
Abstract
Abdominal aortic aneurysm surgery associated with a horseshoe kidney (HSK) is a serious technical challenge for the surgeon. We reviewed our experience with 127 patients electively operated on between 1990 and 2004 for abdominal aortic aneurysm. Pre- and perioperative medical, surgical, and radiologic data were retrospectively reviewed. Preoperative diagnosis was achieved with computed tomography with or without angiography or with additional conventional aortography.
Seven patients were recognized to have had a HSK, with a mean age of 67.29 ± 2.43 years. Preoperative serum creatinine levels were similar in patients with or without HSK (1.0 ± 0.08 vs 0.9 ± 0.12 mg/dL; not significant). In five of the patients with HSK, reimplantation of the anomalous renal artery was necessary. In all 127 patients, hospital mortality consisted of 5 patients, none of whom had an HSK. Dealing with HSK seemed to increase aortic clamp times (30.43 ± 3.55 vs 27.04 ± 3.92 minutes; p < .05) slightly. Patients with or without HSK were given similar amounts of intravenous fluid replacement (2,214.2 ± 441.3 vs 1,923.3 ± 433.6 mL/patient; not significant) and allogeneic blood transfusion (0.71 ± 0.49 vs 0.9 ± 0.4 U/patient; not significant) and had a similar intensive care unit stay.
Abdominal aortic aneurysms associated with HSK have been managed without division of the isthmic tissue. The left retroperitoneal approach provided adequate exposure for all patients with HSK.
The incidence of horseshoe kidney (HSK) varies from 1:400 to 1:1,000, and its association with abdominal aortic aneurysm (AAA) is rare. 1–3 The presence of this anatomic variation may complicate surgery because it may be adhered to the aneurysm sac, with a possible bulky isthmus and a possible need to divide it, or it may have an anomalous arterial supply or venous drainage requiring some kind of surgical reconstruction in up to 60% of patients. 4 Another surgical consideration includes renal pelvis anomalies or extrarenal calyces. Preoperative diagnosis and evaluation of such anomalies in AAA surgery are warranted for surgical workup, and possible perioperative risks are considered. Additional renal angiography is indicated to show a possible anomalous blood supply to the HSK. This approach is accepted commonly in the modern era of computed tomography (CT). Intraoperative observation was the usual scenerio in most cases before then.
A retroperitoneal surgical approach and endovascular exclusion of the aneurysm are the methods of choice for elective repair. 2,5,6 Endovascular methods have become more popular recently; however, only early results from a highly limited number of patients are available. Usually, a surgical approach from the left retroperitoneal space is recommended, particularly in patients with large anterior renal arteries or multiple and relatively dominant accessory arteries.
Methods
In this retrospective analysis of 127 patients with AAA who underwent nonemergent open surgical procedure with a left retroperitoneal approach among 259 surgical patients between 1990 and 2004, medical charts, operative and intensive care unit (ICU) records, and pre- and postoperative radiologic data were reviewed in particular to recognize patients with HSK. Institutional review, ethics committee approval, and informed consent from each patient were acquired. Ruptured aneurysms and those treated with other surgical or nonsurgical strategies were excluded from the analysis (112 patients with transperitoneal incision with 40 patients operated in the emergency settings; 20 patients with endovascular intervention). Pre- and perioperative comorbidities and complications were noted. Mortality was depicted as death within 30 days after surgery. Hospital stay was defined as the length of stay in the hospital from the day of surgery. Nonfatal complications were life-threatening complications that did not end in death. Diagnosis was established with abdominal ultrasonography, CT with or without angiography (ie, CT angiogram), or CT with additional conventional aortography when indicated. Among the postoperative complications, acute myocardial infarction was diagnosed according to the American Heart Association/American College of Cardiology criteria 7 ; acute renal failure was diagnosed with perioperative onset of oliguria or anuria and/or if a previously normal serum creatinine level exceeded 1.8 mg/dL. Neurologic states were evaluated using National Institutes of Health criteria 8 . Colonic ischemia and peritonitis were diagnosed on clinical examination and direct explorative laparotomy. An anomalous renal supply was considered in the case of multiple renal arteries (more than two) and/or arteries other than those originating bilaterally from the aorta (eg, anterior or more distal origin). Statistical procedures were done by using SPSS, version 10.0 (SPSS Inc, Chicago, IL). Data are expressed as mean ± standard deviation. A p value of less than .05 was considered statistically significant. Fisher exact test, Levene F-test, and the independent-samples t-test were used for the statistical evaluation of data.
Results
Seven patients (six males, one female) with an AAA and HSK (Figure 1, Table 1) were detected in this 14-year-long period. Diagnostic workup for 32 of 120 non-HSK patients included only abdominal ultrasonography and aortography; the remaining were diagnosed with contrast-enhanced CT scan. Five patients with HSK were recognized to have had CT scan, and the angiographic workup was achieved by means of conventional aortography in all but one, who had a CT angiogram. In two of the patients with HSK, preoperative diagnosis of HSK was not possible with ultrasonography, and an intraoperative diagnosis was done (one had a low-quality CT scan with limited resolution and number of slices, which also failed to show HSK). In all seven patients, operative records revealed adequate exposure with a left retroperitoneal approach. Management of AAA with HSK was achieved by retracting the HSK medially and opening the sac laterally, even sometimes posterolaterally when appropriate. The isthmus was never divided, and the distal portion of the synthetic graft was passed behind the HSK. Direct anastomosis of a distally originating renal artery to the graft was applied in three patients (bilaterally low origin in one patient); anastomoses of one and two large isthmic branches (lumen diameter > 3 mm) to the graft were achieved with the Carrel button technique in two patients, respectively, and reimplantation was not necessary in the remaining two patients. In the first of the latter patients, the artery to the HSK originated above the clamp (Figure 2). Topical cooling of the HSK was not used in any of the patients. Additionally, in the non-HSK group, reanastomosis of left renal artery in 10 patients and reanastomosis of both renal arteries in five patients were necessary. As a general approach, the aortic clamp was “lowered” on the graft as soon as the proximal anastomosis and the reimplantation of the renal arteries were completed so as to minimize renal ischemic time. One of the patients with HSK had concomitant left renal artery stenosis with normal pre- and perioperative creatinine levels. A concomitant left renal endarterectomy was performed. This series also included two patients with an inflammatory aneurysm, one in the HSK group (Figure 3).

Preoperative contrast-enhanced computed tomographic scan of an abdominal aortic aneurysm associated with a horseshoe kidney.

Three-dimensional reconstruction of a postoperative computed tomographic angiogram of an abdominal aortic aneurysm associated with a horseshoe kidney.
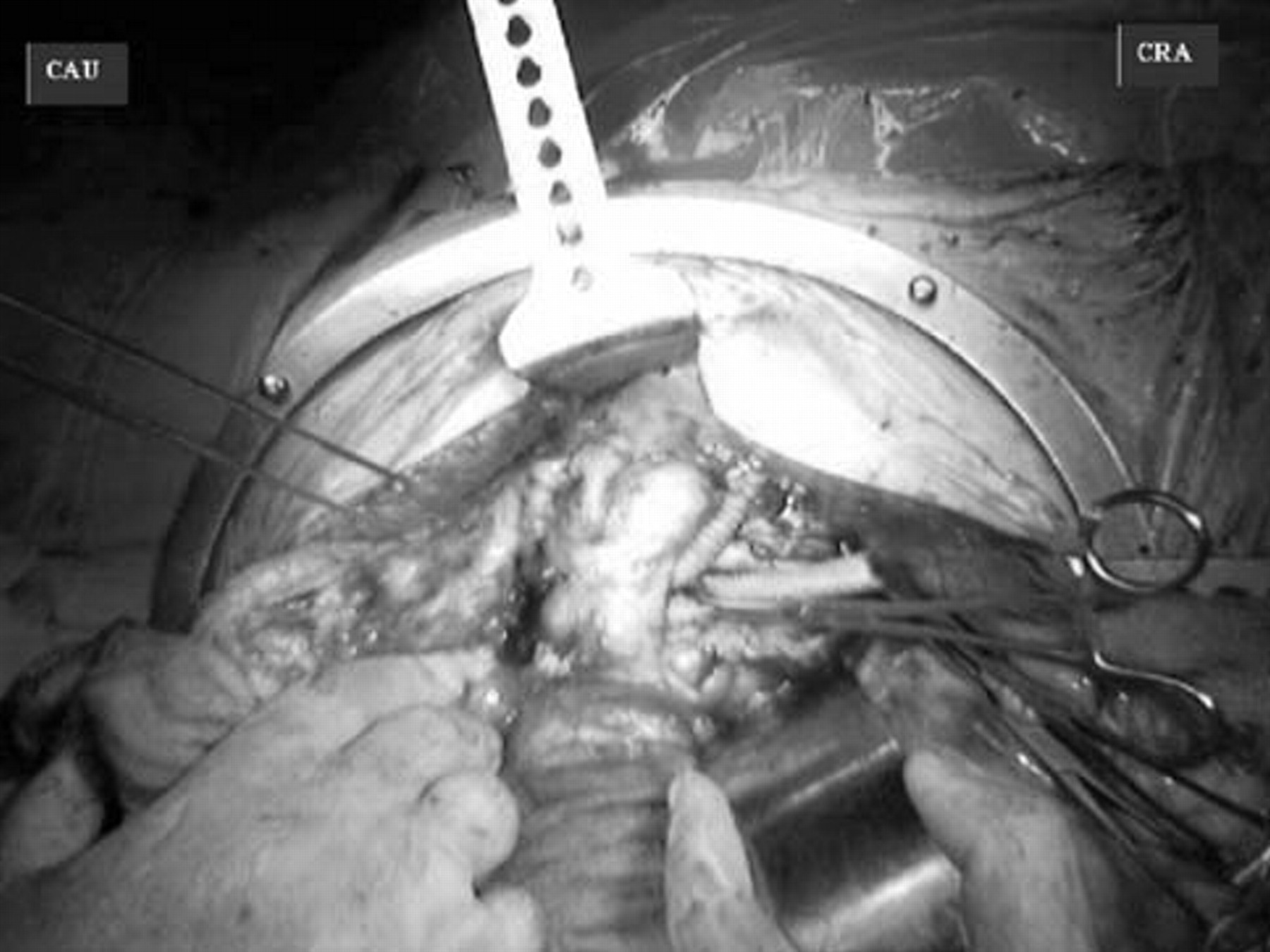
Operative view of an inflammatory abdominal aortic aneurysm associated with a horseshoe kidney. Note that the retroperitoneal incision was extended transperitoneally to reach the adhered right iliac artery and the bifurcated graft is passed craniocaudally behind the horseshoe kidney without dividing the isthmic tissue. CAU = caudal; CRA = cranial.
Preoperative Data of 127 Patients Who Underwent Elective Surgery for Abdominal Aortic Aneurysm between 1990 and 2004
AAA = abdominal aortic aneurysm; COPD = chronic obstructive pulmonary disease; Cr = creatinine; HSK = horseshoe kidney; NS = not significant.
A p value less than .05 is significant.
*Independent-samples t-test;
**Fisher exact test.
Table 1 depicts preoperative data regarding the patients with or without HSK. The mean age of the patients with HSK was 67.29 ± 2.43 years. Although preoperative serum creatinine levels were slightly higher than in patients with HSK (1.0 ± 0.08 vs 0.9 ± 0.12 mg/dL; p < .05), the perioperative renal failure rate was similar (Table 2). The mean aneurysm diameter in patients with HSK was 60.7 ± 5.3 mm (range 55–70 mm). A Dacron tube graft was used in four patients with HSK (57%) (18 mm in three patients and 20 mm in one patient), and bifurcated grafts were used in three patients (all 18/9 mm in size).
Perioperative Outcome of Surgery with a Left Retroperitoneal Approach in 127 Patients with Abdominal Aortic Aneurysm
AAA = abdominal aortic aneurysm; HSK = horseshoe kidney; ICU = intensive care unit; IV = intravenous; MI = myocardial infarction; NG = nasogastric; NS = nonsignificant; XCL = cross-clamp.
A p value less than .05 is significant.
*Independent-samples t-test;
**Fisher exact test.
Smoking was far more common in patients with HSK than those without (71.4% vs 22.5%; p < .05). Among all 127 patients in 14 years, 5 cases of in-hospital mortality were noted, none of whom belonged to the HSK group. The causes of death in these patients included mesenteric infarction and peritonitis (n = 1), cardiopulmonary failure following myocardial infarction (n = 2), and pulmonary failure with prolonged mechanical ventilation (n = 2). Patients with or without HSK were given similar amounts of intravenous fluid replacement (2,214.2 ± 441.3 vs 1,923.33 ± 433.6 mL/patient; p = .087) and allogeneic blood transfusion (0.71 ± 0.49 vs 0.9 ± 0.42 U/patient; p = .26) and had a similar ICU stay (see Table 2). Mechanical ventilation durations were higher in patients without HSK (10.06 ± 2.40 vs 7.43 ± 2.82; p < .05). Patients with HSK were noted to have slightly longer aortic clamp times (30.43 ± 3.55 vs 27.04 ± 3.92 minutes; p < .05).
Discussion
Although rare, AAA surgery associated with an HSK is among the technical challenges for aortic reconstruction. 2,9,10 Anatomic considerations regarding a bulky isthmus enwrapping the aneurysm, firm adhesions, location of the renal pelvis and the ureters, and anomalous arterial supply of the HSK commonly requiring an additional arterial reconstruction are all taken into account, usually before the surgical procedure. Aortography and a detailed analysis of a contrast-enhanced CT scan are invaluable. An extensive review of 19 patients with HSK in 31 years by O'Hara and colleagues revealed an 84% preprocedural diagnosis of HSK. 11 Their 16% mortality rate may appear to be very high in comparison with our results; nevertheless, their series included three emergent patients and cases of dialysis-dependent renal failure postoperatively. Abnormal preoperative renal function was associated with a significantly increased risk of mortality. In our seven patients, the mean preoperative serum creatinine level was 1.0 ± 0.08 mg/dL, which was lower than that reported by O'Hara and colleagues (1.5 mg/dL). 11 It is noteworthy that preoperative serum creatinine levels in our series were higher in patients with HSK; nevertheless, the perioperative renal failure rate was similar in both groups. CT has been reported to be the most accurate tool for diagnosis of HSK in advance. 12,13 Two patients in this series (28%) were operated on without knowledge of the HSK in advance, possibly owing to the limited availability of CT at the time. One of these two patients did have a very low-quality CT scan with suboptimal slicing, which barely showed the aneurysm but not the HSK.
The left retroperitoneal approach is the surgical incision of choice. 2,10,14 It provides adequate surgical exposure behind the HSK, enabling avoidance of division of the isthmus and trauma to isthmic branches at most times. Regarding the left retroperitoneal approach, special consideration is paid to aneurysmatic iliac arteries. In particular, right iliac artery involvement may be troublesome for the surgeon and may make the surgery considerably difficult. It is noteworthy that iliac involvement was present in two of the seven patients with HSK, and the repair with an aortobifemoral bifurcation graft was feasible in both patients. This issue is particularly of concern in the case of inflammatory aneurysms; in one of the latter two patients with HSK, the aneurysm was inflammatory and a transperitoneal extension was necessary (see Figure 3).
Various other strategies, such as the transperitoneal approach, 14 a midline abdominal incision with a right retroperitoneal approach, 15 and the endovascular approach, 5,16 have been reported. Endovascular therapy has become such a rapidly developing area that it has been used even in emergency settings. 17 It appears to be attractive for its minimal invasiveness and avoidance of many technical challenges of open surgery; however, it has drawbacks, such as a relatively high financial burden and the technical problems arising from anatomic considerations (eg, variable renal anatomy, neck calcification and angulations, diameters, peripheral occlusive disease). Additionally, sacrifice of lesser-sized anomalous renal arteries is of consideration. Exclusion of the aneurysm sac presumably excludes these arteries as well. Blockade of arteries larger than 3 mm in diameter was reported to be associated with an adverse renal outcome. 5
In this series, reimplantation of the renal arteries was applied in five of seven patients with HSK. We observed only one patient with a non–dialysis-dependent postoperative renal failure, which resolved in the postoperative period without persistent hypertension, an elevated serum creatinine level, or renal infarction on control CT scan. The artery of the HSK in this patient was reimplanted to the graft. Davidovic and colleagues reported on reconstruction of the renal artery in 10 of 13 patients with no graft occlusion, renovascular hypertension, or renal failure during an average of 5.3 years of follow-up. 18 As expected in this series, the amount of allogeneic transfusion and intravenous fluid replacement and the duration of ICU and hospital stay are similar to those of other 120 patients operated on for elective AAA. Significant findings on analysis of seven patients with HSK were the high smoking rate (71.4% vs 22.5%; p < .05) and the presence of hypertension among these patients (71.4% vs 35.8%), although they did not reach statistical significance in the latter.
In our series, topical cooling of the renal tissue or flushing of the isolated renal artery with cold saline solution was not used. Rapid anastomosis with reimplantation of the renal artery seems adequate for relatively short periods of renal ischemia. Lowering of the proximal aortic clamp along the graft after anastomosis of the anomalous renal artery may be used when a prolonged period of clamping time is anticipated.
An expected finding was higher mechanical ventilation times in the non-HSK group. This may be partly due to the fact that all mortal and morbid cases were dominant in the above-mentioned group of patients. In particular, five of all six cases with a perioperative respiratory distress were among patients without an HSK. Additionally, the number of patients with an HSK is thought to be too few to reach a conclusion. This has also been reflected as similar ICU and hospital stay duration in both groups.
Patients with AAA associated with HSK can be operated on with a left retroperitoneal approach without any significant increase in transfusion rate, volume replacement, or ICU and hospital stay in comparison with those without HSK. High preoperative creatinine levels may be predictive of a possible perioperative renal compromise; prompt reanastomosis of the anomalous renal artery is important for preserving renal function.
Routine postoperative follow-up with a CT scan is recommended unless reimplantation was performed. In the latter case, abdominal Doppler ultrasonography and/or CT angiography may be recommended. An additional angiogram may be required if visualization of the anastomosis and/or the anastomosed vessels is inadequate.