
Abstract
We report the endovascular treatment of two patients presenting with aortoduodenal fistulae. The first patient was a 66-year-old man admitted with hematemesis. He was on clopidogrel and had received a cryopreserved aortic graft for a mycotic abdominal aortic aneurysm five years earlier. Computed tomography (CT) showed aortic pseudoaneurysms in close contact with the duodenum. Endovascular repair was carried out. Twenty-seven months after the procedure the patient remains asymptomatic. The second patient was a 78-year-old man admitted with abdominal pain and nausea. CT revealed an abdominal aortic pseudoaneurysm and aortoduodenal fistula. He suffered from severe chronic obstructive pulmonary disease that greatly increased his surgical morbidity and mortality. An endovascular repair was performed under epidural anesthesia. The patient died of a postoperative pneumonia 38 days after surgery. These two cases illustrate the importance of endovascular aortic repair especially when an open surgical procedure is either difficult or impossible.
Keywords
Introduction
Aortoenteric fistula (AEF) is an abnormal communication between the aortic and intestinal lumens. It is an uncommon clinical condition that results in death if left untreated. AEFs can present in the native abdominal aorta (primary AEF), after endovascular aortic repair 1 or, more frequently, after aortic reconstructive surgery (secondary AEF). The incidence of primary AEFs according to autopsy studies varies from 0.04 to 0.07%, 2,3 while it rises to 1.6% in patients after abdominal aortic reconstruction. 4 Surgical repair consists of a thorough debridement of all the tissue surrounding the fistulous tract followed by either an extra-anatomical reconstruction and aortic ligation or in situ placement of a graft. Open repair is associated with high operative mortality (30–40%), an amputation rate of 9–10% and an aortic stump rupture of 10–50%. The long-term survival approximates 50% at three years. 5,6 Endovascular repair has emerged as an alternative treatment option for this devastating complication. Several case reports have described the successful treatment of AEFs with endovascular stent-grafting. 7–12 Here we present our experience with two patients, suffering from aortoduodenal fistula, without signs of sepsis, successfully treated with endovascular grafts.
Case report
Case 1
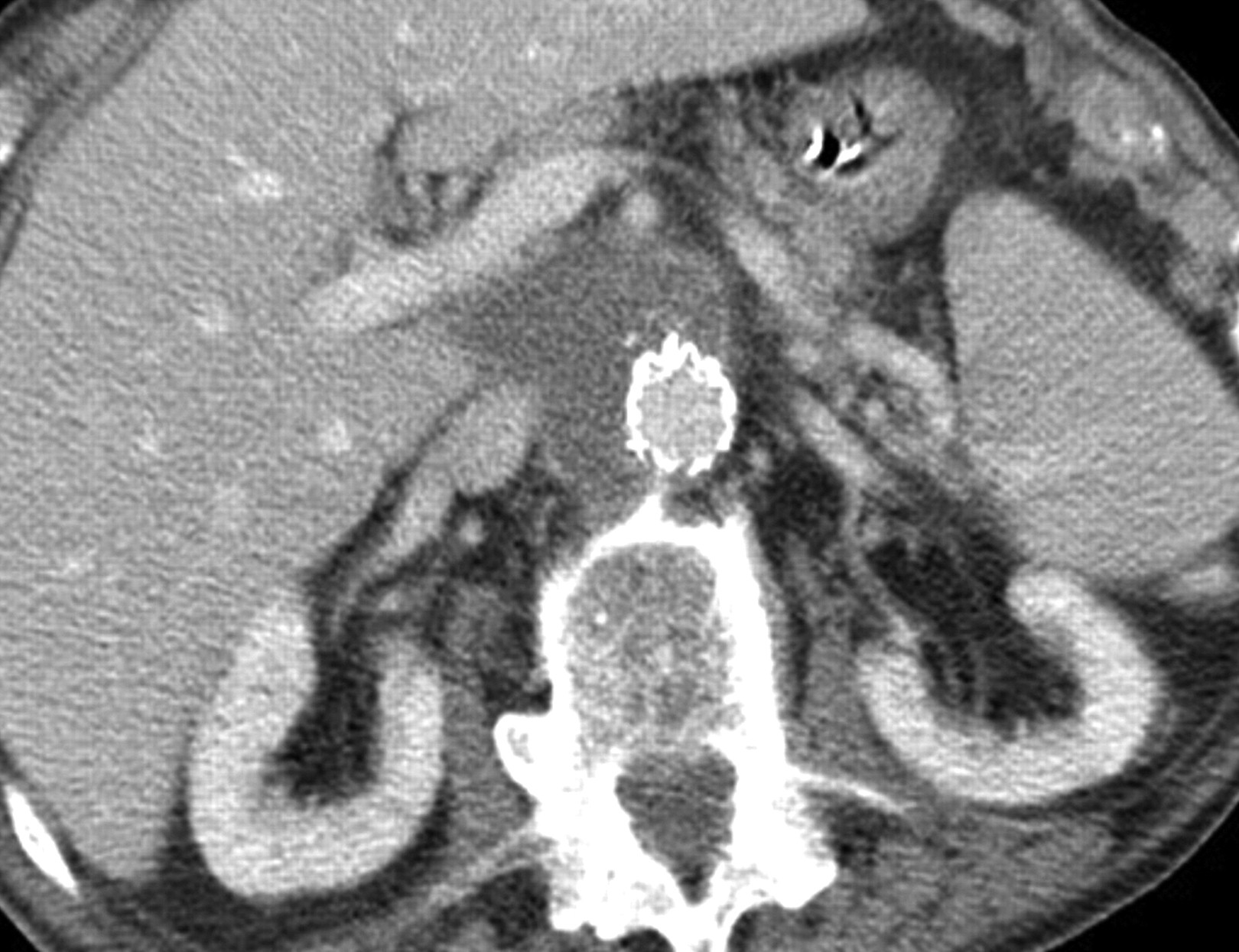
A 66-year-old man was admitted after an episode of hematemesis and syncope. He suffered from hypertension, diabetes, dyslipidemia and coronary heart disease. He had had a myocardial infarction eight years ago and several episodes of angina for which he had had several intracoronary stents placed, the last one, a drug eluting stent (everolimus) nine months before the event. He was on both acetylsalicylic acid and clopidogrel. Five years earlier, he had been treated at another center for a mycotic abdominal aortic aneurysm. He underwent aneurysm resection and interposition of a cryopreserved aortobiiliac bypass and a left iliac-femoral bypass with prosthesis. At the time of admission, his systolic blood pressure was 107 mmHg, heart rate was 59 bpm, body temperature was normal, white blood cell count was 8110/μL and hematocrit was 40.9%. Fresh blood was obtained after nasogastric tube placement. Hematocrit slowly dropped to 31.1%. Two upper gastrointestinal (GI) endoscopies failed to identify the source of the bleeding. Abdominal computed tomographic angiograms (CTA) showed several aortic pseudoaneurysms, two of them in close contact to the third and fourth portions of the duodenum. (Figures 1–3). These findings were suggestive of aortoduodenal fistula. Given the high morbidity and mortality associated with open surgery in this patient, endovascular treatment was chosen. The procedure was performed under general endotracheal anesthesia. Stent-graft placement of an infrarenal aortic device was performed, via bilateral femoral artery cutdowns under C-arm fluoroscopic guidance. An aorto-iliac right stent-graft (AUB2216C126) and occluder (OCL14) in the left iliac artery (Talent, Medtronic Inc, Minneapolis, MN, USA) were placed and a femoro-femoral bypass was performed. Postoperative imaging demonstrated satisfactory stent-graft position, complete exclusion of the pseudoaneurysms and no endoleak. Bleeding stopped immediately after stent-graft placement. Treatment of perforated duodenum consisted of nasogastric decompression, parenteral nutrition and antibiotics. On the ninth postoperative day, follow-up of computed tomography (CT) with oral contrast did not demonstrate any leak; oral intake was begun on the 15th day. The patient received intravenous broad-spectrum antibiotics perioperatively. No signs of sepsis or graft infection developed postoperatively and the blood cultures remained negative. The postoperative course was uneventful and the patient was discharged after 28 days, on oral ciprofloxacin for two weeks. After 27 months of follow-up, the patient is doing well, with no symptoms of bleeding or infection. Pseudoaneurysms are excluded, and no perigraft fluid, air or endoleak are evident on CTA (Figure 4).
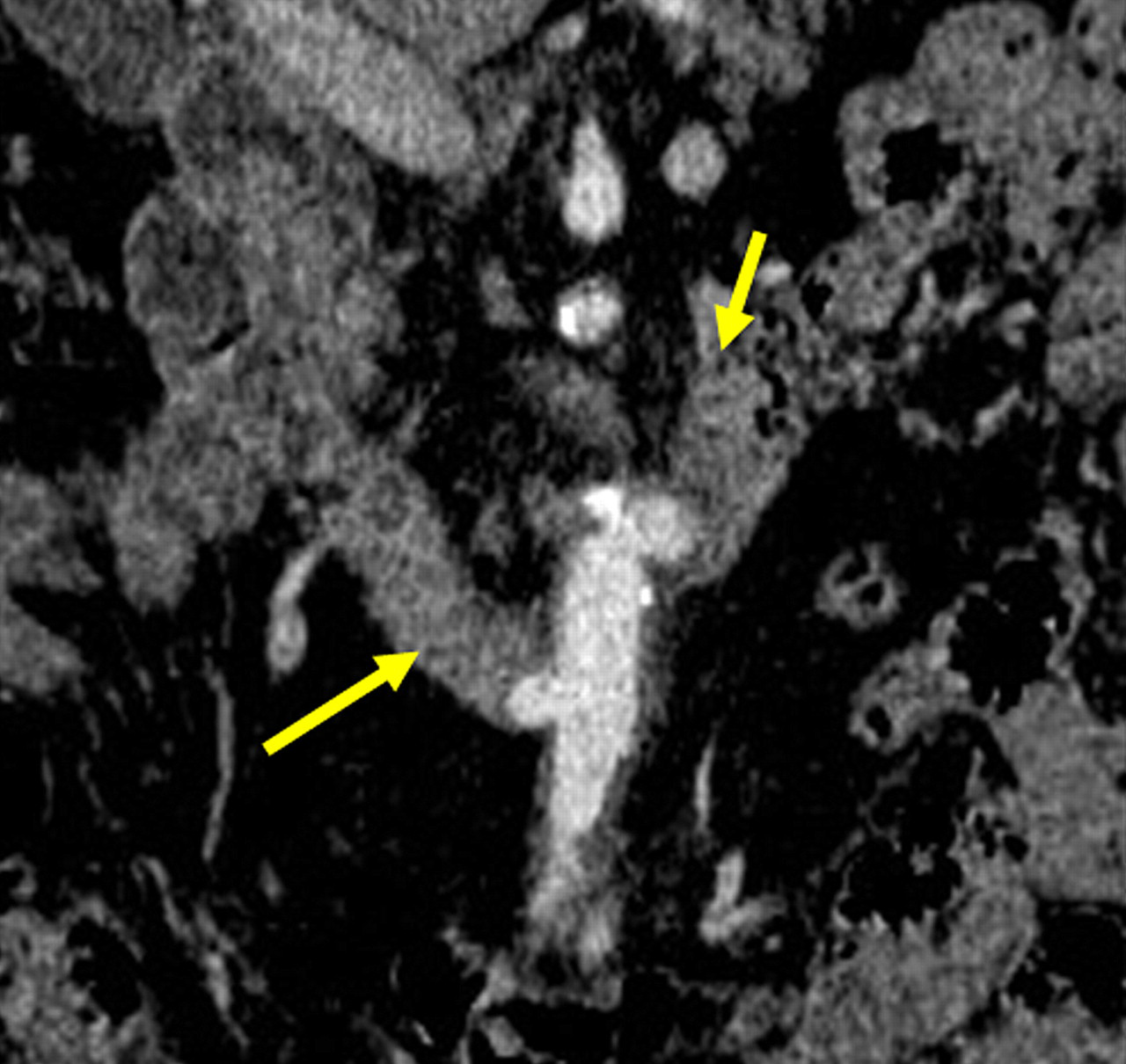
Contrast-enhanced computed tomographic scan showing several pseudoaneurysms, two of them in close contact to the third and fourth portions of the duodenum

Contrast-enhanced computed tomographic scan: pseudoaneurysm in close contact to the third portion of the duodenum
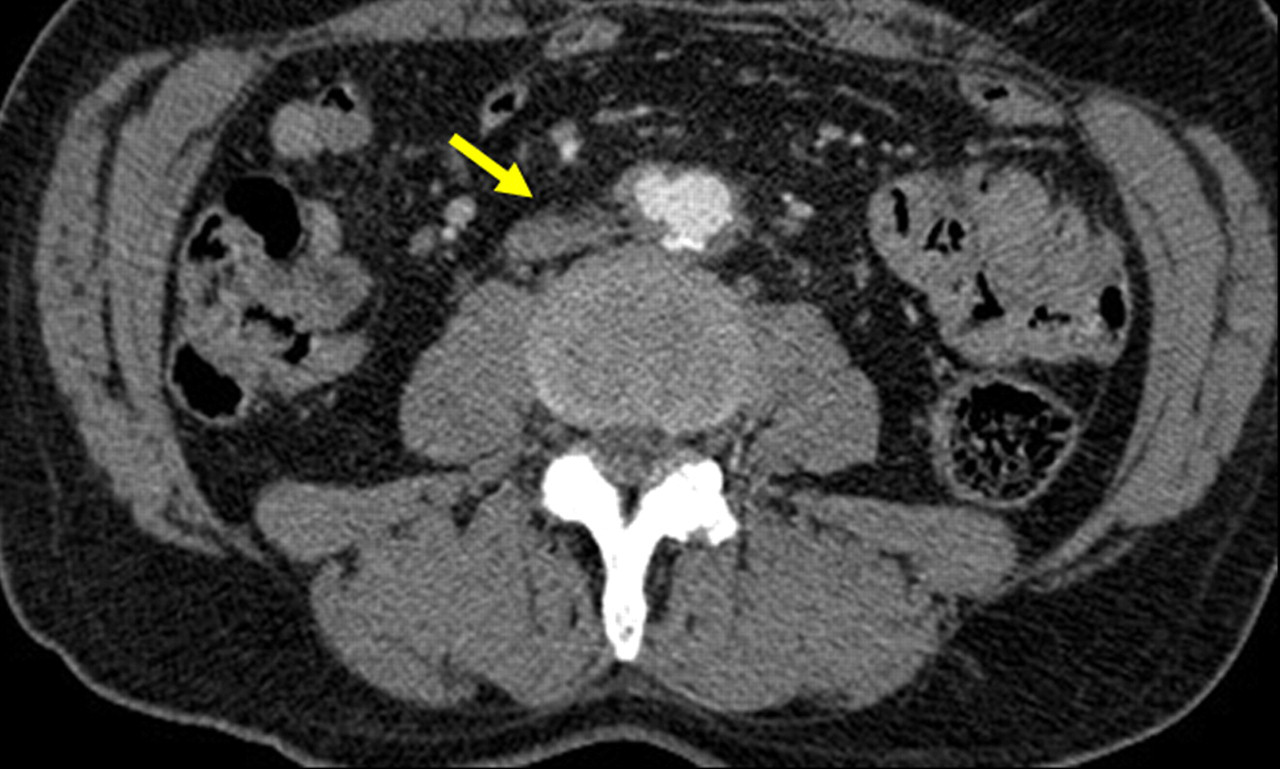
Contrast-enhanced computed tomographic scan: pseudoaneurysm in close contact to the fourth portion of the duodenum
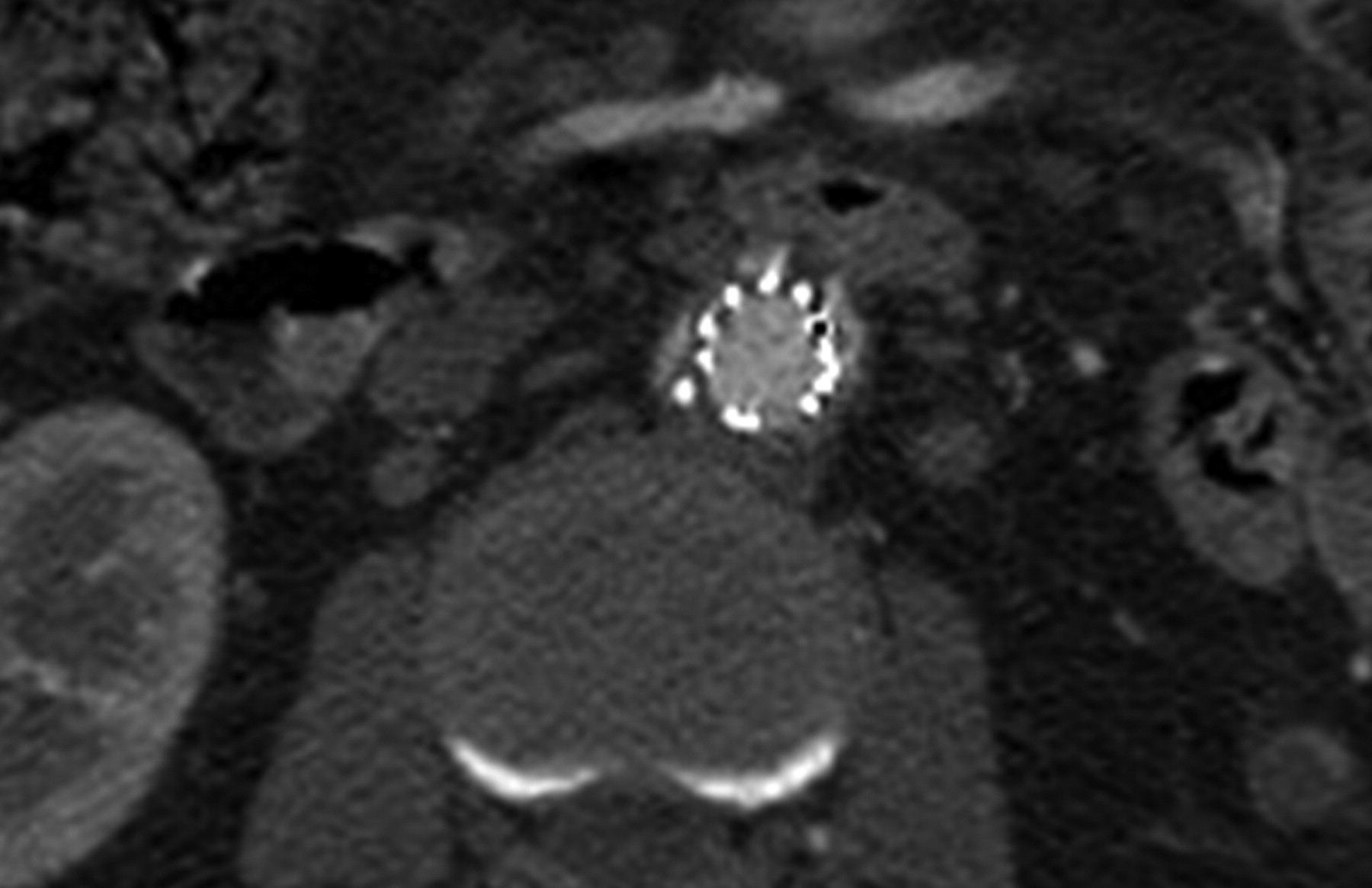
Contrast-enhanced computed tomographic scan 24 months after surgery showing pseudoaneurysms excluded, and no perigraft fluid, air or endoleak
Case 2
A 78-year-old man was admitted to the emergency department complaining of nausea and excruciating abdominal pain for two days. He suffered from severe chronic obstructive pulmonary disease (COPD) and was on home chronic oxygen therapy. On examination, his systolic blood pressure was 130 mmHg, heart rate was 116 bpm and temperature was normal. Laboratory tests showed a white blood cell count of 13,000/μL and a hematocrit of 35%. CT scans discovered the presence of an infrarenal pseudoaneurysm with a transverse diameter of 7 cm and active extravasation of contrast from aorta to the duodenum (Figures 5 and 6). Due to his high risk for an open-surgical procedure because of his severe COPD, an endovascular repair was performed under epidural anesthesia. Intraoperative angiography confirmed the presence of a pseudoaneurysm (Figure 7). A tube stent-graft (28 × 70 mm; Talent, Medtronic Inc) was introduced through an arteriotomy over the right common femoral artery and deployed to cover the abdominal aortic pseudoaneurysm. An intraoperative aortogram confirmed satisfactory positioning of the endograft, with complete sealing of the pseudoaneurysm sac (Figure 8). The patient received intravenous broad-spectrum antibiotic agents perioperatively, blood cultures were negative and no sepsis or signs of graft infection developed postoperatively; the hematemesis subsided after the procedure. As in the previous patient, non-operative management of perforated duodenum was performed. A control CTA on the ninth day showed no evidence of leak or digestive complications (Figure 9) initiating oral intake on the ninth day. Four weeks after surgery, his lung function deteriorated as a result of nosocomial pneumonia and he died on the 38th postoperative day.

Computed tomographic scan showing an abdominal aortic pseudoaneurysm of 7 cm with a tract of contrast going to duodenum
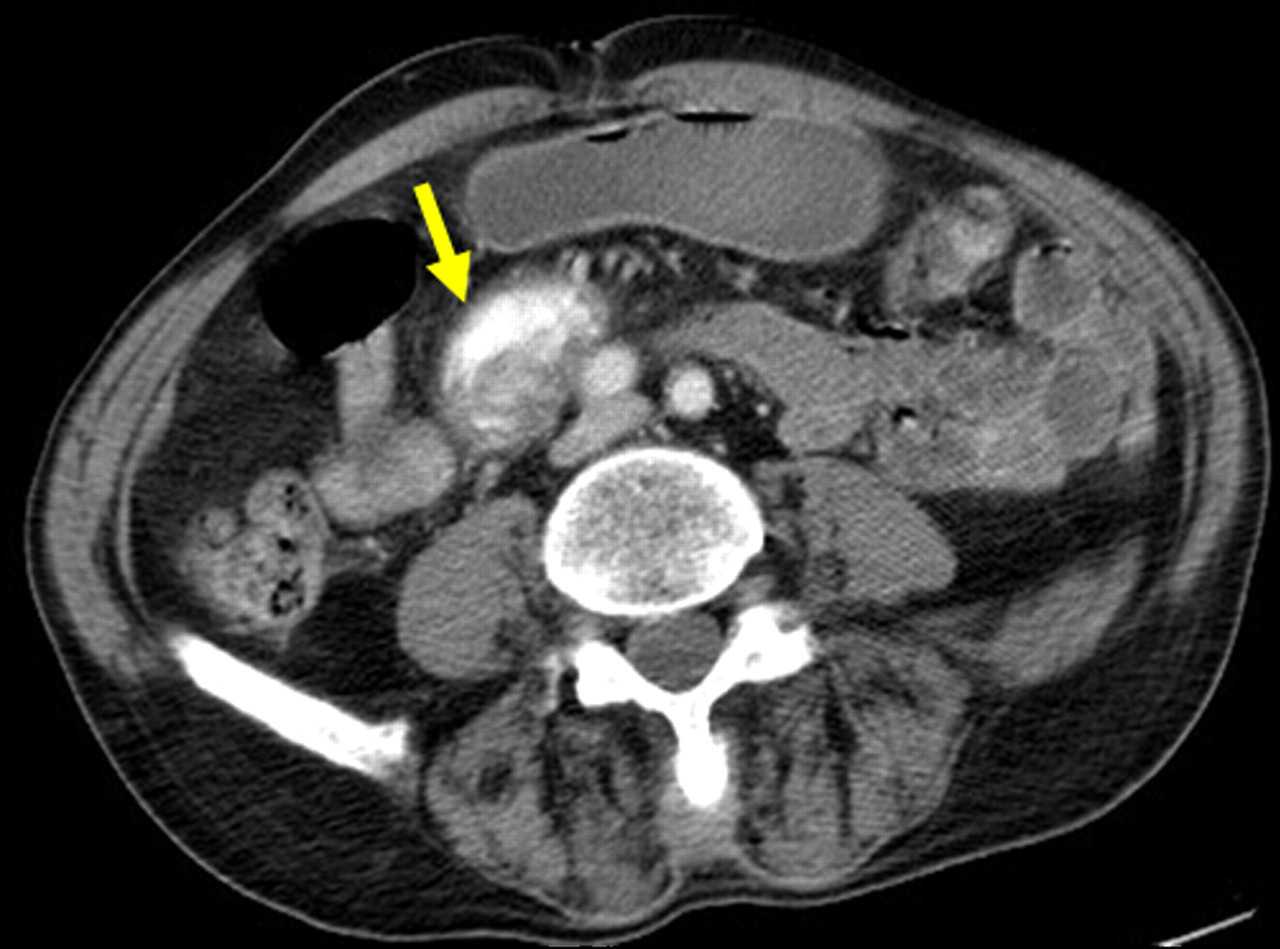
Preoperative computed tomographic scan with intravenous contrast shows extravasation of contrast from aorta to the duodenum (arrow denotes extravasation)
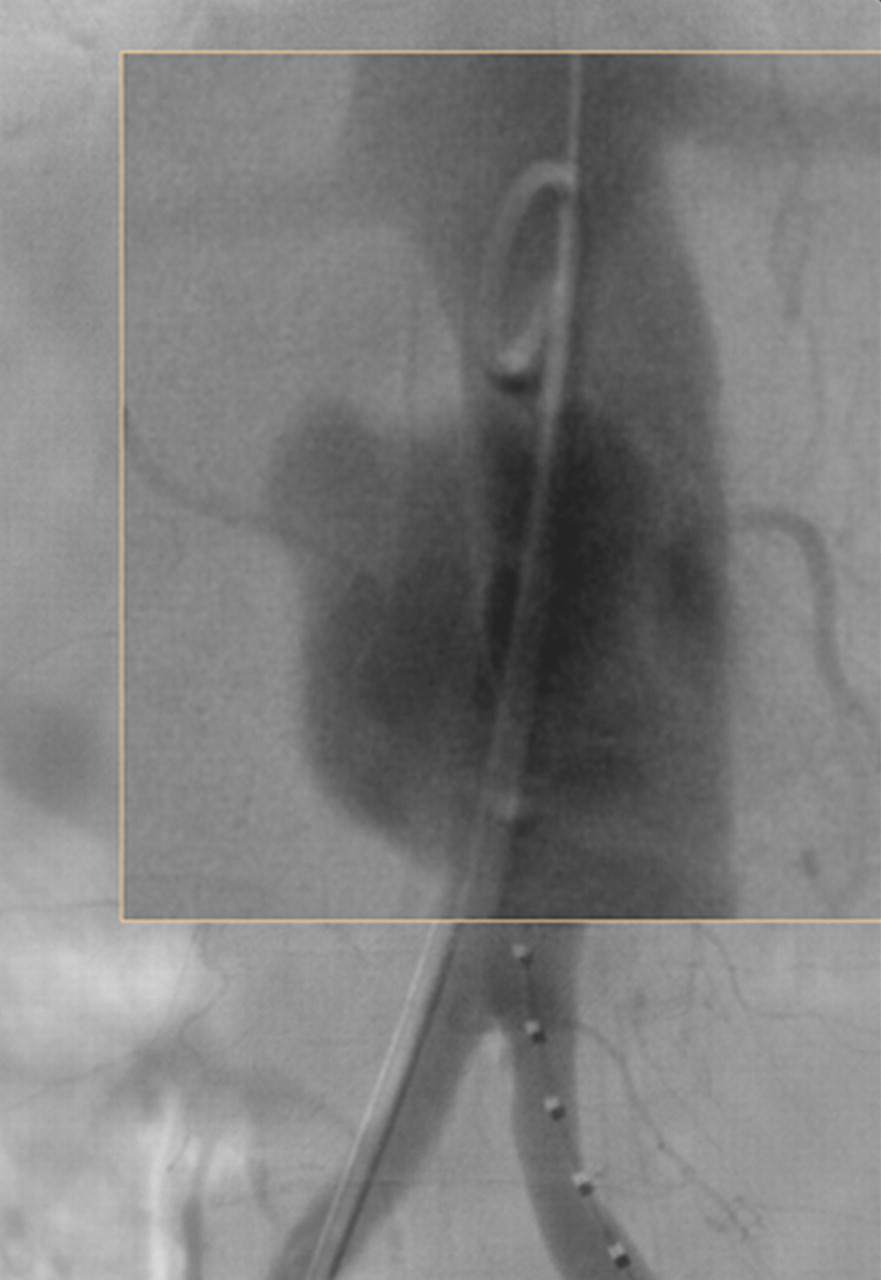
The intraoperative angiogram confirmed the presence of an infrarenal aortic pseudoaneurysm

After placement of a tube stent graft, the pseudoaneurysm and the aortoduodenal communication were completely excluded
Computed tomographic angiography on the ninth day showing no evidence of leak or digestive complications
Discussion
AEFs represent great diagnostic and therapeutic challenges in vascular surgery. Regardless of etiology, the traditional management goals of AEFs are: to control hemorrhage, to resect infected material, to repair the gastrointestinal fistula and to ensure adequate distal perfusion. Surgical treatment consists of intestinal repair, aortic ligation and an extra-anatomical bypass, or in situ repair in cases of minimal contamination of the aortic bed at the time of surgery, although it may be difficult to assess at laparotomy. Conventional surgical repair undertaken in a critically ill, hemodynamically unstable and septic patients is associated with high operative morbidity and mortality rates. 5 Furthermore, patients with AEFs often have multiple co-morbidities and limited life expectancies that may place them at high risk for open repair. Baril et al. 7 published their experience with AEFs, treated with open and endovascular repair over a nine-year period, and found an overall survival of 23 months. Burks et al., 9 reported that 50% of patients who survived the endovascular management of AEFs were dead within two years because of cardiopulmonary disease unrelated to their AEF.
Endovascular aortic repair offers a less invasive alternative than traditional open surgery to seal the aortic fistula and control bleeding in patients with AEFs. On the other hand, endovascular repair is limited because it does not include intestinal repair and may leave prosthetic material in contact with a contaminated area (the GI tract). However, in selected patients, in situ repair of AEFs is the preferred surgical treatment. 13 Futhermore, conservative treatment of a gastrointestinal perforation is an acceptable approach on selected patients. 14
The most relevant complication of successful endovascular repair for AEFs is recurrent infection. Danneels et al. 8 found re-infection or recurrent AEFs in 60% of 15 patients with AEFs, at 9.5 months follow-up after endovascular treatment. They recommended endovascular treatment as a bridge treatment to an open-surgical procedure when possible, except for patients unfit for open surgery. In a systematic review of 41 reported cases by Antoniou et al., 15 the incidence of infection or recurrent bleeding after endovascular stent-graft repair of AEFs was 44%. The factors associated with treatment failure (both 30-day and overall survival) were the evidence of preoperative sepsis, and persistent infection after surgical treatment. Most deaths were associated with septic or hemorrhagic complications. Burks et al. 9 reported that all patients who had obvious signs of graft infection either died or required adjunctive measures to control persistent sepsis The attempts to interrupt the communication between the aortic and bowel lumen with either minimally invasive or surgical methods were not associated with better results of endovascular treatment; 15 these procedures are recommend by Burks et al. 9 in patients with AEFs affecting the esophagus or the colon to decrease the risk of persistent sepsis. Patients should be treated with broad-spectrum antibiotics on empirical bases as it is almost impossible to obtain good samples for culture. Antibiotics should cover most common gastrointestinal flora and should be modified accordingly following the blood cultures results. If the cultures are positive, antibiotic therapy should be continued for four to six weeks. The duration of antibiotic treatment has not been well established although in a review by Antoniou et al., 15 lifelong antibiotic treatment did not prevent future sepsis.
For these two patients, endovascular repair was the best option. Patient 1 was on clopidogrel, due to a drug eluting stent placement, had had previous aortic surgery and was actively bleeding, and so was unfit for open surgery. In the second patient, the severe COPD made the risk of a procedure under general anesthesia unacceptable. Both patients were anatomically fitted for endovascular approach. The first patient had a pseudoaneurysm close to bifurcation of cryopreserved graft, and so it was not possible to deploy a tube graft; besides, the diameter of distal graft was not wide enough to fit an aortobiiliac endoprothesis. None of our patients presented signs or symptoms of infection at the time of the first procedure; postoperative CT with oral contrast showed no septic complications either. Based on the evidence that postoperative septic complications developed mostly in patients with active infection in the periprocedural period, we decided not to perform any open surgery on patient 1.
Conclusion
There is little consensus about the optimal management of AEFs. Endovascular management of AEFs provides rapid control of bleeding and, for patients fit for open repair, it can be used as a bridging procedure to definitive repair particularly in the setting of a systemic infection. Most patients presenting with AEFs are elderly and physiologically compromised, with multiple co-morbid conditions and a limited life expectancy. In these patients, who are poor candidates for open surgical aortic repair, endovascular treatment has been advocated as a definitive treatment.
These two cases confirm the importance of endovascular aortic repair as an effective alternative to standard open surgical management, especially in those situations when an open-surgical procedure is either difficult or not feasible.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: none reported.