
Abstract
Management of arteriovenous malformation (AVM) remains a major challenge to vascular surgeons. A multidisciplinary approach was introduced in our hospital to manage these cases from October 2003 to date. This is a report of our experience in their management. A prospective study was done on all patients with symptomatic AVM admitted to our unit between October 2003 and May 2006. All patients had preoperative duplex scanning and magnetic resonance imaging with or without conventional angiography. A multidisciplinary team assessed and treated these cases according to the type of malformation. Thirty-two cases were included in this study, with a mean follow-up of 18.3 months. Of these, 20 cases were predominantly venous and treated with surgical excision (n = 14) or ethanol sclerotherapy (n = 6). Twelve cases were predominantly arterial or arteriovenous shunting; 10 were treated with preoperative embolization followed by surgical excision and the remaining 2 with superselective embolization alone. The overall complication rate was high (31%). However, all were minor and settled down conservatively. No recurrence was observed in the early follow-up period. Management of AVM by a surgical and endovascular approach can deliver excellent results, with acceptable morbidity and no recurrence in the early follow-up period.
Management of arteriovenous malformation (AVM) remains a major challenge to vascular surgeons. Over the last two decades, there have been revolutions in its investigations and treatment. The poor results from proximal ligation of the feeding vessel 1 have been improved after introduction of superselective catheterization and embolization. 2 The standard surgical excision of venous malformation used in the past has been replaced partly with sclerotherapy, with favorable results. 3 The ill-planned management strategy has been replaced by a multidisciplinary approach. 4 A new classification (Hamburg classification) 5 has emerged and has become the basis for diagnosis and management. The multidisciplinary management approach was introduced in our hospital to manage these cases from October 2003; this is a report of our experience.
Patients and Methods
A prospective study was performed on all patients with symptomatic AVM admitted to the vascular unit, King Fahd Hospital of the University, Saudi Arabia, between October 2003 and May 2006. A full clinical history and physical examination were done. Each symptom and sign, for example, pain, discomfort, and limited mobility, was reported. All patients had preoperative duplex scanning to assess hemodynamics, feeding arteries, the type of malformation, and its draining veins. Magnetic resonance imaging (MRI) was performed to confirm the diagnosis and to assess the extent of the lesion, tissue involvement, and any concomitant lesions. Slow-flow venous malformations have high signal intensity on T2-weighted MRIs, whereas high-flow arterial AVMs and fistulae contain a signal void. 6 Computed tomography was used in some cases to rule out skeletal involvement. After a thorough examination and investigation, AVM was classified according to the Hamburg classification 5 into (a) predominantly arterial, (b) predominantly venous, (c) predominantly arteriovenous (AV) shunting, (d) combined vascular, or (e) predominantly lymphatic. If the diagnosis was predominantly arterial or AV shunting AVM, angiography was performed to define the vascular anatomy and proceed to embolization if required. AVM was also staged according to the modified Schobinger classification 7 into four stages: I, cutaneous blush (quiescence); II, enlargement, pulsation (expansion); III, persistent pain, ulceration, or bleeding (destruction); and IV, cardiac failure (decompensation).
A multidisciplinary team assessed and treated these cases according to type and stage. No treatment was required for stages I and II unless serious problems were anticipated, for example, AVM near the eye or in the tongue or a rapidly expanding lesion. Indications for urgent intervention were stages III and IV of the modified Schobinger classification. Selection of intervention, either surgery, embolization, or combined (embolization before surgery), depended on the type, location, and extent of the lesions. Anticipation of postintervention morbidity was always considered.
For venous AVM, surgery alone was preferred in an easily accessible lesion with an acceptable risk of resection; otherwise, percutaneous ethanol sclerotherapy was used. Injection of the sclerotherapy was performed under general anesthesia to prevent pain and patient movement during the procedure. Occlusion of the venous flow was done by the use of a rubber band or tourniquet. Direct puncture of the venous malformation was performed with a Teflon-sheathed needle, and free flow of blood was obtained. If the malformation was deep, contrast medium was injected, and the malformation was visualized followed by an injection of 95% ethanol under fluoroscopic monitoring. The volume of ethanol injected was based on the size and location of the malformation and the patient's weight. On withdrawal of the needle, compression was maintained for 5 minutes to fix the ethanol in the vein wall and to prevent bleeding. All patients received intravenous dexamethasone (0.1 mg/kg) immediately before the procedure and continued every 8 hours for 3 days postoperatively to control the inflammation. This was gradually tapered off over the following 5 days.
If the lesion was a predominantly arterial or AV shunting and was surgically accessible, a combined approach was performed with preoperative embolization of the AV communication followed by surgical excision. Embolization would decrease the blood loss during surgical resection. If the lesion was diffuse or disability was anticipated after surgical intervention, superselective embolization alone was performed.
Angiography and embolization were carried out in the angiography suite using Polystar (Siemens, Erlangen, Germany). All patients underwent diagnostic angiography that disclosed the AVM and feeding artery. Images were reviewed by both the radiologist and the vascular surgeon. Following superselective catheterization of the feeding artery of the AVM, the position of the tip within the artery was ascertained with new images before embolization. In most of our cases, glue was used as the embolizing agent. In these cases, a 1:1 mixture of Histoacryl glue (n-butyl cyanoacrylate [NBCA]) as an embolic material and Lipiodol (Guerbet, Aulnay-Sous-Bois, France) as a contrast material was injected under fluoroscopy. Fast withdrawal of the catheter after injection was carried out to avoid its adhesion within the vessel wall. In cases of long feeding vessels with multiple collaterals, embolization was performed by microcoils (3–12 mm; Cook McReye, William Cook, Bjaeverskov, Denmark). Postembolization angiography was performed to ensure proper occlusion of the main feeding vessel to the AVM. In some patients, the pulsation persisted in the swelling owing to multiple feeding vessels and underwent more than one session of embolization. In cases that had surgical resection, local tissue was used for closure whenever possible. If the defect was large, a split-thickness skin graft or pedicle flaps were used.
Postoperative success was determined by subjective improvement of symptoms along with objective evidence of improved clinical signs, including a reduction in the lesion size and improved range of movement. All postintervention complications were recorded.
Follow-up consisted of a history and clinical examination. For patients in whom recurrent symptoms warranted intervention, repeat MRI with or without angiography was performed. In patients who remained asymptomatic, no further investigation was required.
Results
Thirty-two cases were included in this study: 18 females and 14 males, with a median age (± SD) of 18.8 (± 8.4) years. Six cases were stage II and 26 cases were stage III. Indications of intervention were severe pain (21), ulceration and bleeding (5), expanding swelling (4), and big tongue lesions (2). The majority (13 cases) of the lesions were in the head and neck (Figures 1 to 3), followed by the upper extremity (9 cases; Figure 4), the lower extremity (7 cases), and the back (2 cases; Figure 5) and only one case in the abdominal wall (Figure 6).
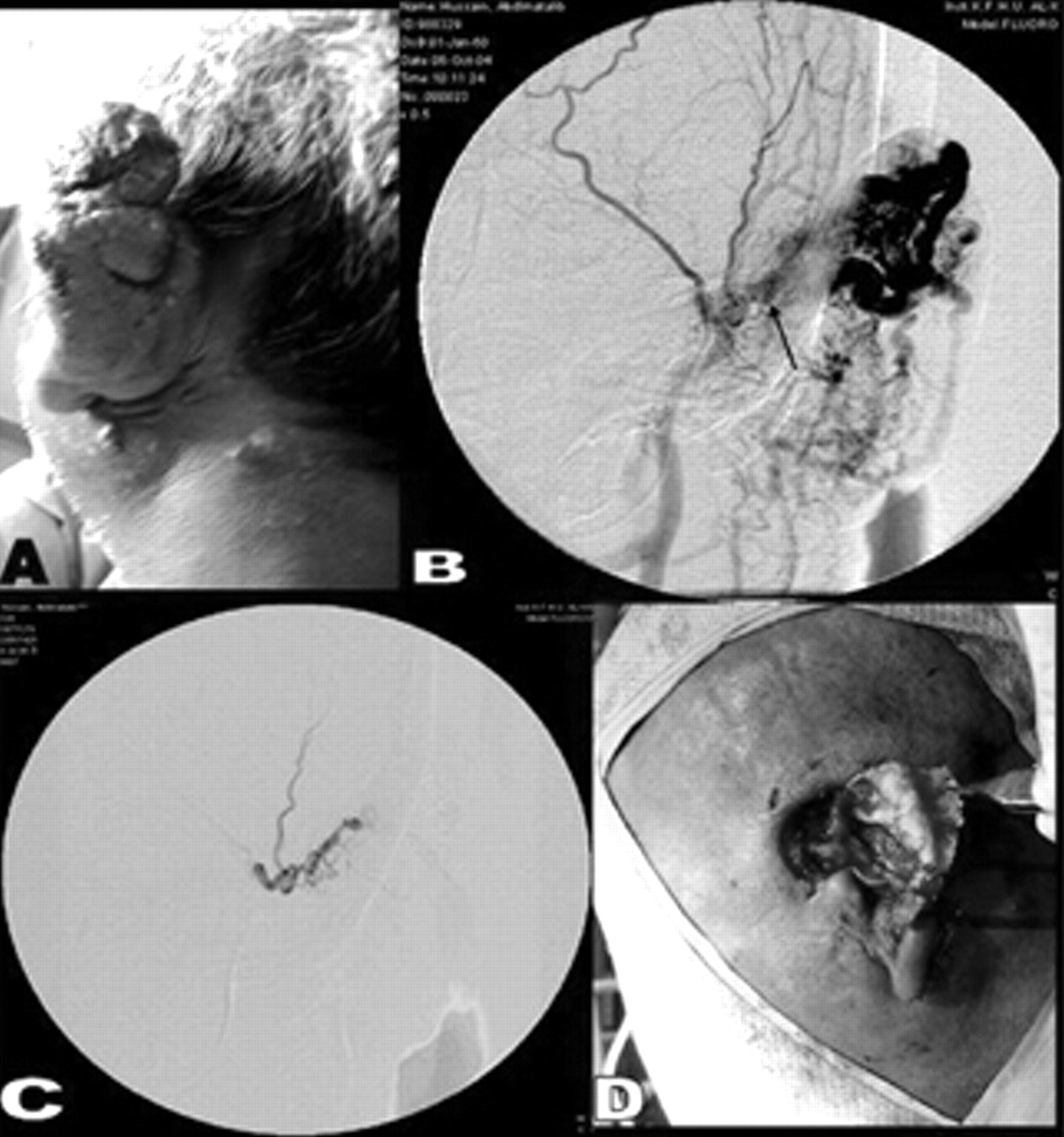
A, Photograph of a 35-year-old man with a left ear arteriovenous malformation (AVM). B, Selective external carotid artery angiogram showing the AVM supplied by branches of the superficial temporal artery (arrow). C, Superselective embolization of the feeding artery with glue. D, Postsurgical excision of the AVM leaving the cartilage intact.
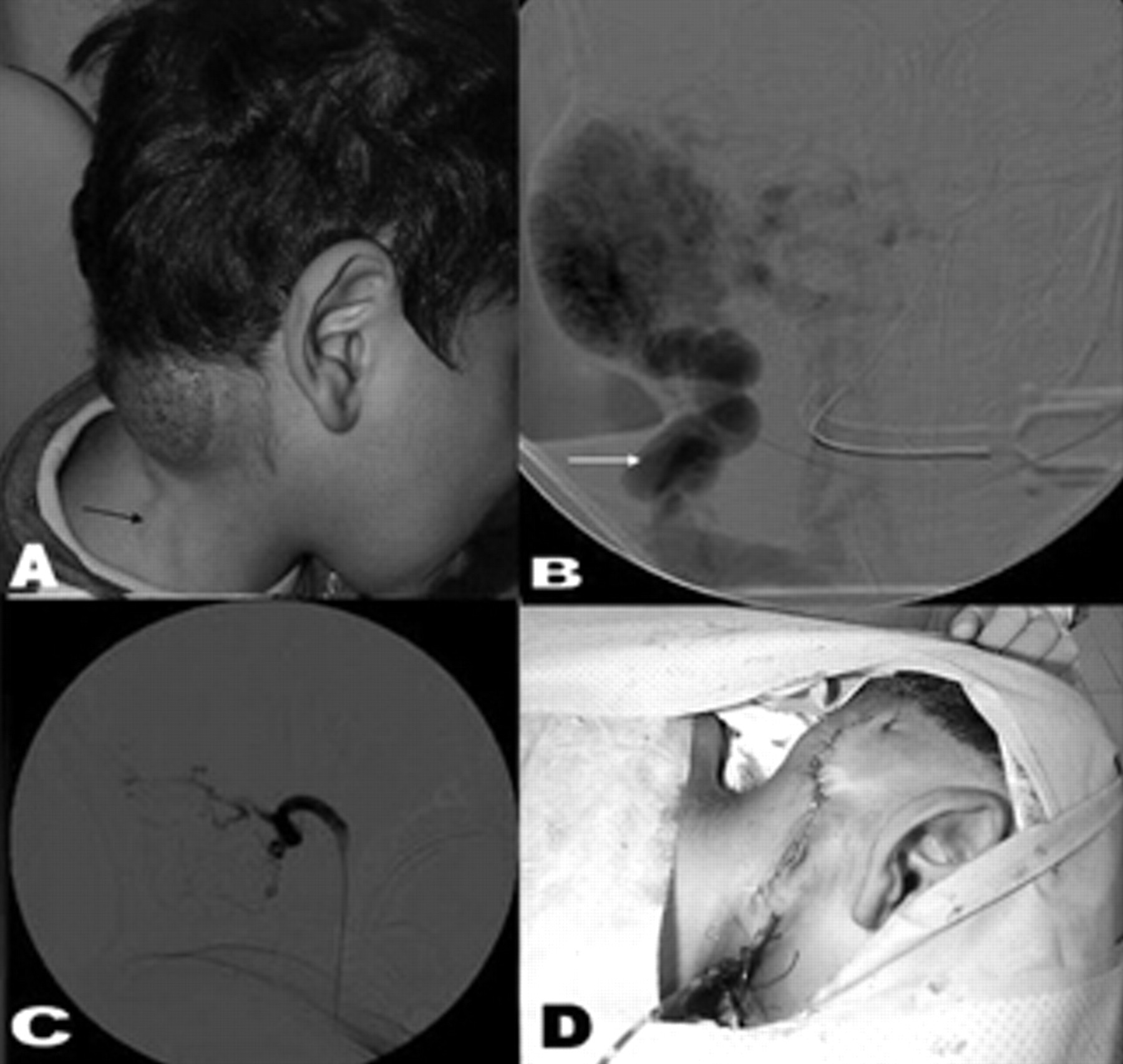
A, Picture of a 5-year-old boy with a right occipital arteriovenous malformation (AVM) with a dilated draining vein (arrow). B, Selective external carotid angiogram showing the AVM (predominantly arteriovenous shunting) supplied by branches of the occipital artery with a dilated draining vein (arrow). C, Superselective embolization of the feeding artery with glue. D, Postsurgical excision picture of the AVM.
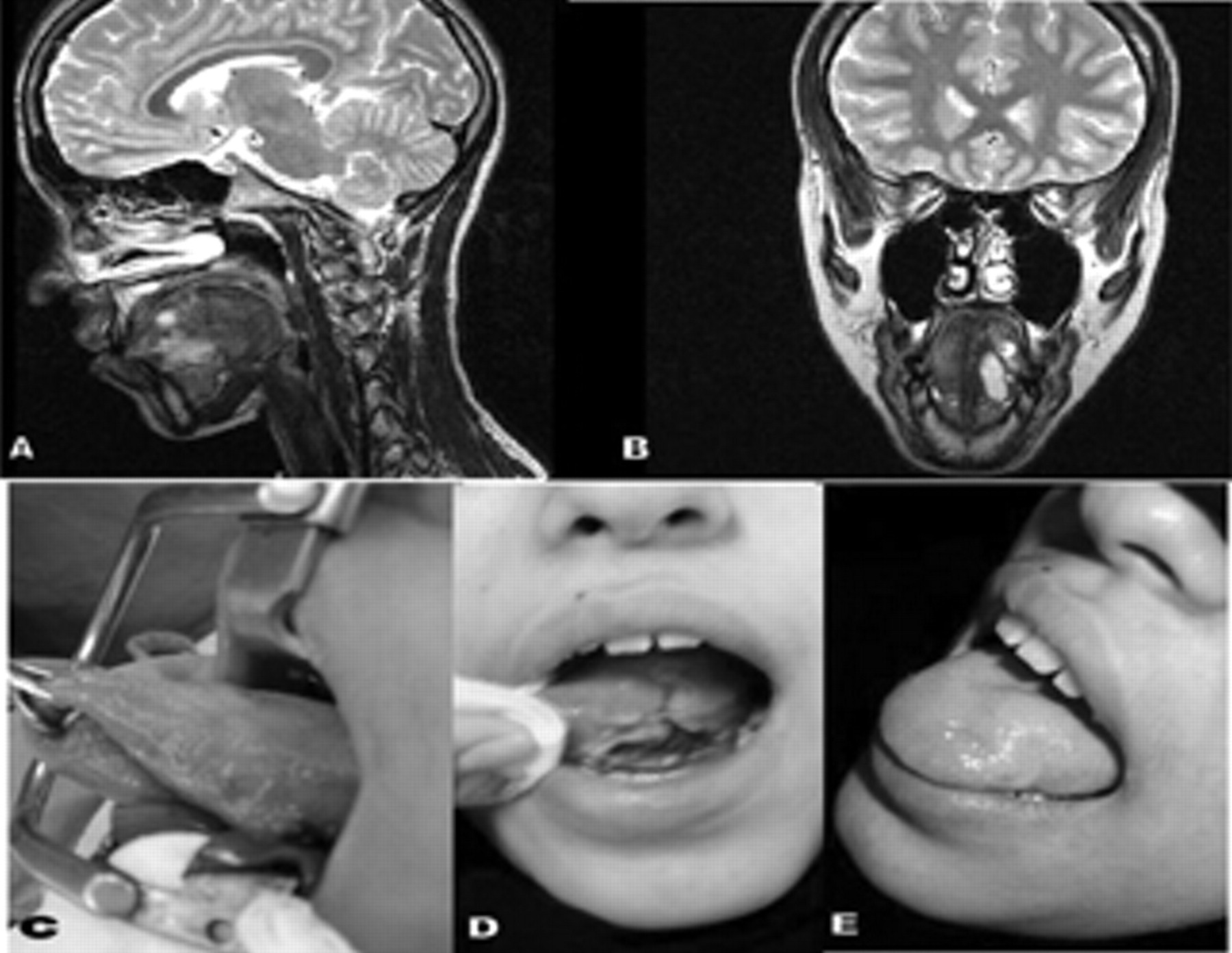
A and B, Sagittal and coronal T2-weighted magnetic resonance image of the tongue showing a high signal intensity area at the left hemitongue extending to the floor of the mouth, with no signal void. C, Picture of the tongue before alcohol injection showing the venous arteriovenous malformation (AVM) on the left side. D, Postinjection (fifth day) showing sloughing at the site of the AVM. E, Postinjection (4 weeks) showing complete healing of the tongue.

A, Axial computed tomographic scan showing cortical erosions of the right humerus neck by an overlying arteriovenous malformation (AVM). B, Sagittal T2-weighted magnetic resonance image of the right shoulder showing a superficial and deep high-flow AVM. C, Right axillary angiogram showing the AVM with multiple feeding arteries from the circumflex brachii and profunda brachii arteries. D, Superselective embolization of the circumflex brachii artery with glue.

A, Picture of a 32-year-old woman with an arteriovenous malformation (AVM) in the right upper scapular area and a scar from the previous attempt at surgical removal. B, Selective angiogram of the right thyrocervical trunk artery showing the feeding arteries of the AVM (predominantly arterial). C, Postembolization subclavian digital subtraction angiography showing complete occlusion of the feeding artery (arrow) with glue. D, After surgical excision of the AVM.
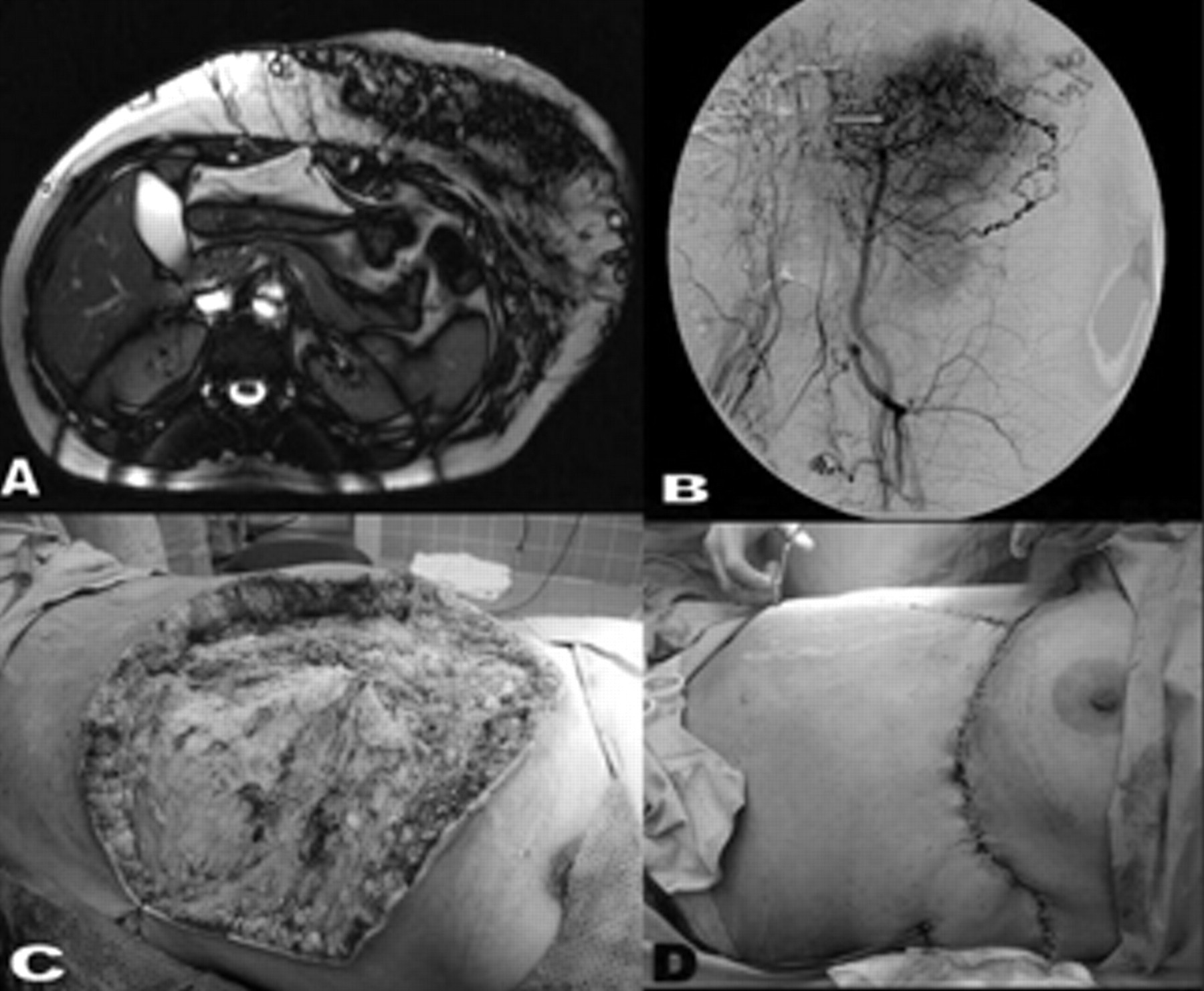
Axial T2-weighted magnetic resonance image of the upper abdomen showing a large mixed signal intensity of a left upper abdominal wall arteriovenous malformation with no intra-abdominal extension. B, Delayed aortogram after embolization of the left inferior epigastric artery using coil (arrow). C, Picture of the abdominal wall after surgical excision. D, Abdominal wall after plastic reconstruction with a local flap.
Twelve cases were either predominantly AV shunting (nine) or predominantly arterial (three). Four of these cases had attempted surgical excision in other hospitals. In all of these four cases, no preoperative embolization was performed, and severe bleeding developed at the start of surgical resection. Ten were treated with preoperative embolization followed by surgical excision within 3 to 5 days (see Figures 1, 2, 5, and 6). It was noticed that blood loss during resection was minimal. Two were diffuse, with bony involvement, and were treated with superselective embolization alone (see Figure 4). The arteries embolized are listed in Table 1. A mean of 1.75 embolization procedures was required (range 1–3). In all cases, the size decreased dramatically after embolization, and pain in the lesion persisted for 1 to 3 days. In the cases treated with embolization alone, the patients' symptoms disappeared completely after 4 to 5 days. Adjunctive plastic reconstruction was required in five cases (see Figure 6). Histopathologic examinations of the excised lesions confirmed the diagnosis (Figure 7) in each.

Photomicrograph of the lesion in Figure 5: multiple intercommunicating vascular channels; some are of the small thin wall and others are of the large thick wall type. The vascular channels are interspaced by fibrofatty stroma (hematoxylin-eosin stain; ×100 original magnification).
Arteries Embolized in Arteriovenous Malformation Cases (n = 12)
NBCA = n-butyl cyanoacrylate.
Twenty cases were predominantly venous; 14 were treated with surgical excision and 6 with ethanol sclerotherapy (Table 2 and Figure 3).
Management of Venous Malformations (n = 20)
The complication rate was 31%. However, all incidents were minor and mostly limited to skin and subcutaneous tissue. Five patients had wound infection, four developed sloughing and ulceration (see Figure 3), and one patient was complicated with temporary ulnar nerve neuropathy. All cutaneous complications settled down by débridement and dressing (see Figure 3). At the end, the cosmetic results were good, and all patients expressed satisfaction.
Over a mean follow-up period of 18.3 months (range 2–30 months), 31 (97%) patients remained asymptomatic. One patient developed mild pain in the shoulder 14 months after superselective embolization alone. MRI was performed and showed no evidence of recurrence.
Discussion
Until recently, the histologic terminology of vascular anomalies was confusing. In 1982, vascular anomalies were divided according to cellular kinetic into two types: lesions owing to endothelial hyperplasia (tumors) and lesions that arise by dysmorphogenesis and exhibit normal endothelial turnover (malformation). 8 These malformations are the result of faulty development of the blood vessels with multiple connections between arteries and veins. In the present study, all cases that had surgical resection showed such multiple dilated intercommunicating vascular channels. In 1988, a new classification was published based on the International Society for the Study of Vascular Anomalies (ISSVA) consensus during the Hamburg workshop. 5 We used this classification in the present study and found it helpful in planning further management of such cases, especially endovascular treatment. In 1990, AVMs were also categorized according to the Schobinger clinical staging system introduced at the ISSVA meeting in Amsterdam. 7 This categorization has therapeutic implications with regard to the indication and urgency of intervention.
Although the history and clinical examination can diagnose most cases of AVM, duplex ultrasonography 9,10 is very important to confirm the diagnosis and provide information about blood flow, the feeding artery, and the draining vein. However, it has a limited role in the assessment of deep lesions and lesions adjacent to air or bone. MRI 11 is the most valuable imaging modality in classification of AVM. It depicts the anatomic relationship between the vascular lesion and adjacent structures. It can also differentiate a high-flow from a low-flow lesion. In the present study, both duplex ultrasonography and MRI were performed routinely, and we found them the most important minimally invasive tests. Selective and superselective arteriography are used for predominantly arterial and AV shunting to determine further detailed anatomic information and to decide on the treatment plan. 9
High-flow AVMs pose the greatest risk for severe bleeding during surgical resection. The initial reduction of the volume of blood flow in the vascular malformation is recommended. At present, preoperative transcatheter superselective embolization is preferred to proximal ligation because it can recruit vessels that may be surgically inaccessible. 12 Many embolizing materials are available nowadays. A liquid adhesive such as NBCA has become the first line of therapy at many centers. These agents polymerize on contact with ionic materials such as blood. 13 NBCA was used in most of our cases. We found that it was easy to deliver, free from complications, and relatively cheap. Although the current series is relatively small, our outcome assessment and follow-up were prospective and precise. Other retrospective studies have showed that transcatheter embolization can eliminate or improve the symptoms of AVM in a high percentage of patients. 2,6,7,9,13
Some authors do not recommend NBCA as a sole permanent agent to control a lesion effectively because there is no evidence of permanent damage to the endothelium. 7,9 Combined treatment consisting of selective embolization followed by surgery usually gives the best results. 7,14,15 Long-term outcomes from studies in which the treatment was embolization alone were disappointing. 16,17 Some authors reported that postembolization surgery was performed in only 6% of cases. In this series, only 28% of the cases had complete resolution of the symptoms, and in 8%, the symptoms persisted or got worse. Complete surgical resection was indicated in most of the cases within 2 to 5 days of embolization. 7,18
Many sclerosing materials have been used for treating AVM with a high recurrence rate. The origin of AVM as an embryonal remnant, maintaining the original ability to grow when conditions become optimum, may explain this high recurrence rate. 19 Ethanol sclerotherapy was used recently, with high success and low recurrence rates. 19–21 Absolute alcohol induces denaturation of tissue protein, precipitating protoplasm and subsequent permanent obliteration of the vessel lumen, with no chance of regeneration of endothelial cells. 22 Although the number of cases was relatively low in the present study, with a short follow-up, the success and recurrence rates were similar to those of previous reports. 19–21 On the other hand, ethanol is dangerous because of its toxicity and local complications. 19 In the present study, we tried to be selective and used extreme caution. Most of the complications in our studies and others 3 were minor and confined to surface epithelium and underlying subcutaneous tissue. 21–23 These usually healed with standard wound care.
In conclusion, a multidisciplinary team approach improved the results in our series and others. 4,24,25 Management of AVM by a surgical and endovascular approach can deliver excellent results, with acceptable morbidity and no recurrence in the early follow-up period. Preoperative embolosclerotherapy facilitates the surgical resection and allows treatment of cases that were beyond the scope of conventional surgical treatment.
Footnotes
Presented in part at the 7th International Congress of the Asian Society for Vascular Surgery, Kuala Lumpur, Malaysia, August 2006.