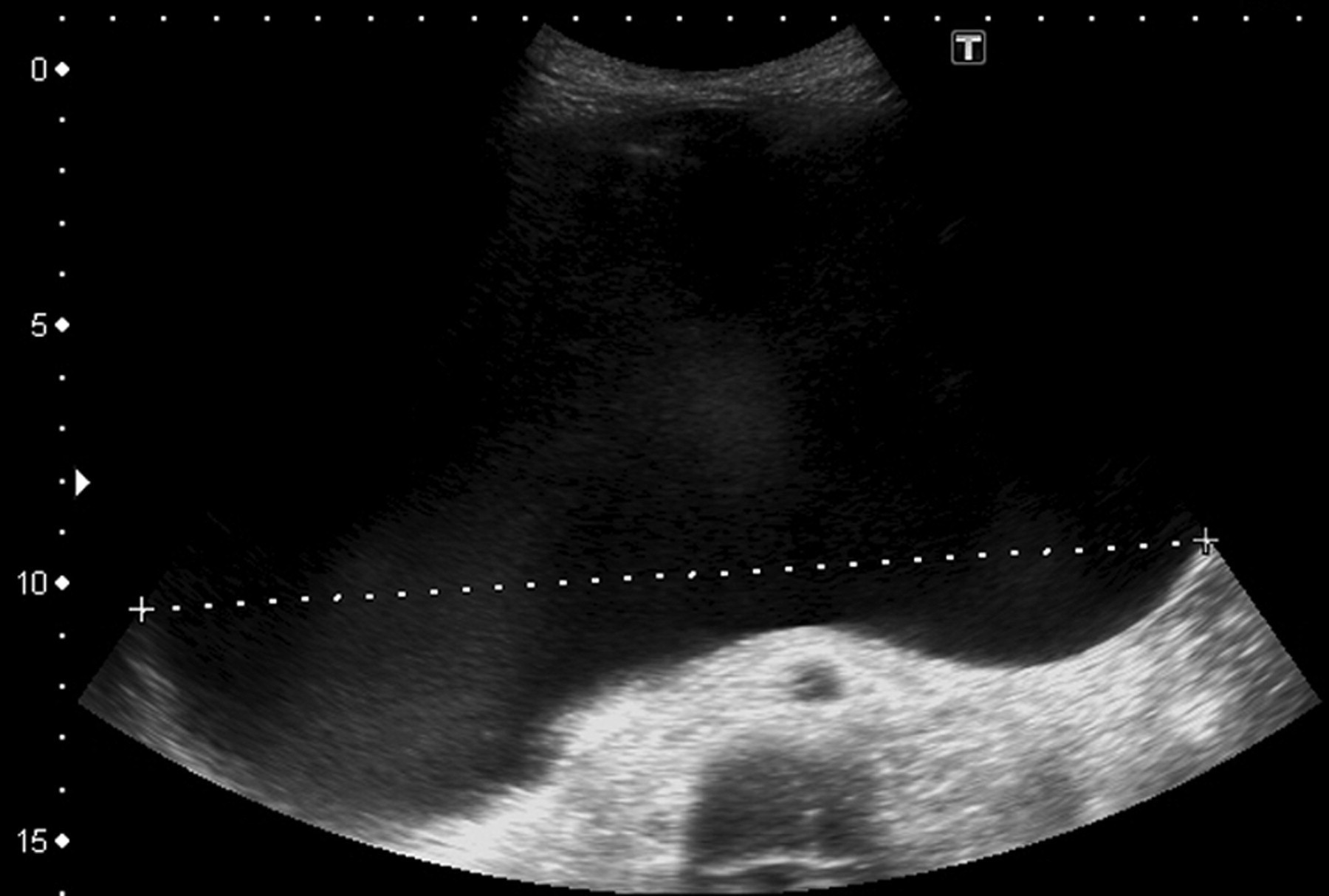
Pathologically proven example of dermoid cyst in a 15-year-old girl, this dermoid exhibited purely cystic features
A small proportion of dermoid cysts may exhibit multiple locules, thick and thin septa, and solid appearing components, mimicking ovarian malignancy (Figures 11 and 12). In this situation it can be difficult if not impossible to distinguish the atypical dermoid from a borderline of frankly malignant cystic ovarian tumour with US, and further investigation, for example with pelvic MR imaging (MRI), and serologic markers such as CA125, are recommended.

Thickened septations within a multiloculated mass. Computed tomography and magnetic resonance demonstrated the presence of fat, and histology confirmed an infarcted dermoid cyst which had evidence of capsular rupture

Hyperechoic mural nodularity. Borderline tumour was suspected but magnetic resonance imaging demonstrated the cystic component to be fatty sebum and the mural nodule to be a Rokitansky nodule. This was confirmed to be a dermoid cyst at histology
Mimics of dermoid cysts
Haemorrhagic cysts may be seen as hyperechoic masses, but these usually demonstrate increased through-transmission compared with the posterior acoustic attenuation seen in association with dermoid cyst, 8 and haemorrhage often shows additional distinguishing features such as fibrinous strands or retracting clot. 6
Endometriomata may mimic dermoid cyst due to the presence of desiccated blood products and nodules of fibrosis; shadowing hyperechoic foci may be seen.
Bowel gas may be mistaken for a hyperechoic dermoid cyst or vice versa. A mass may be missed with the limited field of view using a transvaginal approach, and a transabdominal examination is especially important when a pelvic mass is palpated but not seen on transvaginal ultrasound.
Tubo-ovarian abscesses may contain shadowing hyperechoic areas due to the presence of gas, fluid–fluid levels due to the presence of pus and hyperechoic areas due to haemorrhage but the clinical context (usually an unwell patient, often with signs of sepsis and pain) will be helpful in making this diagnosis. Figure 13 demonstrates such an example.
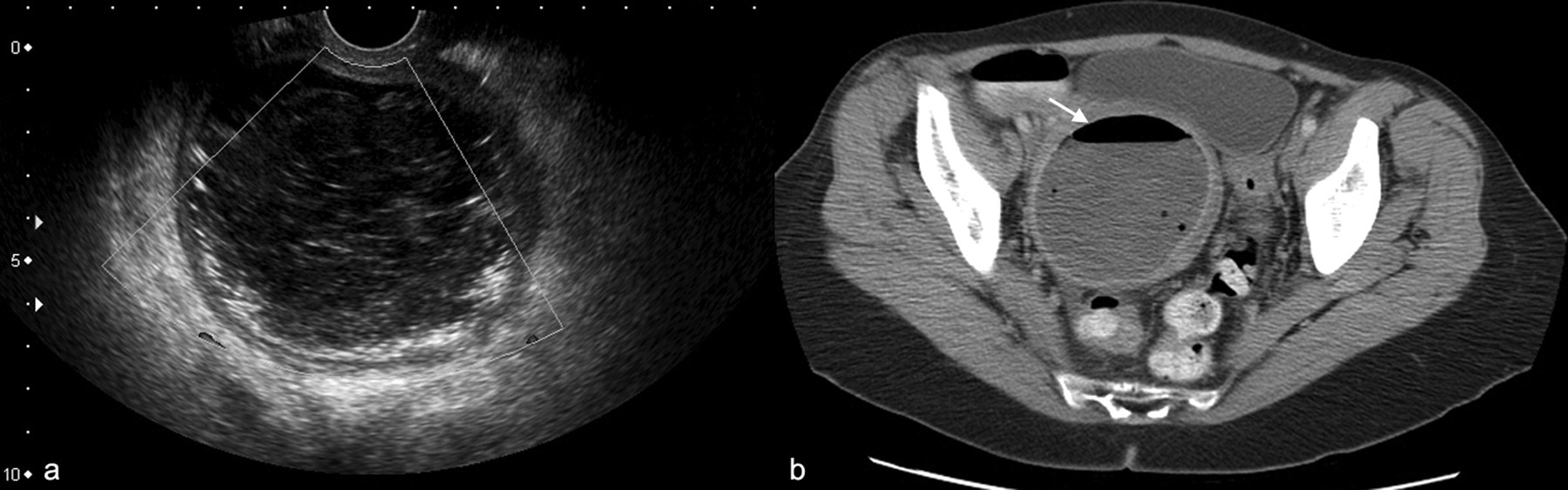
Ultrasound (a) demonstrates mass with multiple linear high reflectivity echoes. This could be misinterpreted as dermoid mesh but the patient was unwell and computed tomography (b) confirmed the presence of gas within this pelvic abscess
Pedunculated fibroids may result in a shadowing mass with calcification.
Ectopic pregnancy, perforated appendix with appendicolith, and solid ovarian masses, particularly those with a fibrous component such as cystadenofibromas are further examples of pathologies whose features may occasionally mimic those of a dermoid cyst and all have been described as causes of false-positive diagnoses. Figure 14 demonstrates a mass which contains regional high echogenicity. Dermoid cyst was within the differential but at histology this was a granulosa cell tumour.
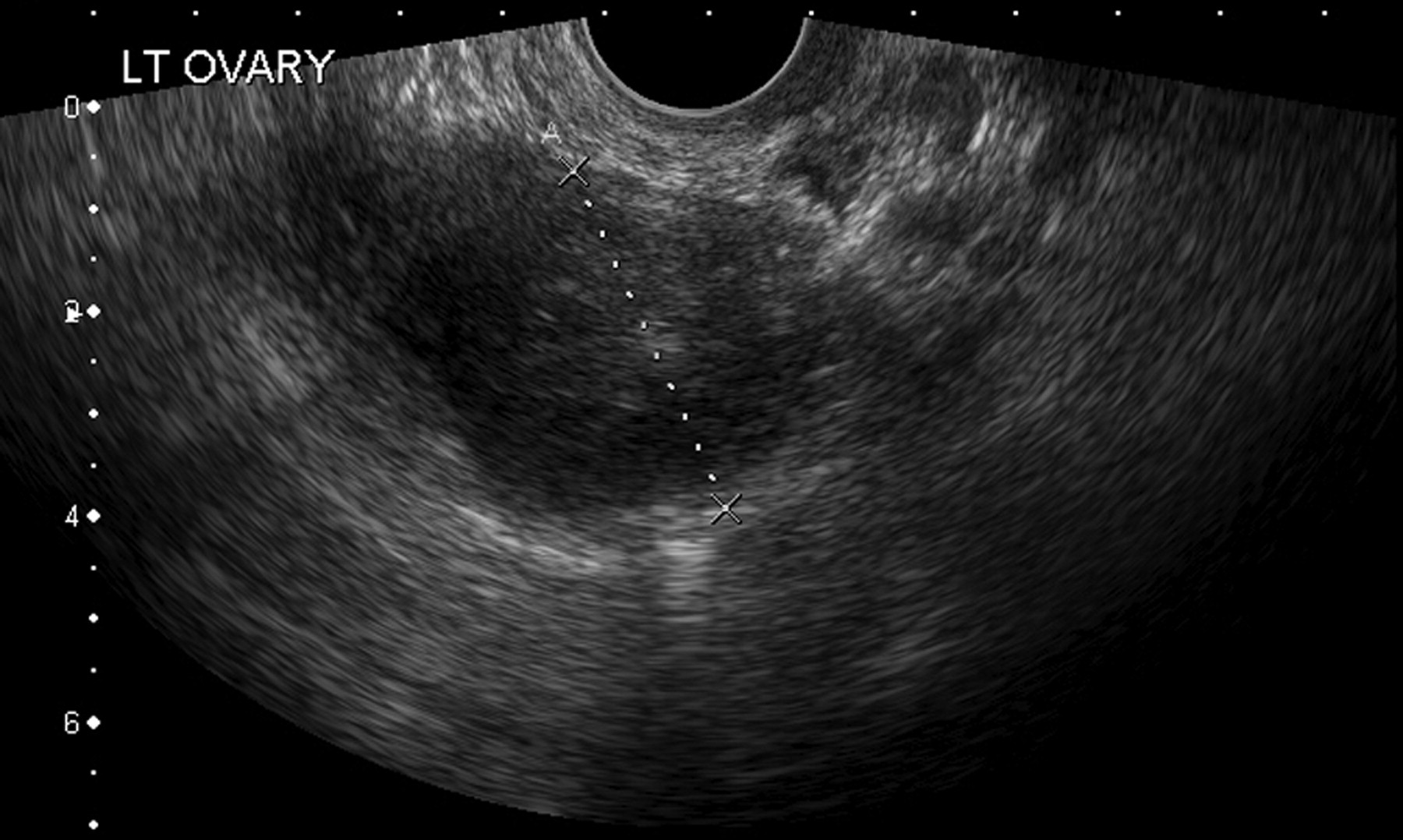
Mass containing areas of increased echogenicity. Histology: granulosa cell tumour
Conclusion
Accurate characterization of adnexal masses is vital for guiding appropriate patient management and surgical planning. In particular, distinguishing between benign and malignant masses helps to determine the type of and extent of surgery as well as where surgery is performed and by whom.
While the appearance of dermoids can mimic other pathologies and the sensitivity and specificity of US for diagnosing dermoid cysts is less than that of MRI or computed tomography (CT), certain sonographic features are considered classical for a dermoid. We have outlined these characteristic features. More than one feature is often present and a thorough examination to detect additional features allows a high positive predictive value to be achieved with US alone.
CT and MRI are more sensitive and specific for the presence of fat within a mass, and these modalities, particularly MRI, may be helpful where further characterization of a mass is required, but they are expensive and time consuming, factors which must be considered given the present financial climate and limited resources. Malignancy is rare in these tumours and there are few signs with other modalities that will accurately predict or exclude malignancy. MRI should be limited to the evaluation of patients where the US findings are equivocal or the presentation unusual. CT should be reserved for patients where there are other features to suggest malignancy, when it serves as the optimum staging modality.
In summary, in the right clinical context and in the presence of two or more characteristic features, US is a reliable tool for the diagnosis of mature cystic teratoma, and most dermoid cysts can be diagnosed with US.
DECLARATIONS
The authors have no conflicts of interest to declare.