
Abstract
Studies on hyperhomocysteinemia in vascular occlusive disease have included mostly patients with arterial occlusion. However, more recent studies have included cases of venous occlusive disease as well. Our present study is aimed at comparing the prevalence of hyperhomocysteinemia in venous occlusive disease vis-è-vis arterial occlusive disease in the North Indian urban population. Homocysteine was estimated by chemiluminescent immunoassay in 205 normal controls and 536 patients, 244 presenting with arterial occlusion and 292 with venous thrombotic disease. The mean homocysteine in patients with arterial occlusion was 21.79 ± 0.09 μmol/L (mean ± standard error of measurement), in patients with venous thrombosis was 25.53 ± 0.1 μmol/L, and in controls was 11.33 ± 0.18 μmol/L. The prevalence of hyperhomocysteinemia (> 15 μmol/L) was 56.38% in arterial occlusive disease and 54.64% in venous thrombosis. In patients with peripheral vascular occlusive disease, patients with deep venous thrombosis (DVT) had the highest mean homocysteine level (25.51 μmol/L), which was even higher (32.14 μmol/L) when associated with pulmonary embolism (PE). There is a high prevalence of hyperhomocysteinemia in arterial and venous occlusive disease. Hence, in all patients with vascular occlusive disease, hyperhomocysteinemia should be elucidated and treated. In addition, long-term follow-up is required to ascertain whether the reduction in homocysteine decreases the thrombotic events and whether homocysteine levels can actually be of prognostic or predictive value in cases of DVT with PE.
Vascular pathology is heralded by an altered vascular endothelium or vessel wall. Hence, any factor contributing to such an alteration would become a risk factor for vascular disease. One such substance is homocysteine (Table 1). 1–4
Etiology of Vascular Thrombosis
Lp = lipoprotein.
Homocysteine is a small, sulfur-containing amino acid derived primarily from the breakdown of dietary methionine in the activated methylation cycle. 5,6 This homocysteine either reenters the cycle to form methionine or gets transsulfurated to form cysteine. The methylation cycle has three limiting factors-methylenetetrahydrofolate reductase (MTHFR), folic acid, and vitamin B12-whereas the transsulfuration reaction is dependent on cystathionine-β-synthase (CBS) and pyridoxine. Deficiency in any of these vitamins or defects in the genes of either of these enzymes will reduce the rate of metabolism of homocysteine and cause an increase in its plasma level. 5,6 The defects in the MTHFR and CBS genes can lead to either reduced synthesis of the enzymes or even synthesis of defective enzymes. The most commonly occurring polymorphisms are enumerated in Figure 1. Hyperhomocysteinemia is modifiable by administration of the B group vitamins, irrespective of its cause. 7
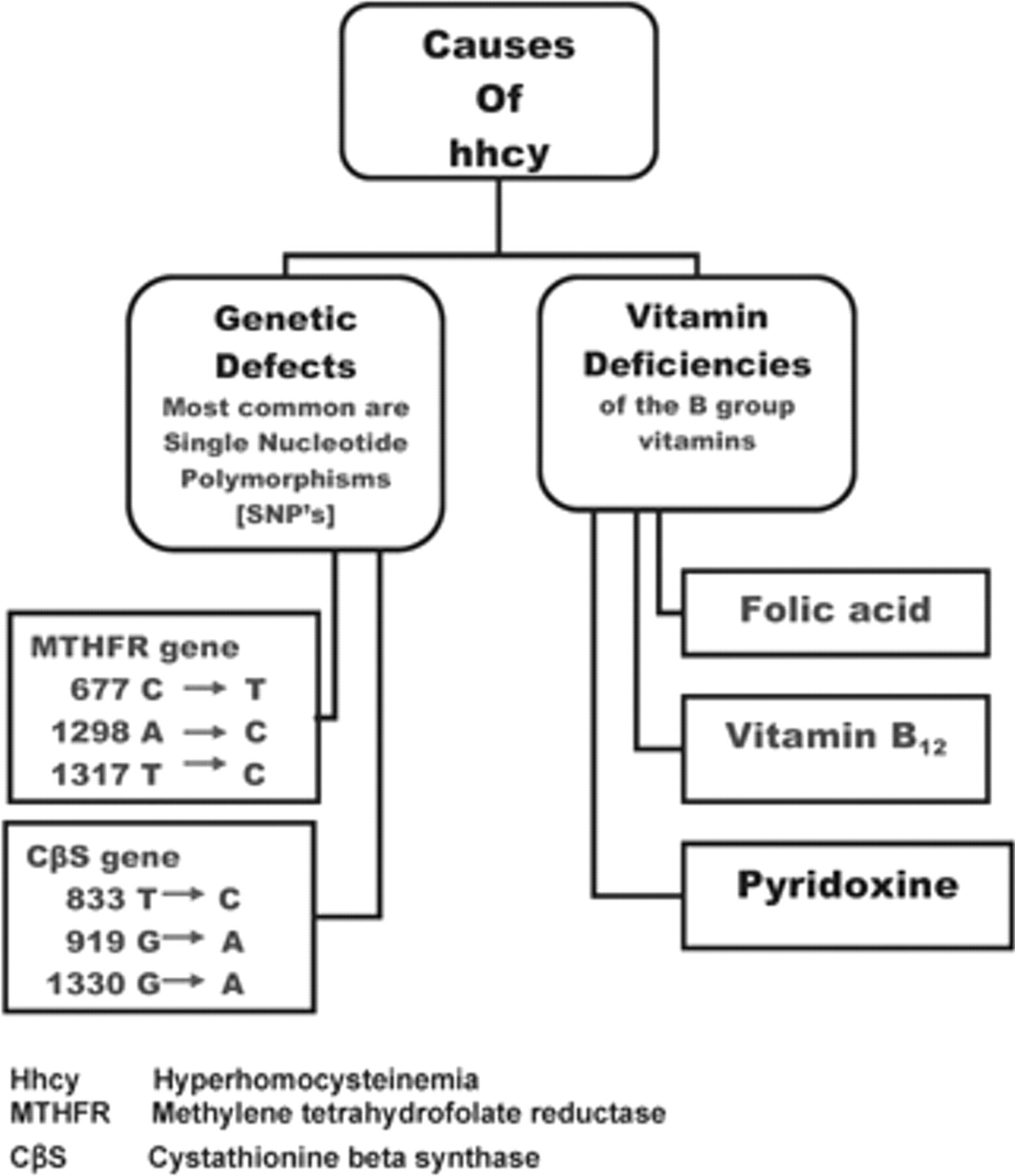
Causes of hyperhomocysteinemia (hhcy). CβS = cystathionine-β-synthase; MTHFR = methylenetetrahydrofolate reductase.
Homocysteine has many pathogenic properties. 8 Most significant among these is its oxidant properties by virtue of the sulfur atom it contains. 9 In the healthy state, this oxidizing ability is countered by the naturally occurring (proteins and enzymes) and dietary antioxidants in the body. When this dynamic balance is altered, deleterious oxidative effects result.
In 1968, McCully discovered that hyperhomocysteinemia was the pathogenic factor in premature atherosclerosis in cases of homocysteinuria with mental retardation in children. 10 Ever since, it has been implicated as a risk factor in vascular disease predisposing patients to atherosclerotic and thrombotic plaque formation by platelet function abnormalities in arteries and through abnormalities of coagulation in veins. 8
Worldwide data have elucidated the biologic reference interval (BRI) of plasma homocysteine as 5 to 15 μmol/L, with a mean of 10 μmol/L in various global populations. 11,12
Studies on hyperhomocysteinemia in vascular disease have included mostly patients with arterial occlusion. 13–15 However, more recent studies have included cases of venous disease as well. 16–18 Our present study was aimed at comparing the prevalence of hyperhomocysteinemia in venous thromboembolism vis-è-vis arterial occlusive disease in the North Indian urban population and assessing the response to vitamins of the B group.
Methods
Among the patients with vascular disease coming to our hospital for treatment, 536 patients were randomly selected. Of these, 244 presented with arterial occlusion and 292 with venous thromboembolism. Diagnosis was based on angiography and/or duplex scanning. The 205 normal controls selected were healthy individuals without any complaints, history, or family history of vascular disease. The plasma homocysteine level of all subjects was estimated by chemiluminescent immunoassay, which involves antigen-antibody complex formation followed by an enzymatic reaction, with the final chemiluminescent product being measured on the Immulite (marketed by Diagnostic Products Corporation, Los Angeles, CA). 19
To assess the effect of different types of vitamin therapy on homocysteine levels, 29 patients receiving either different combinations of vitamins of the B group or no vitamin supplements were subjected to repeat estimations of plasma homocysteine when they attended their follow-up clinics.
Statistical analysis was done by applying analysis of variance and t-test.
Results
The mean homocysteine level in the controls (age 18–75 years) was 11.33 ± 0.18 μmol/L (mean ± standard error of measurement), which is significantly higher than the worldwide mean of 10.0 μmol/L. 2 The mean homocysteine level in patients with arterial occlusion was 21.79 ± 0.09 μmol/L and that in patients with venous thromboembolic phenomena was 25.53 ± 0.10 μmol/L, both significantly higher (p < .0001) than the corresponding values in the controls (Table 2) but not significantly different from each other (p = .9252).
Mean Homocysteine and Prevalence of Hyperhomocysteine in Occlusive Vascular Disease
hcy = homocysteine; SEM = standard error of measurement.
Among the cases of peripheral vascular disease, the highest value of mean homocysteine (25.51 μmol/L) was seen in cases of deep venous thrombosis (DVT), the values being even higher (32.14 μmol/L) when such cases were complicated with pulmonary embolism (PE). The lowest values (within the BRI) were observed in postpartum patients, with even lower values in those who presented with DVT subsequent to recurrent abortion (Figure 2).

Mean homocysteine (in μmol/L) in different types of peripheral vascular disease (in ascending order of mean homocysteine). AT = arterial thrombosis; DVT = deep venous thrombosis; MVT = mesentric vein thrombosis; PE = pulmonary embolism; PP = postpartum; RA = recurrent abortion.
The prevalence of hyperhomocysteinemia in patients with arterial and venous occlusive disease was 56.38% and 54.64%, respectively (see Table 2). The prevalence of homocysteine > 11.33 μmol/L (our population's mean homocysteine level) was 79.09% in cases of arterial occlusion and 76.07% in venous thrombosis.
The 29 patients who attended follow-up were grouped into three categories: patients not receiving any vitamin supplements, patients receiving a single daily dose of 5 mg folic acid, and patients receiving varying combinations of vitamins B12 and B6. The decrease in homocysteine levels per month of treatment in these groups was 1.5%, 13.2%, and 9.8%, respectively (Figure 3).

Percent decrease in homocysteine (hcy)/month (mth) of treatment with different vitamin preparations.
Discussion
In the past decade and a half, there has been an exponential increase in the studies pertaining to homocysteine and its various implications, most prominent among them being its effect on vessel walls.
Given that the maximum pathogenicity of homocysteine is in the vascular endothelium, it should follow that arteries and veins would both be affected. Yet it was observed that the majority of studies were conducted in patients with arterial occlusion exclusively, 13–15 and only a few recent studies have been conducted in venous occlusive disease cases as well. 16–18 Given that none of these were conducted in the Indian population, it was deemed necessary to ascertain the mean homocysteine level and the prevalence of hyperhomocysteinemia in cases of venous thromboembolism vis-è-vis arterial occlusion in a North Indian urban population. At the same time, their response to vitamins of the B group was assessed in terms of the rate of reduction in homocysteine.
Given that the prevalence of hyperhomocysteinemia in both categories of patients is similar and that the mean homocysteine levels in these two groups are not significantly different from each other (see Table 2), it follows that both arteries and veins are equally susceptible to the pathogenicity of hyperhomocysteinemia.
It has been elucidated that hyperhomocysteinemia does not have a threshold for pathogenicity, 7 meaning that even within the BRI, pathogenicity increases as homocysteine levels increase. Therefore, it has been suggested that the patients with a homocysteine level greater than the population mean should be targeted and treated for hyperhomocysteinemia. Toward this end, we further categorized the patients into those with a homocysteine level more than or less than 11.33 μmol/L. This yielded a percent prevalence of homocysteine > 11.33 μmol/L of 79.09% in arterial occlusion and 76.07% in venous thrombosis.
Given that the mean homocysteine level was significantly higher (p < .01) in the presence of PE than in its absence in patients with DVT and that PE is potentially fatal, it might follow that homocysteine has a prognostic or predictive role to play in these cases. However, further studies would be required to substantiate this preliminary observation.
As is shown in Figure 2, in patients with postpartum DVT and DVT associated with recurrent abortion, the mean homocysteine level was the lowest; in fact, it was within the BRI of 5 to 15 μmol/L. It can be postulated that during pregnancy, all subjects are administered daily supplements of folic acid; hence, homocysteine stays within the BRI, but it becomes necessary to ascertain the mean homocysteine level in normal pregnancies before any conclusion can be reached on this front.
There have been variable reports about the efficacy of the B vitamins in reducing levels of homocysteine 7,18 ; hence, some of the patients who came for follow-up were also subjected to repeat homocysteine estimations. Given that they came to us at varying intervals after institution of treatment, their response to B vitamins was assessed in terms of the rate of reduction in homocysteine, that is, the percent decrease in homocysteine per month of treatment. Figure 3 shows clearly that a single daily dose of folic acid yields the maximum reduction in homocysteine-13.2% per month. In one case of DVT (a 35-year-old male), when a multivitamin containing 1.5 mg of vitamin B12 and 1 μg of vitamin B6 was replaced with a single daily dose of 5 mg of folic acid, the rate of decrease in homocysteine increased from 5.2 to 9.2%.
Conclusions
The salient positive findings of this study can be stated as follows:
The prevalence of hyperhomocysteinemia in arterial occlusion and venous thrombosis is comparable.
The mean homocysteine level in both of these groups of patients is similar, in addition to being significantly higher than the mean homocysteine level in the controls.
Patients with peripheral vascular occlusive disease were segregated as per their diagnoses, and among these, the highest mean homocysteine level was observed in patients with DVT, especially so when there was concomitant PE as well.
The most effective means of lowering homocysteine is, possibly, a single daily dose of 5 mg of folic acid.
Thus, in conclusion, it may be said that homocysteine is a modifiable risk factor for vascular occlusive disease, whether it is arterial or venous, and that the most effective means of reducing homocysteine is, possibly, a single daily dose of folic acid.
In addition, long-term follow-up is required to ascertain
Whether folic acid is, indeed, the most effective homocysteine-lowering vitamin (our preliminary follow-up had very few subjects)
Whether reducing homocysteine results in a reduction in thrombotic events
Whether the apparently increased level of hyperhomocysteinemia associated with PE in cases of DVT actually has a predictive or prognostic role in DVT for the occurrence of PE
Footnotes
Presented in part at the XIIIth Annual National Conference of Vascular Society of India (VSICON 2006), New Delhi, India, November 3–5, 2006.