
Abstract
Many patients presenting with haematuria undergo intravenous urography, renal tract ultrasound and cystoscopy. Renal tract ultrasound includes imaging of the bladder, which can significantly increase scan times by necessitating bladder filling, which can impact negatively on appointment scheduling. Little published literature exists on whether ultrasound of the bladder in the presence of haematuria is of any clinical benefit. This study aims to redress this by comparing bladder ultrasound to the gold standard of cystoscopy and also by assessing temporal implications in this patient group. A prospective study was undertaken where 96 consecutive urology-referred patients had their bladder ultrasound findings compared with the findings of cystoscopy under the headings of mass, trabeculation, diverticulum, stone and fistula. Ultrasound had poor sensitivity (47.8%), but good specificity (94.5%) in detecting the predefined bladder pathologies with a poor Kappa score of 0.33 when compared with cystoscopy. In addition, there was a significant time burden placed on the list by including bladder scanning as part of the renal tract sonographic assessment. In conclusion, bladder ultrasound is not shown to be a clinically useful adjunct to cystoscopy for the detection of bladder pathology. We would recommend that, in the setting of haematuria, ultrasound be used only for upper tract assessment.
As in many other centres, our current protocol is to examine with ultrasound the full urinary bladder in all patients presenting with haematuria despite cystoscopy being recognized as the superior imaging technique. We investigated this practice to determine its efficacy and to identify whether changes were required. It was anticipated that our findings may help to endorse current procedure or lead to recommendations which could result in service improvement.
Our hypothesis was that bladder ultrasound performed during the routine investigation of haematuria does not afford significant clinical benefit, and may extend unnecessarily examination times. Our aims were to compare the diagnostic outcomes of bladder ultrasound to flexible cystoscopy and to evaluate the temporal cost associated with bladder ultrasound. Locally urology protocol varies for macroscopic and microscopic haematuria and for patients under and over the age of 40. Although it is appreciated that nationally many patients presenting with haematuria may have computed tomography intravenous urography (CTIVU), this is not performed routinely at our centre.
While including the bladder during a renal ultrasound examination does not result in any significant burden of mortality or morbidity, other factors and potential complications still need consideration. The patient is asked to drink one pint of water prior to their appointment to allow ultrasonic visualization, which may be problematic in certain patient demographic groups such as the elderly. Fluid loading in a patient cohort often on diuretic therapy is questionable. Furthermore, many patients may find it uncomfortable to attend and wait with a distended urinary bladder.
Certain variables are involved in attaining adequate bladder filling for optimum imaging, including body mass, hydration status, temperature and timing of consumption. As a result many patients attend with inadequately filled bladders. These patients are therefore required to drink more fluid after their initial scan prior to being reimaged (sometimes on more than one occasion), which lengthens not only their own stay in the department and cumulative imaging time, but also encroaches on subsequent patient appointment times. In order to accommodate these unpredictable but frequent delays, longer time periods have to be used for each individual patient attendance which has the effect of reducing overall capacity. Therefore, including ultrasound imaging of the bladder as part of the routine assessment of the renal tract in the investigation of haematuria can be a source of discontent to patients and those performing the examination, as well as impacting on waiting lists. Limited published literature exists on comparison between imaging techniques in the investigation of haematuria, and on whether or not to include the bladder as part of renal tract assessment.1–5 This study aims to address whether, in the setting of haematuria, routine investigation of the bladder by ultrasound is indeed necessary, when a patient also undergoes cystoscopy.
Materials and Methods
This prospective study was carried out over a three-month period at Leigh Infirmary which is part of the Wrightington, Wigan and Leigh NHS Foundation Trust. Ethical approval was obtained from the local hospital ethics committee.
An initial pilot study was performed to determine the percentage of patients referred for haematuria investigation who subsequently had cystoscopy, in keeping with our centre's investigation policy. This occurred in over 95% of cases, demonstrating that nearly all patients referred for haematuria go on to have cystoscopy.
A literature review was performed to determine whether any bladder pathologies may exist which would be identifiable only by ultrasound and not cystoscopy, thus making the exclusion of bladder ultrasound unacceptable. None was found. In addition, a set of bladder pathologies was identified which would be detectable by both bladder ultrasound and cystoscopy enabling direct comparison of the two techniques.
Cystoscopy was used as the recognized gold standard technique for identification of bladder pathology, and it is against this that the ultrasound sensitivity and specificity were to be measured. These abnormalities were bladder mass, 6 bladder calculus, 7 bladder diverticulum,8,9 bladder wall trabeculation 10 and bladder fistula.11,12 A limitation of cystoscopy is that it cannot assess bladder volume. However, it can identify urethral abnormalities and bladder wall inflammation. An advantage of ultrasound is that it has the ability to detect incidental pelvic pathology.
The urinary tract ultrasound assessments within the study were performed with no deviation from departmental protocol, which involves ultrasound of both kidneys and bladder of patients with haematuria referred from the urology department. If a cystoscopy had been performed in advance of the scan the sonographer was blinded to the report and was therefore unaware of any predetected pathology. All ultrasound examinations were performed by one of three experienced sonographers each with at least 10 years’ experience. Patients were instructed to drink one pint of water prior to scanning and to refrain from micturition in an attempt to achieve a distended bladder. 13 Drinks other than water were not recommended since they may contain caffeine which has a diuretic effect. Patients were scanned using either a Phillips HDI ultrasound machine (Philips Medical Solutions, Crawley, UK) using a 2–5 MHz curvilinear transducer, or a GE Logiq 5000 ultrasound machine (GE Medical, Wauwatosa, WI, USA) with 3–5 MHz curvilinear transducer. The ultrasound examinations were reported immediately post completion by the sonographer performing the scan.
Any trabeculation and bladder wall thickening were measured on the posterior bladder wall. 11 Residual post micturition volume was calculated using the height, depth and width of the bladder. 14 Any suspected bladder stones were differentiated from calcified bladder tumours by altering patient posture 15 as were debris and clots. In addition, note was made of masses, diverticula, fistulae and enlarged prostate glands. Space was included on the data collection sheet for other pathologies not listed above. The time taken for each ultrasound examination was recorded, including time taken to allow the patient to fill their bladder while waiting for an additional scan.
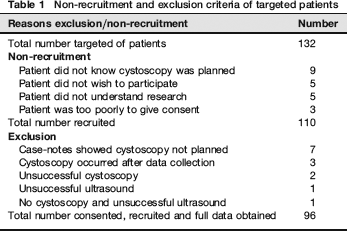
Patients considered eligible for inclusion into the study were those patients with microscopic or frank haematuria who were referred to the urology department either by their general practitioner or via the accident and emergency department. Patients were excluded from analysis if they did not have cystoscopy or ultrasound assessment of the bladder. Table 1 shows non-recruitment and inclusion/exclusion criteria of targeted patients.
Non-recruitment and exclusion criteria of targeted patients
All cystoscopies were performed by either a consultant urologist or a urology specialist nurse using an Olympus Video cystoscope (Olympus KeyMed Group, Southendon-Sea, UK). Cystoscopy was performed, as per protocol, using local anaesthesia by way of topical gel, with preprocedural ciprofloxacin antibiotic cover. Patients were eligible for cystoscopy if they presented with either microscopic or frank haematuria. Exclusion criteria for cystoscopy were either a patient unable to give appropriate consent, consent refusal or patients not medically fit for the examination.
Following the pilot study, a cohort of 105 patients was sought giving a confidence limit of 90% and confidence interval of 8%. Cohen's Kappa inferential statistical test was used to measure concordance of dichotomous data and represents the chance corrected proportional agreement between bladder ultrasound and flexible cystoscopy using cystoscopy as verification of pathology. A kappa result of k = 0 indicates no agreement, k > 0.41–0.6 indicates moderately good agreement, k > 0.61–0.8 indicates substantial agreement and k > 0.81–1 indicates almost perfect agreement. 16
Results
Over the three-month study period, 132 recruitment letters were sent out and 110 patients participated. Table 1 shows the data were incomplete on 14 investigations, so the final number was 96. Of these, 57 (59%) were men and 39 (41%) were women. The age range was 16–87 years with a mean age of 58. This gives the study results a confidence limit of 90% with a confidence interval of 8%.
Bladder ultrasound efficacy
Table 2 shows bladder pathologies detected by both cystoscopy and ultrasound, with a total of 28 identified pathologies in 23 patients on cystoscopy, and a total of 18 pathologies in 15 patients on ultrasound. Not all pathologies were detected by both tests.
Pathology detected on cystoscopy and ultrasound
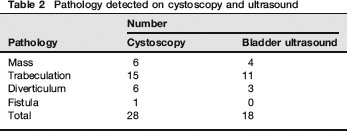
Table 3 shows the sensitivity of ultrasound to detect bladder pathology when compared with recognized gold standard cystoscopy is 47.8% while its specificity is 94.5%.
Ultrasound sensitivity and specificity
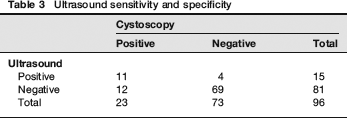
The kappa value was calculated at 0.32 with a 95% confidence interval of 0.1102–0.5232 indicating only a poor to fair agreement between cystoscopy and bladder ultrasound. Ultrasound was shown to have a sensitivity of 47.8% and a specificity of 94.5% for detecting bladder pathology. Correlation of ultrasound and cystoscopy sensitivity and specificity with regard to pathologies is shown in Tables 3 and 4.
Correlation of ultrasound and cystoscopy

Ultrasound performance time
The total time to perform a scan of both kidneys on the 96 patients was 471 minutes (7 hours 51 minutes), with a mean time of four minutes 54 seconds. There were only four (0.4%) lengthy kidney scans in patients with renal pathology, which took over 10 minutes to perform.
The total time taken to perform bladder scans, including time allowed for optimal bladder filling, on the 96 patients was 1096 minutes (18 hours 16 minutes), with a mean time of 11 minutes 25 seconds per bladder scan. There were a total of 34 (35%) lengthy bladder scans; 12 took over seven minutes, six took over 10 minutes and 16 took over 20 minutes to perform.
Figure 1 shows the times taken to scan bladder and kidneys of patients. The middle quartiles for a kidney scan were from four to six minutes, while the median time was four minutes. The middle quartiles for a bladder scan were from five to 10 minutes, while the median time was six minutes. The shortest time to scan kidneys was one minute and the longest 15 minutes, while the shortest time to scan a bladder was two minutes and the longest 61 minutes.
Box Whisker plot of scan times for bladder and kidneys
Cystoscopy performance time
The specific time taken to perform each cystoscopy was not documented nor was individual patient experience of the procedure, as this was not the aim of the research since it did not impact on the ultrasound department. However, the average time taken to perform a cystoscopy was about five minutes, with five minutes preparation time. The procedure is well tolerated, though patients can vary in their pain threshold and hence experience is variable. Often after the procedure patients have discomfort for a few voids, but this usually settles within 24 hours.
Discussion
The study hypothesis is that bladder ultrasound, which is performed during the routine investigation of haematuria at this centre, does not afford any significant clinical benefit, while extending significantly examination times. One study aim was to compare the diagnostic outcomes of bladder ultrasound in the setting of patients who also have flexible cystoscopy as part of their diagnostic work-up.
Locally all patients over 40 years of age experiencing macroscopic or microscopic haematuria routinely have renal tract ultrasound, intravenous urography (IVU) and cystoscopy. Patients under 40 years of age with macroscopic haematuria have renal tract ultrasound, IVU and cystoscopy, while those presenting with microscopic haematuria have renal tract ultrasound and cystoscopy only.
Although this is a single centre study and involves small numbers, we have demonstrated that the sensitivity of bladder ultrasound in detecting bladder pathology was poor while its specificity was moderately good. Our study indicates that routine bladder ultrasound, when compared with cystoscopy, may be an unsatisfactory modality for detecting certain specific bladder pathologies. 17 However, a larger study is required for corroboration of our findings.
Bladder mass: The sensitivity of ultrasound was only 66.6%, meaning that there would be a miss rate of 8.2 per 100,000 population in men and 3.2 per 100,000 population in women were ultrasound to be used alone. 18
Trabeculation: Ultrasound reported 11 cases of trabeculation compared with the 15 found during cystoscopy, but of more significance was the fact that only 33% of the cases reported by ultrasound were in fact true positives and 66% were false-negatives.
It has been suggested that a cause for this is that bladder under-filling creates a trabeculated appearance and hence misdiagnosis. 19
Diverticula: Of the six cases identified by cystoscopy, only three were found on ultrasound with a further three falsepositives identified.
Fistulae: Only one fistula was found during cystoscopy but it was missed by ultrasound as was the associated bladder mass, which may be due to the fact that it was situated at the dome of the bladder and again under-filling may have an effect on identification of pathology in this region.
The above comparison of pathology detected by the two investigations highlights ultrasound's limitations in this field with its poor sensitivity (47.8%) and moderate specificity (94.5%) compared with cystoscopy.
Table 1 shows non-recruitment criteria. Seven patients did not have cystoscopy. This was because of frailty due to old age or co-morbidities, learning difficulties and in one case the patient declined cystoscopy and was offered computed tomography instead. None of these cases affected whether a patient went on to have renal ultrasound as this was standard protocol and was accepted by all patients with haematuria.
The second aim of this study was to look at the temporal cost associated with bladder ultrasound. Analysis of the time required to perform bladder ultrasound at an attendance for assessment of the renal tracts shows that 96 patients required an extra 1096 minutes (1587 minutes in total) to have their scan compared with 491 minutes solely for upper tract scanning. This equates on average to an increase in time from just over five minutes to 16.5 minutes per patient. At present a patient is allocated a 20-minute attendance slot which equates to 12 patients per four hour session. If bladder ultrasound was to be discontinued then imaging slots could be halved leading to a 100% increase in the number of patients who could be scanned per session.
It is also of note that only 0.4% of upper tract scans exceeded 10 minutes whereas when bladder scanning is included, 35% took over 10 minutes and 16% took over 20 minutes. These figures indicate that there would be approximately two patients per 12 patient list whose scan time would encroach on other scan slots, which may create a negative attendance atmosphere for both the patient who is being kept longer to bladder fill and the other attendees being delayed. Although patient experience was not specifically assessed in this research, there is the added disadvantage of known anecdotal patient discomfort associated with waiting with a full bladder for bladder ultrasound.
There are areas where ultrasound scanning of the bladder is of obvious importance, as in the assessment of post micturition volumes in patients with recurrent urinary tract infections and lower urinary tract signs.20,21 It is appreciated that, in patients with neurogenic bladder, ultrasound may be beneficial in measuring bladder volume and wall thickness. 22 Research suggests that colour Doppler analysis of ureteral jets can enable detection and determination of the degree of ureteral obstruction in many patients with unilateral ureteral calculi. 23 Also, patients with chemotherapyinduced haematuria may benefit from bladder ultrasound to confirm wall thickening or the presence of a blood clot in the bladder, which may mean cystoscopy could be avoided. 24 All these areas of bladder ultrasound are quite specific and not relevant to this study of the routine investigation of haematuria.
CTIVU images the kidneys, ureters and bladder using a contrast medium similar to that used during IVU, but is a superior modality when suboptimal images of the renal tract by normal IVU or ultrasound are obtained due to either patient obesity or overlying bowel gas. CTIVU may also resolve small calculi not seen by alternative imaging and show distant tumour spread, but the radiation dose to the patient is higher than IVU. Some institutions are performing CTIVU routinely and have ceased doing IVUs. However, at our centre CTIVU is not performed routinely on patients presenting with haematuria.
Recent work has attempted to streamline the diagnostic pathway for haematuria assessment, as well as comparing the diagnostic efficacy of associated imaging techniques. 25 However, the paucity of relevant literature has made this difficult to achieve accurately.4,5,25–27 Within the confines of this small local study, there is little evidence to suggest that ultrasound bladder volume assessment and measurement in the setting of routine investigation of haematuria is of any benefit in urology referred patients who are to have cystoscopy. Conversely, our findings suggest that bladder ultrasound causes measurable negative impacts on scheduling and patient attendance for renal tract imaging. On the basis of this study we recommend removing ultrasound imaging of the bladder from the routine assessment of patients referred with haematuria who are to have cystoscopy as part of their investigation.
Declarations
The authors have no conflicts of interest to declare.