
Abstract
Degenerative arterial aneurysms can occur in any vascular territory. However, they are exceedingly rare in the axillary artery. Complications of axillary artery aneurysms may result in acute vascular insufficiency and neurological deficits. Prompt treatment should be employed in the management of this condition. We report a case of an atraumatic degenerative axillary artery aneurysm that was treated with transaxillary open surgical bypass.
Introduction
True axillary artery aneurysms are typically associated with a history of blunt or penetrating trauma, with congenital, atherosclerotic and degenerative etiologies being rare. There have been a few reports in the literature describing atraumatic atherosclerotic aneurysms of the axillary artery. We report a rare case of an axillary artery aneurysm in a patient with no history of prior trauma and no atherosclerotic or degenerative changes detected upon histopathological evaluation of the aneurysmal specimen.
Case report
A 90-year-old woman, with a past medical history significant for hypertension, presented with a sudden onset of right upper extremity pain, weakness, coolness and paresthesias. She had no tissue loss and was referred for evaluation secondary to progressive discomfort. She had no history of arrhythmias, hypercholesterolemia, aneurysmal disease, deep venous thrombosis or hypercoagulable disorder. She was a smoker with a 70-pack-year history. She denied a history of previous upper extremity or chest trauma. On clinical evaluation, the left upper extremity pulse exam was normal whereas there was an absence of brachial, radial and ulnar pulses on the right. She had a prominent pulsatile mass in the right axillary fossa. She had cyanosis of the right hand, with prolonged capillary refill but a normal neurological exam.
A computed tomography scan of the neck and chest with intravenous contrast was performed, which demonstrated a 2.7-cm mass of the distal right axillary artery with associated thrombus (Figure 1). Anticoagulation was initiated and an angiogram of the right upper extremity was performed. This demonstrated a thrombosed axillary artery (Figure 2). Brachial artery to radial and ulnar arteries were patent, with sluggish flow to the hand.
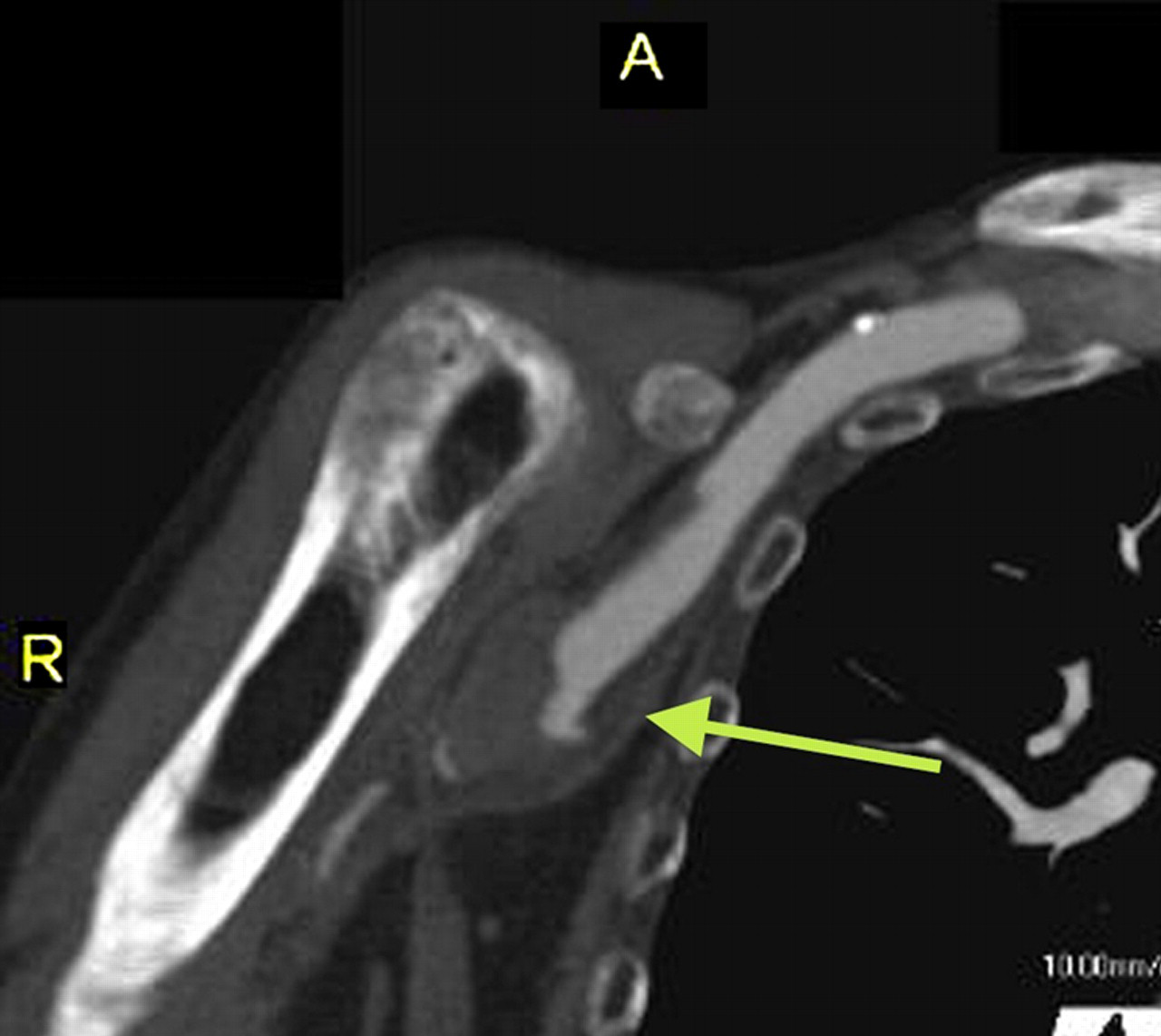
Computed tomography of the shoulder showing thrombosis of the right axillary artery with aneurysm

Angiogram of the right axillary artery showing complete occlusion
She was taken to the operating room for revascularization of the right upper extremity.
A 6-cm incision was made on the medial aspect of the right upper extremity just under the pulsatile mass. The brachial artery was dissected. Proximal and distal control was obtained. This was done in anticipation of a bypass, but the aneurysm appeared to be limited and the dissection was further carried out proximally until normal caliber axillary artery was seen. Care was taken not to injure the brachial plexus. It was felt that an interposition graft would be feasible. The aneurysm was opened, and the clot was removed. A tapered Gore-tex graft (W L Gore and Associates, Inc, Flagstaff, AZ, USA) was interpositioned between the axillary and the brachial artery. A radial artery pulse was noted after the completion of the surgery. Postoperatively, the patient did well and was discharged home. Cultures obtained in the operating room did not grow any organisms. The final pathology was consistent with the arterial wall, and associated blood clot. On follow-up, she remained with fully intact pulses, and no further studies were necessary.
Discussion
Aneurysms of the upper extremities are rare in relation to other peripheral aneurysms. In spite of their rarity, upper extremity aneurysms can result in profound disability secondary to inadequate diagnosis and management. The uncommon nature of aneurysms in this location lends the upper extremity symptoms to be ascribed to an alternative etiology. However, with the advent of more sophisticated imaging modalities, these aneurysms are now less likely to be missed. Prompt recognition can avoid adverse neurological and vascular sequelae. These complications include digit and limb loss, stroke from embolization into more proximal vertebral and right carotid arteries, and exsanguinating hemorrhage. 1
Involvement of the axillary artery is rare among the upper extremity aneurysms, with the subclavian artery more commonly affected. Aneurysms of the axillary artery are generally secondary to blunt or penetrating trauma, causing arterial degeneration. This includes the use of axillary crutches, or in high-stress overhead arm motions during athletic activities. In this set of patients, the cause of axillary artery aneurysms is hypothesized to be secondary to repetitive compression of, or tension on, the vessels at the level of the pectoralis minor muscle and the humeral head, especially in baseball pitchers. 2,3 Infectious and degenerative causes are unusual, but have been reported. 4,5 Atherosclerosis, collagen vascular disease, mycotic aneurysm and thoracic outlet syndrome have also been described as etiologies. 2,3,6–8 Advanced age, like in our patient, has not been previously reported as a risk factor. Patients typically present with pain, numbness and coolness in the affected extremity. Complications such as thromboembolism, progressive distention of the aneurysm, brachial plexus compression, rupture of the aneurysm and local infection may also occur, warranting prompt intervention.
Surgical resections with end-to-end anastomosis, if necessary with autologous or artificial patch repair, are the standard treatments for peripheral aneurysms. Aneurysmectomy and interposition grafting with a saphenous vein is also an option for many patients with axillary artery aneurysms, although size matching may be difficult. Brachial or axillary veins may also be used; however, because these veins tend to develop aneurysms, saphenous veins should be the first choice when available. 3 Prosthetic grafts, such as polytetrafluoroethylene, are also used successfully for reconstruction. They are a good alternative when the quality of the saphenous vein is inadequate or lacking.
Management of select aneurysms using stent grafts has become more prevalent with the developing endoluminal technology. It can be an effective and less invasive alternative to the standard surgical repair, but only a few cases have been described in the literature with respect to axillary artery aneurysms. 9 Stenting across a mobile joint, such as the shoulder, can lead to problems like deformation and fractures of the stent. With the advent of stent grafts with increased flexibility, less compressibility and deformability, the role of endovascular treatment of peripheral aneurysms is promising.
Conclusion
Axillary artery aneurysm is a rare entity. Yet, prompt diagnosis and surgical treatment is important to avoid complications. Rupture with life-threatening blood loss, thromboembolism leading to ischemia and limb loss, or irreversible neurological damage may occur. Open surgical therapy has been the standard of care with excellent results, but endovascular therapy is an evolving option.