
Abstract
Hypothenar hammer syndrome is a rare condition with a peculiar presentation that aids in making a clinical diagnosis. We present a 22-year-old male patient who presented with critical hand ischemia secondary to a distal ulnar aneurysm with distal embolization. The patient was treated with an aneurysmectomy with cephalic vein interposition graft, which resulted in complete reversal of his hand ischemia. This case report outlines the clinical presentation of this rare condition, along with a recent review of the literature.
Introduction
Diverse medical disorders can contribute to upper extremity ischemia; however, non-atherosclerotic conditions should be considered, especially in younger patients. Occupation-related arterial diseases include both thoracic outlet syndrome and, less commonly, hypothenar hammer syndrome (HHS). 1–5 The ulnar artery has a superficial course at the wrist as it crosses laterally to the hook of the hamate carpal bone (Canal of Guyton). This special anatomy makes the ulnar artery more prone to repetitive trauma in certain professionals.
Case report
A 22-year-old male construction worker presented with a three-week history of right hand pain associated with numbness and dry gangrene of the tip of his middle finger. On examination, there was a 15 × 15 mm pulsatile tender mass over the hypothenar eminence. The right upper extremity had normal radial and brachial pulses, sluggish capillary refill (>3 seconds), a positive Allen test and dry gangrene over the tip of the middle finger with coolness and numbness. Serological and hematological tests were normal. An arterial duplex study showed distal ulnar artery occlusion with no Doppler signal over the superficial palmar arch. Digital pressures were measured, and the middle finger pressure was 50 mmHg lower than the other fingers.
Dynamic right upper extremity arteriography was performed via the right femoral retrograde Seldinger approach and it showed a distal ulnar artery aneurysm at the level of the hamate bone, which is consistent with prior episodes of digital embolization (Figure 1). A diagnosis of HHS was confirmed, and surgery was immediately scheduled with routine intraoperative systemic heparinization with 80 units/kg intravenous bolus.
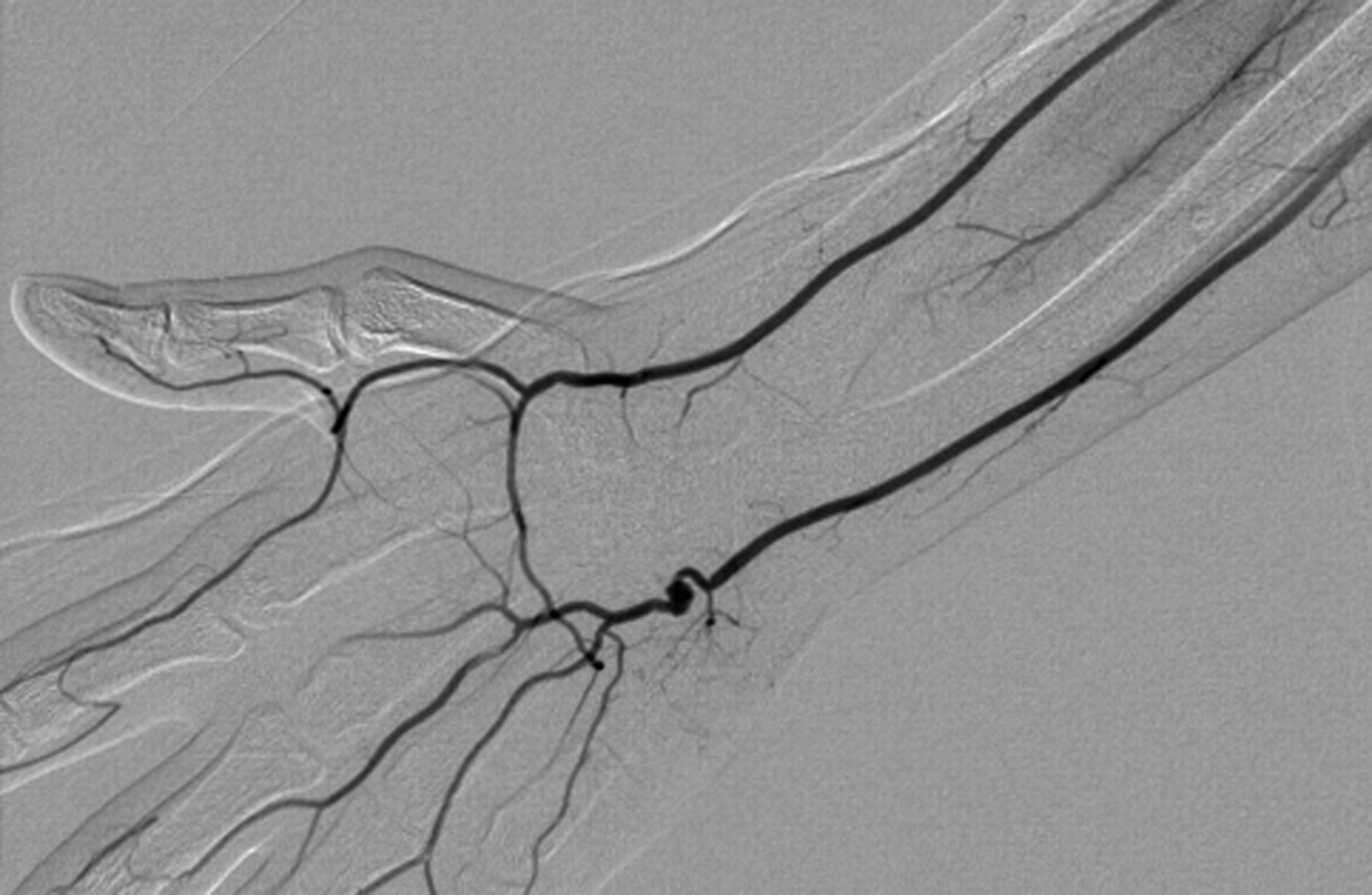
Arteriogram showing distal ulnar artery aneurysm, with distal embolization to the middle finger
Operative intervention was pursued with excision of the 12 × 11 mm aneurysm, with a reversed cephalic vein end-to-end interposition graft. Exclusion of the aneurysm by proximal and distal ligation was felt to be inadequate since there was side branch filling of the aneurysm, which was contributing to sac expansion (Figures 2 and 3). Pathological examination revealed an aneurysm of the distal ulnar artery with an intralumenal blood clot and fibrin. A completion Doppler examination showed triphasic signals over the distal ulnar artery, the superficial palmar artery and the deep palmar arch, as well as over the middle digital artery, with capillary refill of less than two seconds, indicative of spontaneous recanalization. There were no postoperative complications and the digital ischemia symptoms were resolved. The patient was discharged home on full dose aspirin. At the three-month follow-up, his middle finger tip wound was completely healed with normal hand function.
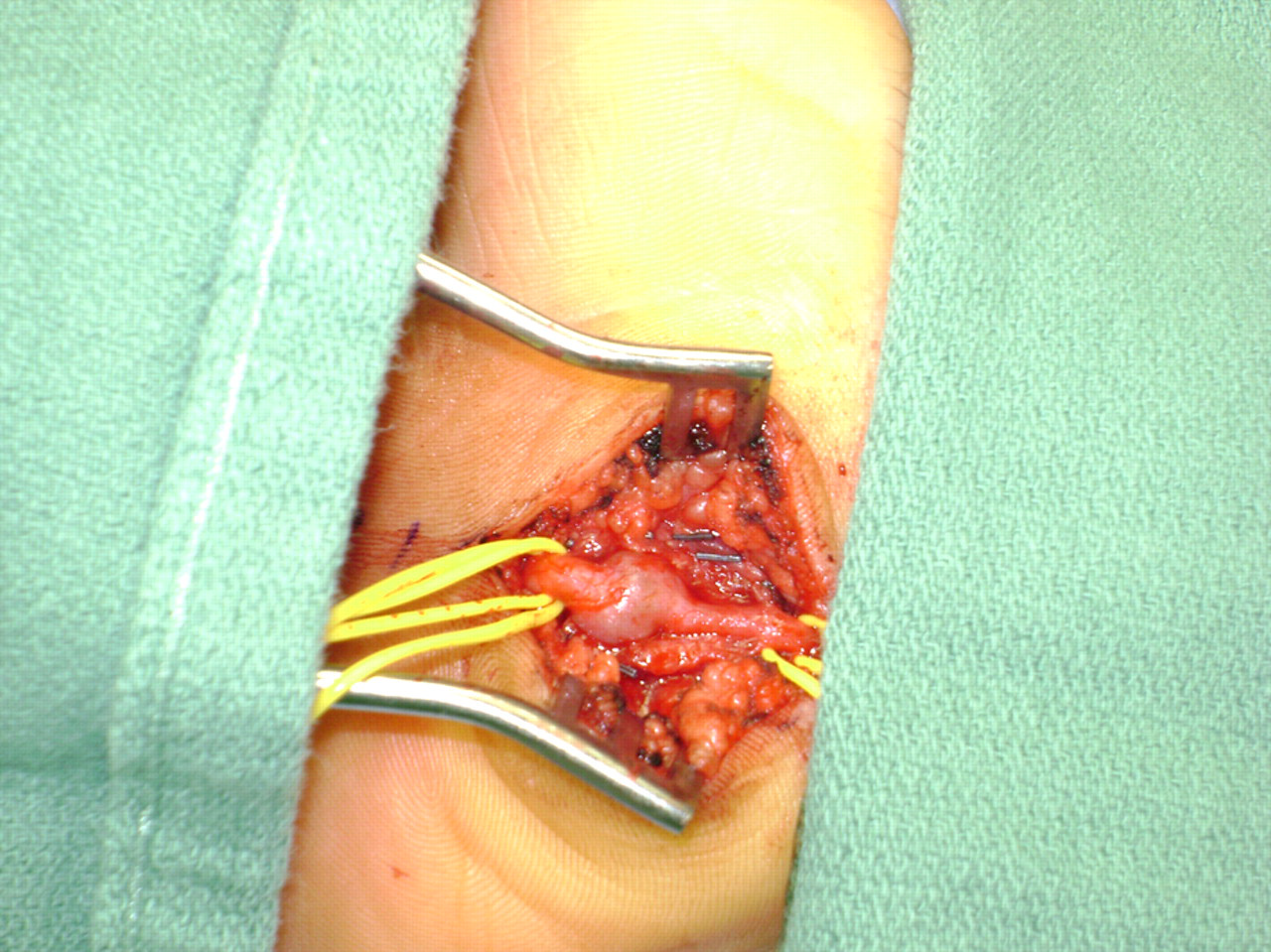
Surgical exploration of distal ulnar artery aneurysm with posterior side branch contributing to sac expansion after proximal and distal ligation

Interposition cephalic vein was used as a conduit after resection of the ulnar aneurysm
Discussion
Since first described by Conn in 1972, 1,2 HHS has been considered to be one of the occupation-related hand ischemia conditions that are secondary to repetitive trauma to the ulnar artery. There are a few mechanisms that can be contributed to HHS. The superficial course and possible friction injury to the palmar branch of the distal ulnar artery may predispose to endothelial injury with possible aneurysmal formation, which may contribute to thrombosis with subsequent distal digital embolization. Other mechanisms such as anomalous muscle predisposing to aneurysmal formation have been evaluated by others. 6 Diagnosis is mainly clinical, based on a history of repetitive trauma and clinical evidence of hand ischemia, and a positive Allen test is a pathognomonic to this clinical scenario. Noninvasive vascular laboratory studies are very helpful, not only for diagnosis, but also as a baseline for postoperative follow-up. A significant decrease in finger pressure may raise the suspicion of a distal aneurysm with embolic phenomena. The utility of computed tomographic angiography and magnetic resonance angiography in establishing diagnosis of HHS is well defined. 7,8 However, because HHS is uncommon, there is no definite consensus in the literature for an algorismic work-up regarding this condition (Table 1). We recommend individual discretion, depending on physician and institutional preferences.
A review of the English literature utilizing pubmed.org with keywords hypothenar hammer syndrome for all the review articles and case reviews for two or more HHS cases was conducted
MRA, magnetic resonance angiography; HHS, hypothenar hammer syndrome
An angiogram is necessary for many reasons: to define the location of the ulnar aneurysm for operative planning; to rule out any other pathological conditions that may contribute to hand ischemia, such as thoracic outlet syndrome; and to outline the extent of digital embolization, 9 as we can see occlusion of digital branches to the right middle finger (Figure 1). We found that exclusion of the aneurysm per se was not enough, since after proximal and distal ligation, the sac continued to expand secondary to the posterior side branch, which acts as a type II retrograde endoleak (Figure 2). Again, the posterior side branch could have been ligated to completely exclude the aneurysm. However, given the small space in the hand, an aneurysmectomy is generally performed for this condition. The purpose of the interposition was presumably revascularization, which is commonly achieved with a vein graft. 10–13 Others have advocated using the inferior epigastric artery as a conduit, 14 assuming a better patency rate based on the coronary artery bypass graft surgery patency data. Also, resection of the aneurysm with end-to-end anastomosis has been described. 15 Ferris et al. 12 reported on the largest series of patients with HHS, with a hypothesis that HHS results from trauma to an intrinsically abnormal artery. Long-term outcome of ulnar artery reconstruction with a vein graft was described in 14 patients over a mean of 52 months, and improvement of the digital brachial index and a subjective evaluation were noted. 16 Another retrospective study of six patients recommended surgical reconstruction of the ulnar artery distal aneurysm as a durable treatment option. 17
In one series of 21 patients, 12 a histological examination of the excised ulnar artery demonstrated fibromuscular dysplasia with superimposed trauma in all 19 specimens examined; also they reported that bilateral upper extremity arteriograms were obtained in 13 of their patients. Eleven of these patients had similar angiographic findings in the contralateral normal hand, suggesting an underlying predisposition to the development of HHS. The authors concluded that HHS does not develop in most patients with repetitive trauma to the hand because their ulnar arteries are normal; therefore, keeping a high index of suspicion is crucial to act before complications. A normal arterial duplex study of the contralateral arm was noted in our patient. Persistence of postoperative digital ischemia, in spite of successful revascularization, may warrant further angiographic evaluation and possible thrombolysis therapy. 18
Little and Grant 4 and Little and Ferguson 19 reinforced the correlation of the duration of employment with the development of this syndrome. HHS is a relatively uncommon condition of arterial hand ischemia and it should be considered in our differential diagnosis for early diagnosis and management.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: none reported.