
Abstract
We describe a case of a 57-year-old woman with repeated acute arterial thrombosis of the femoral arteries following intravenous carboplatin-based combination chemotherapy for metastatic ovarian carcinoma. By extensive workup, no other known causes of arterial thrombosis were found. To our knowledge, this is the first case describing arterial thrombosis occurring as a complication of carboplatin therapy.
Case Report
A 57-year-old woman was admitted to our hospital with acute onset of pain in the left leg. Risk factors for atherosclerotic disease were absent. Her medical history revealed locally advanced ovarian carcinoma diagnosed 3 years earlier. She had been treated in another hospital by debulking and subsequently eight cycles of carboplatin and paclitaxel complicated by thrombosis of the inferior caval vein. Acenocoumarol was given for 6 months. Thereafter, she remained asymptomatic.
After 18 months, the patient was diagnosed with a recurrence of the ovarian carcinoma. A chemotherapeutic regimen of eight cycles of carboplatin and paclitaxel was given. During a stay in a foreign country, after completion of the regimen, she developed a painful, pale, and cold right foot with absent pedal pulses. An acute arterial thrombosis of the right femoral and popliteal artery was diagnosed. Thrombectomy was performed, and because of a compartment syndrome, immediate fasciotomy was done. Two days later, she developed similar complaints of her left foot and an occlusion of the left femoral artery was diagnosed. A left femoral thrombectomy was done. At this time, no workup was done to find an embolic source. Prophylactic subcutaneous low-molecular-weight heparin was given, and the patient was discharged from the hospital with palpable pedal pulses and no remaining complaints.
A year later, the second recurrence, stage IIIC ovarian carcinoma, was diagnosed and treated with a chemotherapeutic regimen of carboplatin and cyclophosphamide in our hospital. A computed tomographic scan showed metastasis in the spleen and spleen hilus. After the fourth cycle, the patient was admitted with pain in her left leg. A week earlier, the pain had started with a sudden cramp in her left leg during exercise, progressing to rest pain at the time of admission. Physical examination revealed a pale and cold left foot with absent popliteal and pedal pulses. Decreased sensibility was noticed, but motility was still present.
Angiography was performed, showing an occlusion at the bifurcation of the left common femoral artery (Figure 1). Perfusion was regained by catheter thrombectomy. Postoperatively, pedal pulses were present. Heparin was administered intravenously, and after a couple of days, low-molecular-weight heparin was restarted. Thereafter, the patient was analyzed for possible embologenic lesions by computed tomographic angiography (CTA), cardiac screening. and iliac and femoral ultrasonography, which did not reveal any embolic sources. No signs of arrhythmia were seen, and an echocardiogram of the heart failed to reveal the presence of an intracardial thrombus. Four weeks later, she developed an arterial thrombosis of the right leg, which was also treated by emergent thrombectomy. The same anticoagulant regimen was continued. Ten days thereafter, she again developed rest pain in the left leg, requiring thrombectomy. Again, a search for an embolic source was initiated, and this time, the CTA showed a floating thrombus in the aorta just caudal to the renal arteries that had not been present on the earlier CTA (Figure 2). At laparotomy, the thrombus was removed via a longitudinal aortotomy. A nonatherosclerotic aortic wall was seen, with no ulcers and no tumor infiltration. The para-aortic lymph nodes showed no macroscopic malignancy. A few days later, her left leg showed reocclusion, which required thrombectomy. A heparin-induced thrombocytopenic thrombosis was suspected but could not be confirmed hematologically: platelet counts had been normal, except a slight drop on one occasion (thrombocyte count: 108 to 87 × 109/L), which could be explained by previously given chemotherapy. A heparin antibody test was negative. Also, no skin lesions at heparin injection sites or acute systemic reactions after heparin bolus administration were seen. Nevertheless, in the absence of any other explanation for this dramatic clinical course, all heparin products were withheld and acenocoumarol therapy was started under temporary administration of danaparoid.
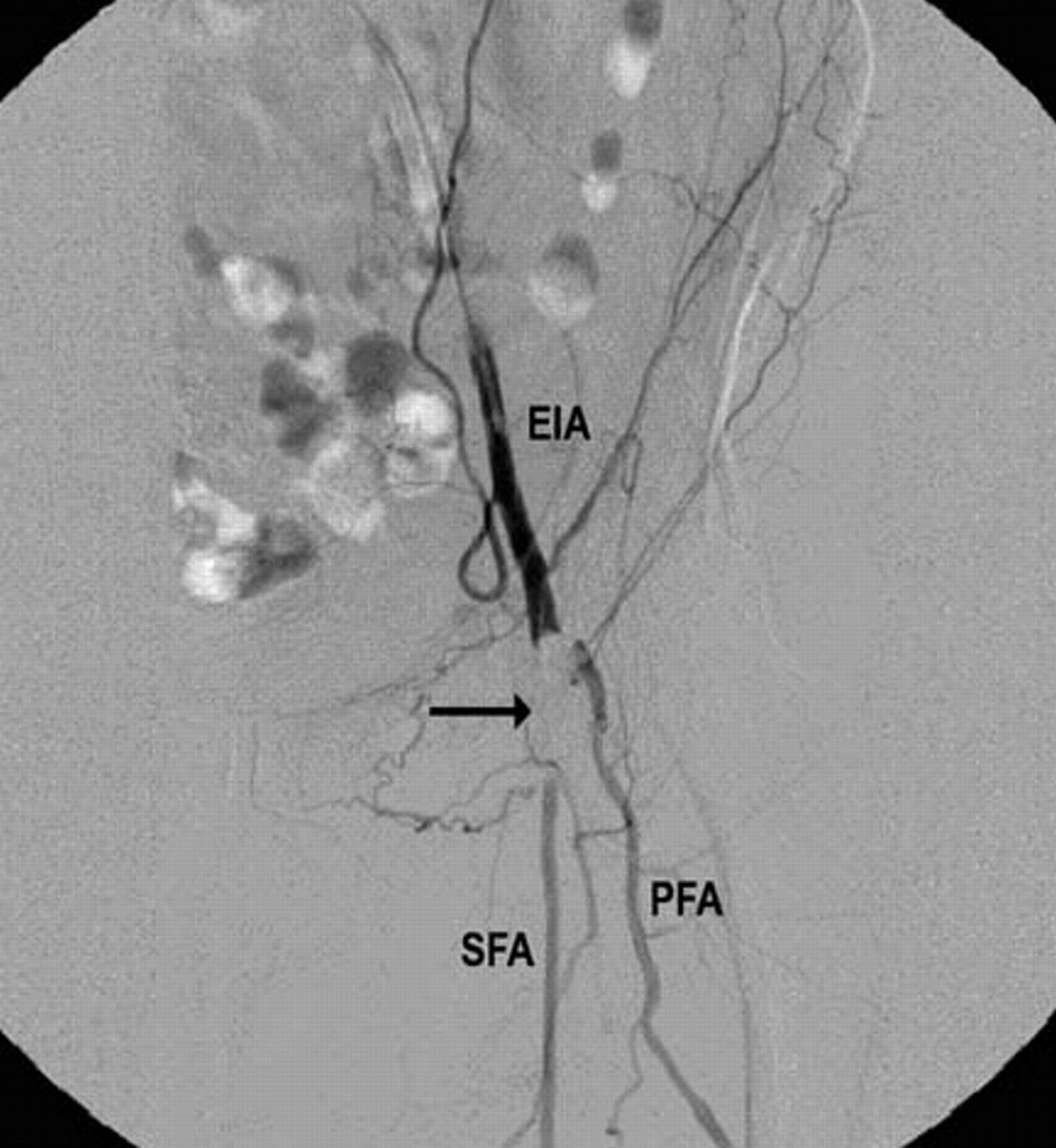
Angiogram demonstrating an occlusion (arrow) at the bifurcation of the left common femoral artery. EIA = external iliac artery; PFA = profunda femoral artery; SFA = superficial femoral artery.
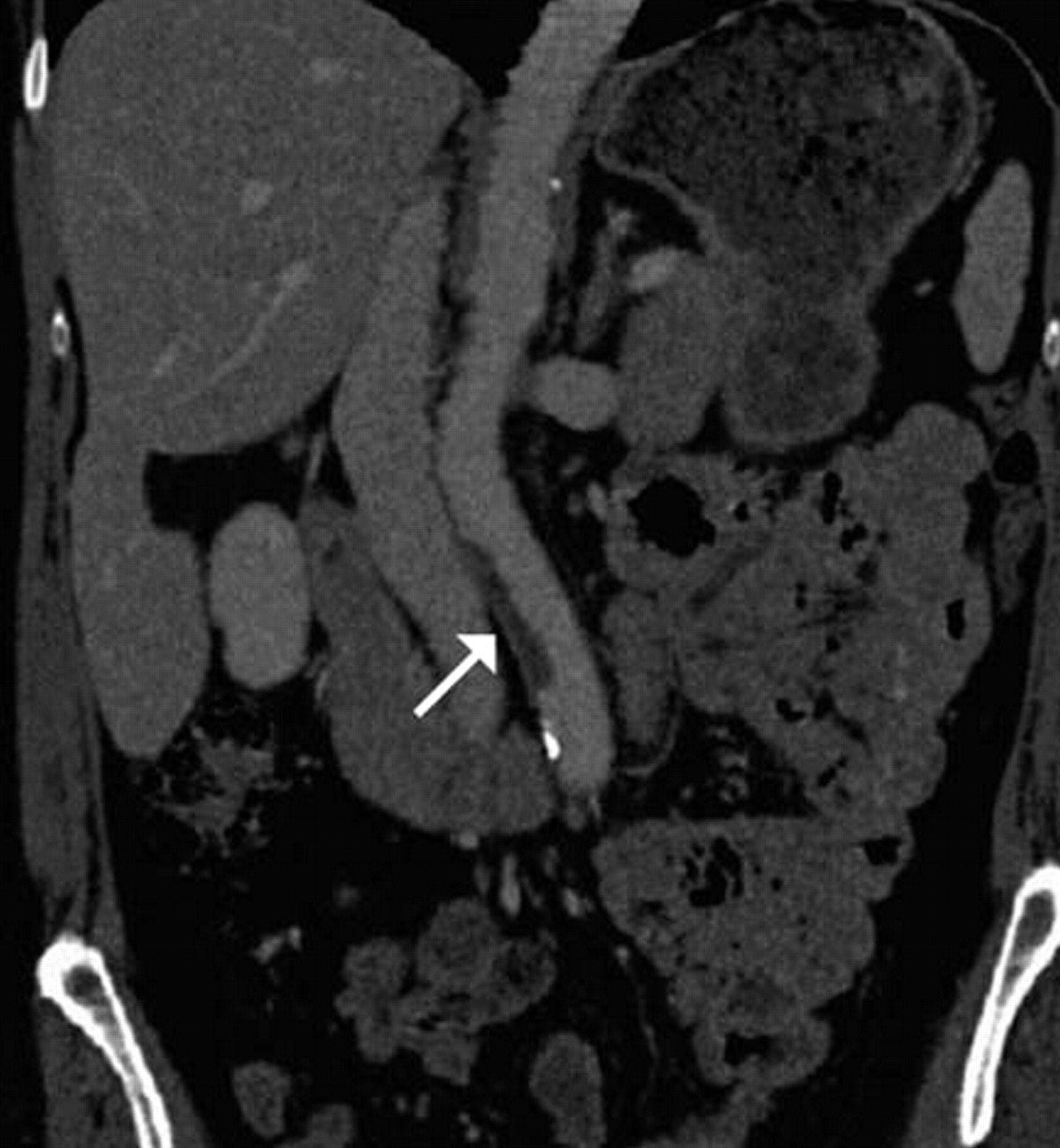
Computed tomographic angiogram showing a floating thrombus in the aorta caudal to the renal arteries (arrow).
After recovery of the surgical interventions, the chemotherapy regimen was continued by cyclophosphamide monotherapy. Subsequently, no adverse vascular events occurred during 1 year of follow-up. In addition to the described procedures above, the clinical course has been summarized in chronologic order in Figure 3.

The clinical course in chronologic order.
Discussion
Large-vessel arterial occlusions have been reported in a few case reports of patients with malignancy treated with cisplatin-based chemotherapeutic regimens, although this is a rare complicaton. 1–3 Carboplatin is an analogue of cisplatin that has been associated with less severe complications, such as thrombotic microangiopathy. 4,5 Also, pulmonary embolism and venous thrombosis have been reported. 6 Acute arterial thrombosis in the extremities caused by carboplatin-based chemotherapy has not been described in the literature. The time interval between the chemotherapy and the events on two different occasions strongly suggests a therapy-associated etiology.
The pathogenesis of the vascular complications in cancer patients receiving chemotherapy remains unclear. It is likely that a combination of mechanisms acts to promote vascular thrombosis, such as expression of procoagulant factors by tumor cells that can induce arterial thrombosis in the presence of stasis of blood. Direct tumor infiltration in the blood vessel can cause damage to the vascular wall, inducing thrombosis. Another mechanism includes increased platelet reactivity caused by tumor-platelet interaction followed by hypercoagulability. Furthermore, endothelial cells may show interaction with tumor cells, leading to a hypercoagulable state caused by triggering of inflammatory cytokines en procoagulentia. 7,8
Factor VIII (von Willebrand's factor), which increases platelet activation by altered endothelial cell integrity, is elevated in patients with arterial occlusive complications followed by cisplatin-based chemotherapy. The precise pathophysiologic basis for this relationship is not yet known. 9
Chemotherapy could induce an increase in plasma fibrinopeptide A levels. This suggests that patients receiving chemotherapy express thrombin-like activity in plasma and, therefore, may be at risk of developing clinically significant intravascular activation of coagulation. 10 In addition, the patient's poor physical status and decreased cell activity undoubtedly have a role in increasing the risk of thromboembolic events. 11
A combination of such mechanisms could cause vascular spasm, with subsequent thrombosis leading to vessel occlusions. It remains unclear which substance is responsible for the occlusive complications. Earlier signs of this rare vascular complication caused by carboplatin-based chemotherapy should be recognized and another chemotherapeutic regimen should be considered to avoid repeated arterial occlusions with severe consequences for the patient. Others have suggested that all patients undergoing cancer treatment should receive thromboprophylaxis with low-molecular-weight heparin. 12
In conclusion, carboplatin therapy may be associated with the occurrence of intra-arterial thrombosis. Future clinical trials with carboplatin should collect prospective information on the risk of vascular events.