
Abstract
Angiolymphoid hyperplasia with eosinophilia (ALHE) is an unusual vascular tumor most frequently located in the superficial head and neck. Noncutaneous localization of this pathology in large arteries presenting as a pulsatile mass is extremely rare. We describe an adult male with a giant left axillary artery tumor secondary to ALHE. ALHE should be considered in the differential diagnosis of localized peripheral arterial masses, especially in young patients.
Angiolymphoid hyperplasia with eosinophilia (ALHE) is an uncommon benign vascular neoplasm manifested by multiple or solitary subcutaneous nodules, usually on or about the head of young adults. ALHE is characterized microscopically by marked proliferation of large endothelial cells with a mixed inflammatory infiltrate consisting of lymphocytes, histiocytes, and eosinophils.
Case Report
A 30-year-old male presented with a history of swelling in the left axillary region for the past 7 years. The swelling was gradually increasing in size to attain the present size of about 15 cm, resulting in limitation of movement at the left shoulder joint. The patient had a history of numbness over the left upper limb of recent onset. There was no history of trauma in the past. He also had a history of a dry cough with wheezing for the past 10 years that required multiple hospital admissions, which, in retrospect, was related to eosinophilia. His past medical records revealed persistent eosinophilia. He had no family history of asthma.
Clinical examination revealed a pulsatile swelling in the left axillary area measuring about 15 × 18 cm and disturbing adduction of the left upper limb (Figure 1A). The skin over the swelling was stretched. There was a significant difference in the brachial artery pulse and blood pressure (right upper limb 120/80 mm Hg, left upper limb 90/60 mm Hg). Examination of the respiratory system revealed extensive ronchi. A complete hemogram showed eosinophilia (56%) with an absolute eosinophil count of 17,920 cells/mm3. Other routine biochemical investigations were normal. A chest radiograph was normal, with no evidence of rib or bony erosion. Magnetic resonance imaging of the swelling showed aneurysmal dilatation of the left axillary artery surrounded by a thick enhancing soft tissue mass (Figure 2). Magnetic resonance angiographic reconstruction (Figure 3) revealed a left axillary artery aneurysm within the mass. There was no thrombus within the aneurysm.
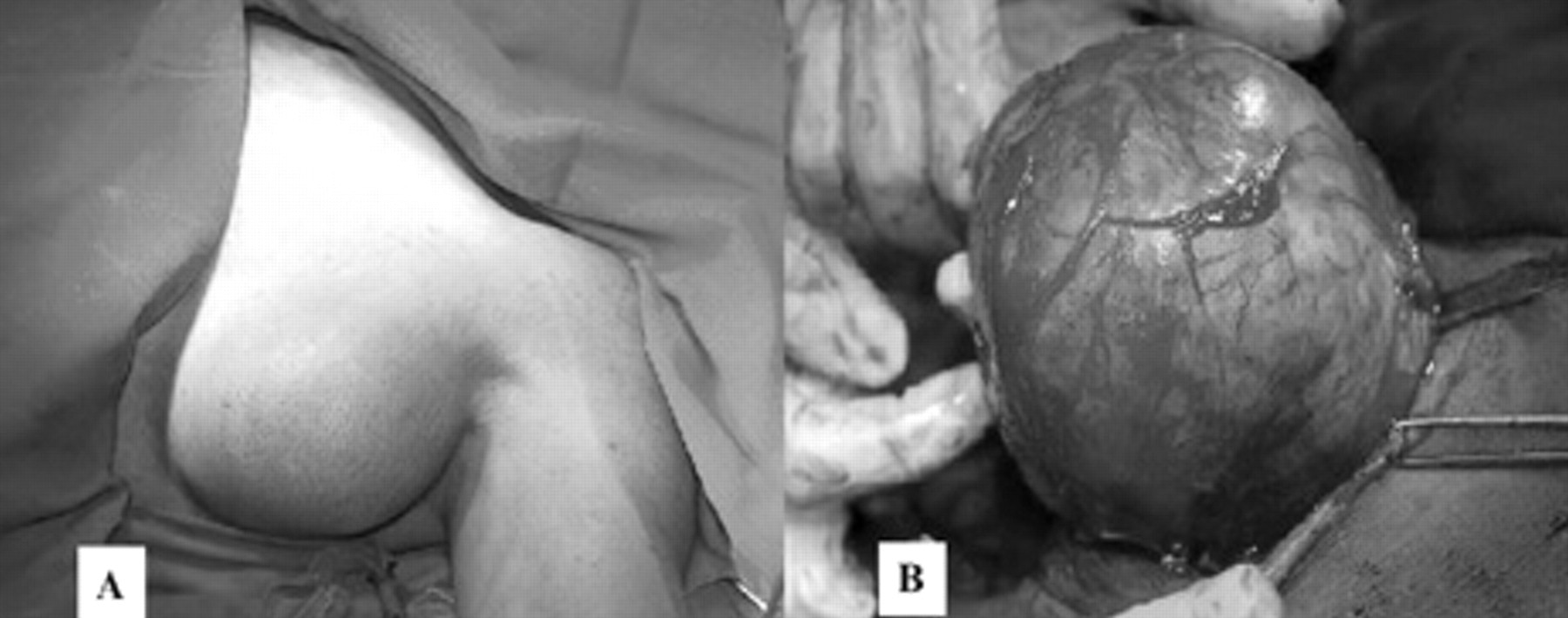
A, Preoperative photograph showing a giant axillary artery aneurysm. B, Intraoperative photograph showing a giant axillary artery aneurysm during excision.

A, Magnetic resonance T1-weighted gated image of the mass showing an axillary artery aneurysm surrounded by a mixed-intensity soft tissue mass. B, Magnetic resonance T2-weighted gated image of the mass showing an axillary artery aneurysm surrounded by a mixed-intensity soft tissue mass.

Magnetic resonance angiographic reconstruction image showing an aneurysmally dilated left axillary artery within the tumor.
Intraoperatively, a well-encapsulated fusiform mass involving the left axillary artery attached proximally to the left subclavian artery and distally to the axillary artery was noted (Figure 1B). The mass was adherent to the brachial plexus, and the axillary vein was noted. Under general anesthesia through a linear incision along the axilla, the swelling was dissected out, taking care to preserve the brachial plexus and axillary vein, and the tumor was resected in toto. The gap of 6 cm in the axillary artery was bridged with a saphenous venous graft taken from the left leg.
The postoperative period was uneventful, with improvement in the left upper limb blood pressure and no neurologic deficits.
On histopathologic examination of the resected mass measuring 12 × 10 × 5.5 cm, the entrance of the medium-sized vessel into the mass was identified. A sac-like opening was seen within the mass. The mass had a thick gray-brown wall. Microscopic examination of sections showed thickened adventitia of the vessel wall with a dense infiltrate of lymphoid cells forming follicle at places (Figure 4A). Microscopic examination also showed prominent infiltrate of eosinophils (Figure 4B) as well as numerous vessels with endothelial proliferation. The features were consistent with ALHE of the axillary artery. The detailed workup to evaluate other causes of persistent eosinophilia yielded negative results.
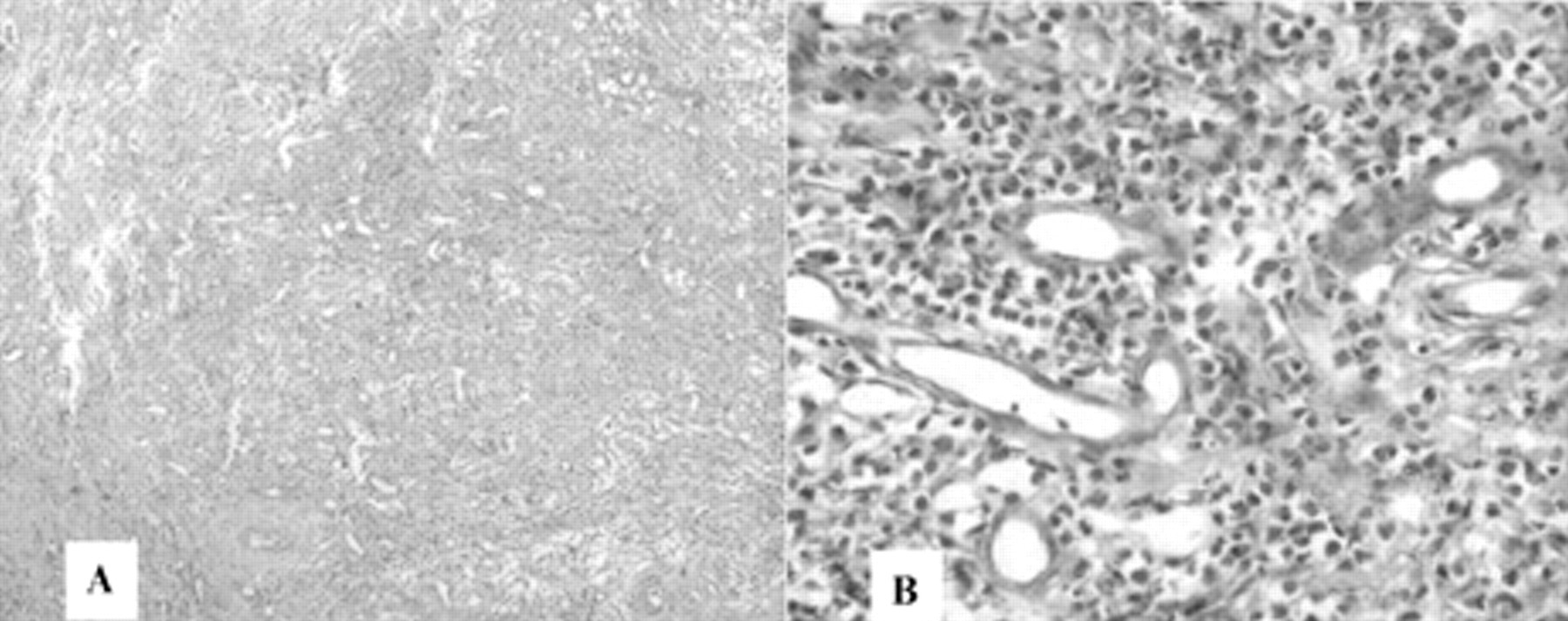
A, Microscopic picture in low power showing a dense infiltrate of lymphoid cells forming follicle at places (hematoxylin-eosin stain; ×100 original magnification). B, Microscopic picture in high power showing prominent infiltrate of eosinophils (hematoxylin-eosin stain; ×1000 original magnification).
To our surprise, at 1 week postoperatively, the repeat hemogram showed a near-normal differential count with an absolute eosinophil count of 650 cells/mm3, which was sustained at the 6-month follow-up. There was a dramatic improvement in the patient's wheezing and cough.
Discussion
ALHE is an unusual vascular tumor most frequently located in the superficial head and neck. The lesion rarely arises from a native blood vessel, as seen in our case. ALHE is a benign vascular lesion that is characterized by well-formed, capillary-sized vessels lined by histiocytoid or epithelioid endothelial cells and often accompanied by a secondary inflammatory infiltrate. 1 Characteristic histopathologic features include an exuberant proliferation of small-caliber, capillary-sized blood vessels and diffuse inflammatory infiltrate. The proliferation of blood vessels has a vague lobular pattern and frequently surrounds a larger blood vessel. The endothelial cells are commonly hypertrophic and sometimes form solid cords with cytoplasmic vacuoles resembling primitive lumina. The inflammatory infiltrate consists of abundant eosinophils along with lymphocytes, plasma cells, macrophages, and mast cells. Lymphoid follicles with germinal centers can be seen, particularly at the periphery of the lesion. 2 Twenty percent of cases also have generalized eosinophilia and occasionally raised serum IgE levels. 3
This tumor has been reported thrice from the radial artery 4–6 and the occipital and brachial arteries. 7 It has also been reported in the heart. 8 The series reported by Fetsch and Weiss showed that in 63% of cases, an artery or a vein was associated with the mass, and in the majority of cases, the vessel was damaged. 1 It rarely regresses spontaneously, but there are no reports of metastatic spread. 9
Originally, this condition was considered the same entity as Kimura disease, described in Asian patients. More recent histologic studies indicate that ALHE and Kimura disease are different clinical and histologic entities. 10–14 The differential diagnosis of this lesion based on clinical and/or histopathologic findings includes pyogenic granuloma, nevus, keratosis, reaction to insect bite, hemangioma, glomus tumor, malignant angioendothelioma, angiosarcoma, and Kaposi sarcoma.
Surgical excision has been regarded as the treatment of choice, but recurrences have been reported, particularly after incomplete removal. 15–17 Topical, intralesional, or systemic steroids; lasers; electrodesiccation, radiation, and cryotherapy have also been used to treat localized ALHE involving smaller lesions in skin. Other treatment options include pentoxifylline, indomethacin farnesil, systemic retinoids, interferon-α, and vinblastine, with variable results. Relapses have been treated successfully with reexcision, oral corticosteroids, and vinblastine, but for larger lesions involving major arteries, excision with reconstruction of the artery is the treatment of choice. In our patient at the 6-month follow-up, there was no recurrence, but there was improvement in eosinophilia and its associated respiratory symptoms.
Conclusion
Even though ALHE commonly arises within the dermis and subcutaneous tissue of the head and neck, it can also arise from major peripheral arteries, albeit rarely. ALHE should be considered promptly in cases of a pulsatile mass arising from the peripheral arteries as early diagnosis and timely surgical excision will lead to complete cure and relief from eosinophilia.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.