
Abstract
We present a case of a 13-year-old boy who presented with a three-day history of left lower extremity swelling and a deep venous thrombosis. On further work-up he was discovered to have a large aneurysm of the inferior vena cava. After extensive discussion with his family, he underwent resection and primary repair of the inferior vena cava without complication. At a six-month follow up appointment, he was doing well with no recurrent aneurysmal degeneration on computed tomography scan imaging.
Keywords
Introduction
We present a case of a 13-year-old boy who presented with a three-day history of left lower extremity swelling and a deep venous thrombosis (DVT). On further work-up, he was discovered to have a large aneurysm of the inferior vena cava (IVC). After extensive discussion with his family, he underwent resection and primary repair of the IVC without complication. At a six-month follow-up appointment, the patient was doing well with no recurrent aneurysmal degeneration on computed tomography (CT) scan imaging.
Case report
A previously healthy 13-year-old male was admitted to our institution in July of 2009. His chief complaint on presentation to his pediatrician's clinic was left lower extremity swelling and pain that began without any recent history of trauma to the leg. The pain began three days prior to presenting to the pediatrician's office and was relieved with Naproxen. The patient had no significant past medical or surgical history, including a prior history of DVT, as well as no family history of DVT or clotting disorders. Initial investigation included a venous duplex study of the left leg, which revealed an extensive DVT that included the distal external iliac, common femoral, femoral, popliteal, posterior tibial, peroneal and gastrocnemius veins of the left lower extremity. The finding of a DVT in a healthy 13-year-old boy was unexpected, so his pediatrician admitted him to the hospital and a CT scan of the abdomen and pelvis with contrast was performed. The CT scan revealed a 3.9 × 4.4 × 6.1 cm well-defined, enhancing mass in the right retroperitoneum that traversed along the course of the IVC at the level of L2–L3, suggestive of a venous malformation (Figure 1). It was discussed whether this was a retroperitoneal mass such as an angiosarcoma or a vascular malformation. An abdominal ultrasound suggested that the mass was an aneurysm of the IVC. At this time, the right lower extremity was asymptomatic so it was not evaluated with duplex ultrasonography during this admission.
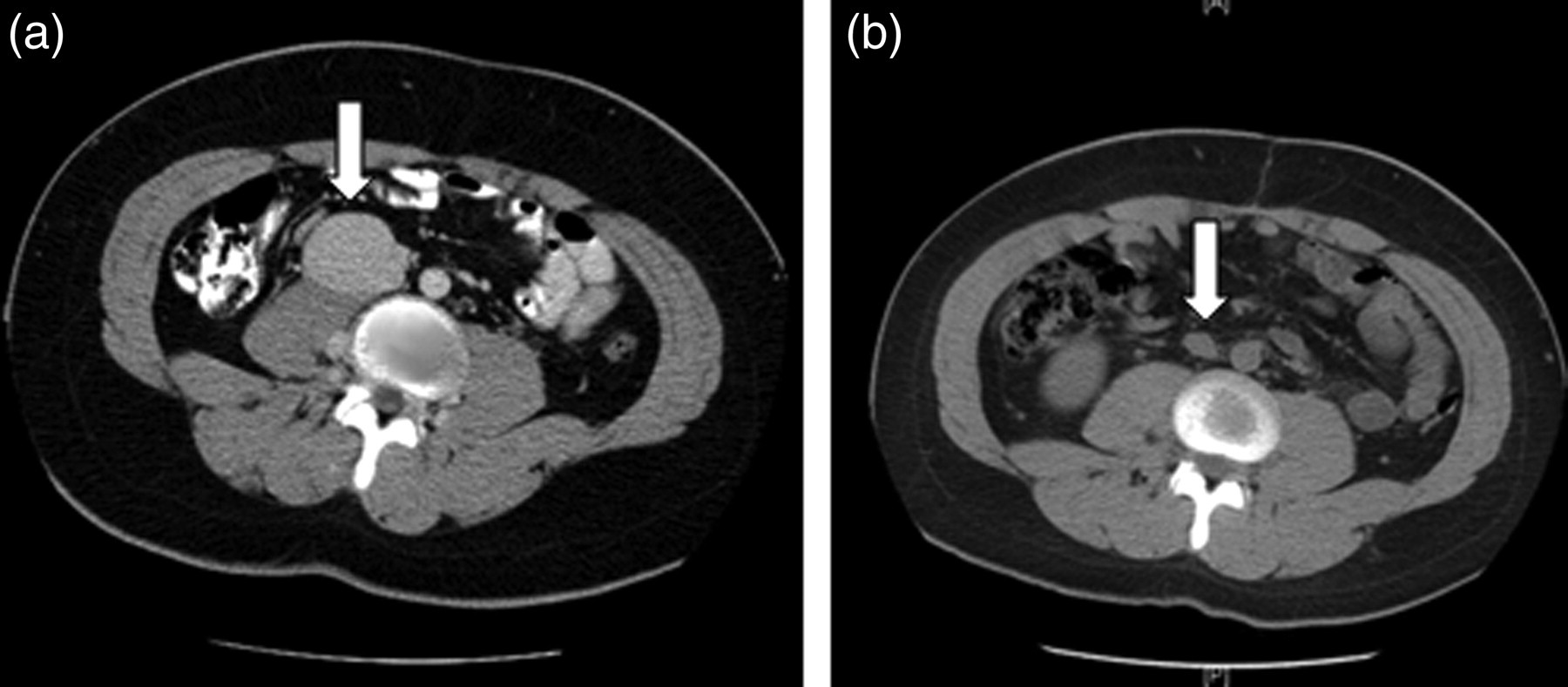
Images on computed tomography (CT) scans. (a) Preoperative CT scan showing the inferior vena cava (IVC) aneurysm. (b) Postoperative CT scan with a normal caliber IVC after resection and primary repair
During his stay at our institution, pediatric hematology/oncology was consulted and recommended a full hypercoagulable work-up be performed to include: baseline complete blood count, prothrombin time/partial thromboplastin time, factor V Leiden, prothrombin gene mutation, protein C and S activity, antithrombin III, lupus anticoagulant, antiphospholipid antibiotics, anticardiolipin antibodies and beta2-glycoprotein antibodies. The entire hypercoagulable workup was negative. At this point, the vascular surgery service became involved and it was decided that he had a saccular, infrarenal IVC aneurysm. For treatment of the DVT, he was placed on full anticoagulation and discharged home on Coumadin. Despite the suggestion of the vascular surgery service to proceed with thrombolytic therapy for his left leg DVT to minimize the risk of developing postphlebitic syndrome, the family declined thrombolytic therapy.
Six weeks later, he returned for a venogram as an outpatient to further delineate the anatomy of this malformation and assess the caliber of the vena cava above the aneurysm (Figure 2). The cavogram showed a normal appearing IVC below the level of the renal veins. There was a large branch with aneurysmal degeneration. Just above the renal veins the vena cava had an atretic portion. Distally there was reconstitution through extensive collaterals. Proximally, the hepatic veins and the suprahepatic vena cava traveling to the right atrium showed normal caliber flow.

Venogram demonstrating inferior vena cava (IVC) aneurysm with a small IVC above the level of the aneurysm
Specific concerns arose when trying to decide on the proper course of treatment. It was discussed with the family that no treatment or simply observation would put the patient at risk for re-thrombosis, pulmonary embolus or possibly rupture. In addition, long-term Coumadin therapy was considered a poor option for an active 13-year-old boy. Due to the atretic portion of the vena cava and the likely possibility of eventual stent failure due to his young age, it was thought that a percutaneous approach would not be possible and an open surgical repair would be necessary. Treatment with an open resection and primary repair would be a major operation; however, this would offer the best option for definitive treatment and prevention of future complications. A literature search at this time yielded many options for repair with no consensus on any one particular approach.
In November 2009, the patient underwent definitive surgical treatment consisting of resection with primary repair of the entire IVC aneurysm (Figure 3). Postoperatively, with no evidence of immediate complications he was discharged home five days after surgery on Coumadin therapy with the plan to continue for six months after the initial diagnosis of DVT. Pathology from the surgical specimen was read as vessel wall with degenerative changes including myxoid degeneration and fragmentation of elastic fibers, with no evidence of malignant features. At an appointment six months after surgery, he was doing well and was without lower extremity pain, discomfort, swelling or difficulty with ambulation. To examine the repair, a follow-up CT scan was obtained which visualized the repair and demonstrated that there was no recurrent aneurysmal dilation of the IVC (Figure 1). On recommendation from the vascular surgeon, Coumadin therapy was replaced with an aspirin a day at this visit with resolution of his DVT on ultrasound evaluation and no evidence of DVT in either lower extremity at this time. The current plan is to continue the daily aspirin and return for follow-up imaging with a CT scan and bilateral lower extremity duplex ultrasound one year from now.
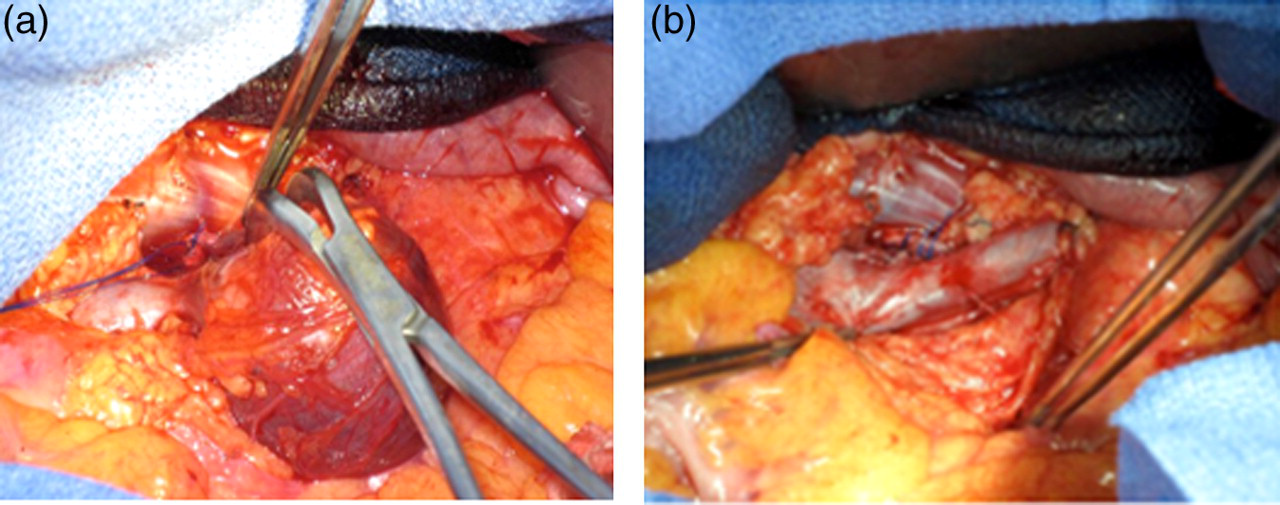
Intraoperative photographs during the aneurysm resection. (a) Shows the saccular aneurysm with a stalk connecting it to the inferior vena cava. (b) Shows the size of the aneurysm in the retroperitoneum prior to resection
Discussion
IVC aneurysms are a rare problem. The first case was reported by Oh et al. 1 in 1973. Since then there have been, to the best of our knowledge, 36 more cases of IVC aneurysms reported in the English literature (see Table 1). Of these cases, only nine have been in children 18 years of age or younger. 1–9 The youngest case reported was in a 2½‐year-old. Another case occurred in a five-year‐old. And finally, the remaining six were in children between the ages of 13 and 18.
Documented cases of IVC aneurysms
Abd. pain, abdominal pain; LE, lower extremity; f/u, follow-up; mo, month; NR, not recorded; PE, pulmonary embolism
Aneurysms of the IVC are true aneurysms, i.e. they involve all three layers of the wall of the vessel. They are classified as either saccular (more common) or fusiform in terms of shape. They are classified by location in a system developed by Gradman and Steinberg 10 in 1993. Type I IVC aneurysms are suprahepatic dilations of the IVC with no obstruction. Type II IVC aneurysms involve suprahepatic or intrahepatic interruption of the vena cava. Type III IVC aneurysms are located inferior to the renal vessels. Type IV is a miscellaneous group including aneurysms of the iliac vein with an associated left-sided vena cava. Finally, another classification based on possible etiology was developed by Thompson and Lindenauer. 11 Type I are congenital, Type II are acquired and Type III are secondary to an arteriovenous fistula.
The etiology of this dilation is a topic of much debate in the literature. Proposed mechanisms include congenital weakness in the wall of the vena cava; embryological malformations such as failure of regression of the embryological vessels or failure of fusion of one of the many anastomotic sites in the development of the adult IVC in utero; venous hypertension as from an outflow obstruction; trauma or other injury to the vessel; and association with surrounding inflammation.
Various presentations and associated complications have been reported in these 36 case reports of IVC aneurysms(see Table 1). For example, many have been associated with thrombosis – usually a DVT in the lower extremity or pelvis and/or abdominal or back pain as occurred in our case. Other patients presented with a pulmonary embolism, compression syndromes, Budd‐Chiari, pitting edema of the lower extremities, rupture, hemothorax, hematuria and associated cutaneous vascular malformations. In several of the case reports, it was stated that the aneurysm was originally thought to be a tumor or mass of the retroperitoneum. Interestingly, there have been no malignant changes seen on any of the pathology reports from these IVC aneurysms ever documented in the literature. Our case demonstrated this same finding.
The course of management or treatment of these aneurysms is just as controversial and undefined in the literature as the etiology. Many of the patients in the case reports were managed conservatively, either with observation consisting of serial imaging studies or observation and anticoagulation for associated thromboses. A number of patients were managed with surgical resection and either primary repair or interposition graft placement. More recently in the literature, a young child underwent coil embolization and vascular plugging of the aneurysm. 9 We were concerned about the durability of endovascular therapy in an adolescent who needed a lifelong solution. Finally, several cases underwent open exploration with or without biopsy. There are many issues to consider when deciding on the course of management to choose for the patient with an aneurysm of the IVC. Another treatment that has been proposed is endovascular stenting of the aneurysm; however, due to the low flow state of the vena cava, and especially if the patient is a child, there is a theoretical risk of thrombosis of the stent over time. 9
What should a young vascular surgeon take away from this case presentation? Ultimately, the most important question that arises is what is the appropriate course of management of a patient with an aneurysm of the IVC? The case reports reviewed had very limited follow-up, ranging from no documented follow-up at all to a maximum three-year follow-up in one adult case. Even less follow-up was reported for the pediatric cases, with 10 months as the maximum (see Table 1). Therefore, without long-term data it is impossible to know which course of management should be the standard of care. It is our opinion that each patient should thus be treated individually with certain factors taken into account. For example, patients who are poor operative candidates and who would likely not be able to tolerate a major operation, such as elderly patients or those with significant co-morbidities, should be considered for either a percutaneous option or observation with anticoagulation. A venogram should be performed to evaluate the anatomy when considering a percutaneous approach because, as with aortic aneurysms, it is not likely that all IVC aneurysms are amenable to an endovascular approach. In our case, we felt that because there is no long-term data on stent patency, placing a stent in a young boy posed the risk of stent thrombosis in the near or even distant future, which would require further intervention at that time. Also, placing a child on anticoagulation could lead to problems with involvement in sports and the overall activity level of a young male, placing him at unnecessary risk of major hemorrhage or injury. Overall, we believe that further research with long-term follow-up needs to be performed before any clear recommendations can be made in regard to the proper course of management for a patient who presents with an aneurysm of the IVC.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: none reported.