
Abstract
A “recurrent” aortoenteric fistula (AEF) is very rare and in literature anecdotic. Currently, graft excision and extra-anatomic bypass are considered the treatments of choice, but are associated with significant mortality and morbidity. Herein, we describe the case of a “recurrent” AEF treated before definitive extra-anatomic bypass, by two different, staged bridge solutions: allograft in situ replacement and endovascular grafting. At 1, 3 and 6-month follow-up, the patient was asymptomatic and normally active.
Keywords
A “recurrent” aortoenteric fistula (AEF) is a dramatic but rather infrequent late complication of abdominal aortic surgery. Treatment of this condition is mandatory even if the resulting morbidity and mortality remain very high.
The traditional management of AEF requires graft removal and an extra-anatomic bypass grafting procedure, 1–9 usually with staging. In the presence of a “recurrent” AEF, the critical needs are to stop bleeding, to eradicate the infection, to repair the enteric hole, and to restore blood flow for the lower limbs. We report a staged endovascular and surgery treatment of a “recurrent” AEF.
Case Report
A 61-year-old man was admitted with melena, sepsis, and signs and symptoms of hypovolemic shock, which had developed in the last few hours.
The patient's history included an hypertensive cardiomyopathy, a hemorrhagic stroke (with minor permanent neurologic deficits), a single episode of acute renal failure (acute tubular necrosis after nonsteroidal anti-inflammatory drug intake), and an aortobisiliac Dacron graft repair for an abdominal aortic aneurysm 15 years previously. After 10 years, he developed a huge pararenal pseudoaneurysm and a concomitant AEF with melena, fever, hyperleukocytosis, and severe anemia. In another hospital, physicians had decided to attempt two different endovascular procedures, with a tube-graft endoprosthesis (Talent, Medtronic, Santa Rosa, CA), for the exclusion of the aortic pseudoaneurysmatic sac and of the AEF. These two surgical interventions were unsuccessful, and 4 months later (3 years before the last hospitalization described here), the patient was newly admitted to our emergency room with melena, hematemesis, and sepsis. He underwent exeresis of a huge abscess (about 6 cm in diameter) around the intestine near the graft, removal of the previous Dacron graft and tube endoprosthesis (Figure 1), and aortic reconstruction with a cryopreserved allograft of the thoracic arch and innominate artery donated from a brain-dead young woman (Figure 2). The patient was discharged on postoperative day 27 and was prescribed a broad-spectrum antibiotic therapy, but despite our advice, he missed all of his follow-up appointments.
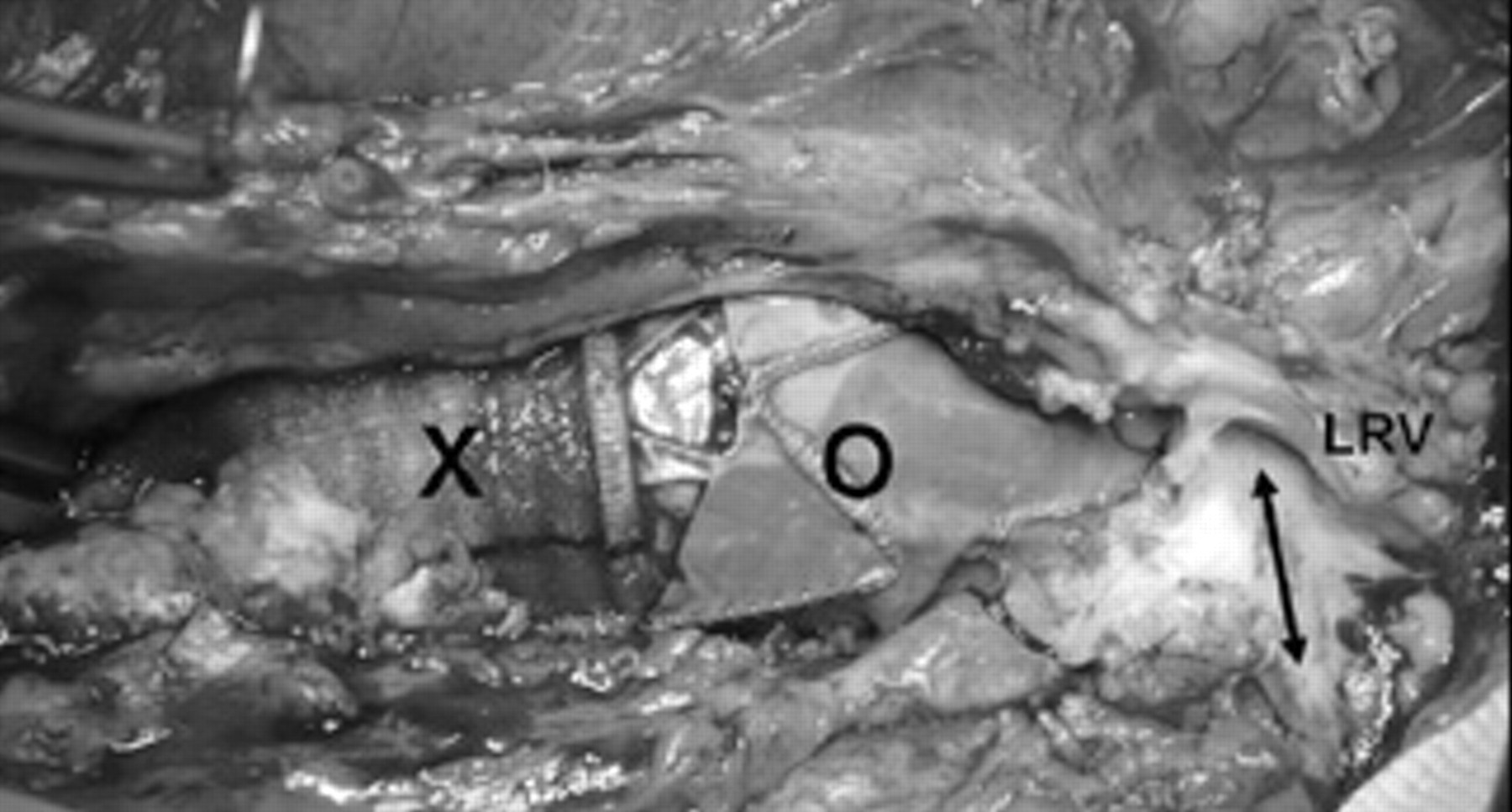
LRV = left renal vein transacted; O = the Talent (Medtronic) endoprosthesis that appears at the root of the pararenal aortic aneurysm; X = the Dacron aortobisiliac graft.

The composite-cryopreserved (aortic arch + innominate artery) allograft in place. LRV = left renal vein transacted.
During the current admission to the emergency room, computed tomographic (CT) angiography highlighted a new AEF between a blister of the homograft and the first portion of the jejunum (Figure 3). The patient had hemoglobin of 6.3 g/dL, active melena, and blood pressure of 70/45 mm Hg. The emergent treatment was to stop the hemorrhage, so an aortouni-iliac endoprosthesis (+ femorofemoral bypass) was performed under local anesthesia. The attempt was successful, the bleeding was stopped, and the hemoglobin was stable at 10.5 g/dL over the following days. Broad-spectrum antibiotic therapy (teicoplanin 400 mg intravenously daily, metronidazole 500 mg intravenously × 2 days, and imipenem 500 mg intravenously × 3 days) was administered as well. After 10 days, when the patient's conditions were deemed fit, we carried out “definitive” surgical treatment consisting of an axilloiliac bypass, the closure of the jejunum opening, the removal of the aortouni-iliac endoprosthesis and the ligature of the aorta below renal arteries.
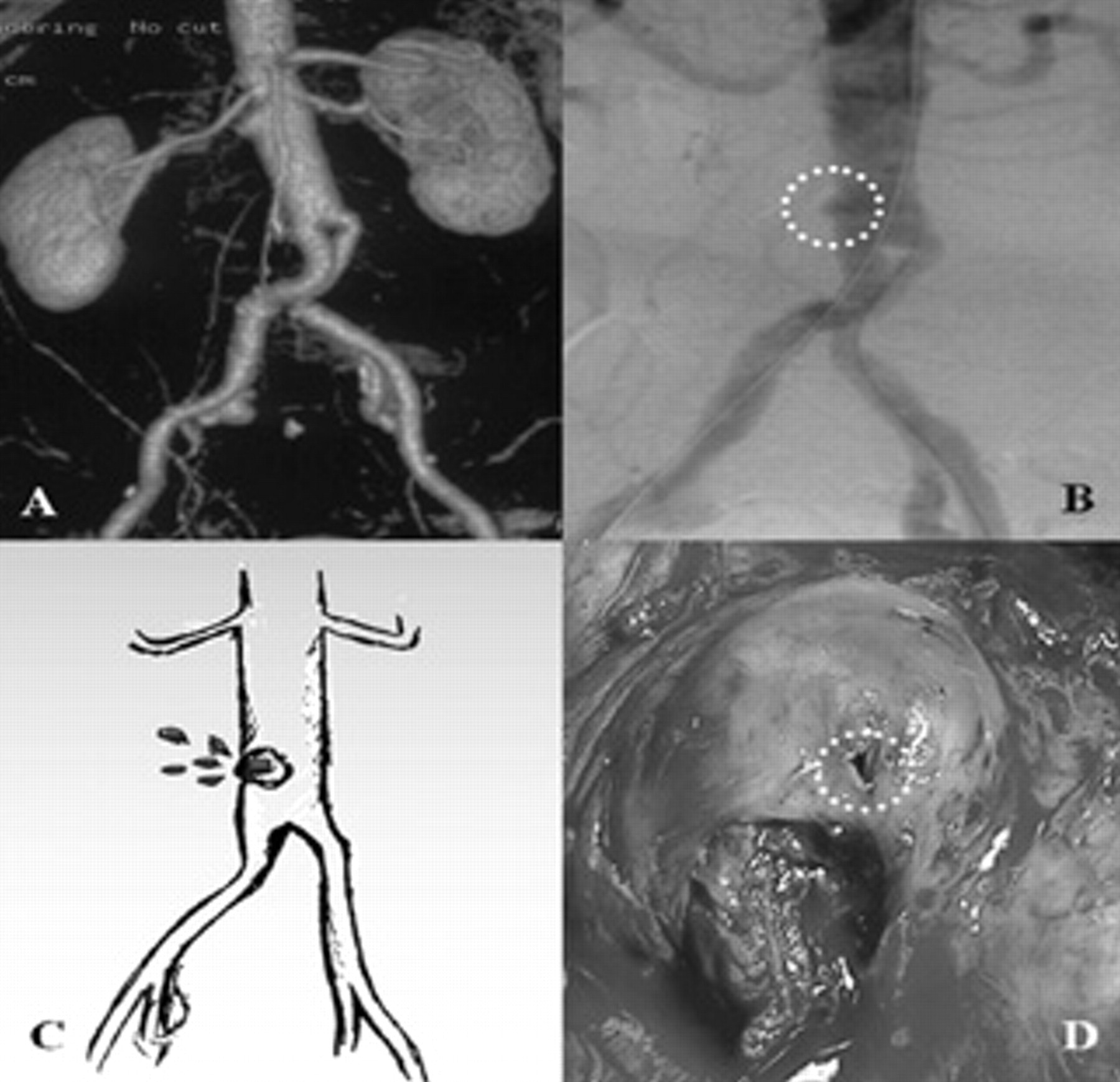
A, The computed tomographic angiogram 1 week after allograft placement; B, the angiography that highlights the allograft blister; C, a scheme of the aortoenteric fistula owing to the blister; D, the intraoperative picture of the blister.
The patient recovered uneventfully from the procedure and was discharged 12 days after surgery. At the 1- and 6-month follow-ups, the axillobifemoral bypass was patent on a duplex sonogram. No direct or indirect sign of infection was found at staged CT angiography.
Discussion
AEF are rare, lethal causes of massive gastrointestinal tract bleeding 10,11 and one of the most challenging diagnostic and therapeutic problems encountered by vascular surgeons. The morbidity and mortality rates are still alarmingly high, particularly in a relapsing AEF.
Conventional treatment of an AEF is based on débridement, repair of the enteric fistula, and removal of the inciting factor. In the literature, anatomic bypass (antibiotic impregnated or silver-coated prosthesis, homograft, or allograft), extra-anatomic bypass (axillobifemoral bypass), and, recently, stent grafting to replace the diseased aorta 12,13 are all described. Nevertheless, a “recurrent” AEF is a more challenging problem for the treatment of both gastrointestinal hemorrhage and infection.
It is necessary to offer the patient the revascularization that could guarantee better results in terms of mortality, morbidity, and anatomic durability.
As we know, the source of infection, and so the fistulous communication, cannot be removed by an endovascular procedure, and the infection cannot always be solved even with aggressive antibiotic therapy. Some authors recently reported the endovascular repair of an AEF in an afebrile patient with a normal leukocyte count, but this treatment failed 27 months later. 12 It must be stressed that a stent graft was placed in the patient successfully after the intestinal closing and elimination of the infection.
Moreover, we can also consider the allograft a “bridge solution” 14–17 for a staged procedure of lower limb revascularization in a case of secondary AEF.
Reported patency and limb salvage for elective extra-anatomic bypass may be acceptable, 8,9,18,19 but some authors reported suboptimal results in cases of extra-anatomic regrafting in the presence of aortic graft infection. 1,3,5,20 In accordance with these last reports, we performed in situ regrafting (cryopreserved allograft). In the literature, early and long-term results of allograft replacement are at least similar to those of extra-anatomic bypass in managing AEF or graft infection. However, we are aware that an allograft can deteriorate for a chronic rejection or for structural degradation of the medial layer. 16 In fact, after a few years, the allograft in this case developed a blister, probably owing to structural degradation in the region of the suture of the composite allograft.
When the symptomatic “recurrent” AEF with hemorrhagic shock came to our attention, we decided to promptly stop bleeding, and this was done via a mini-invasive procedure (aortouni-iliac + femorofemoral bypass under local anesthesia). But thanks to the precedent experience, we took advantage of the endovascular procedure only to prepare the patient for the more definitive procedure.
Moreover, a very strict follow-up protocol is important to avert complications owing to aortic stump disease, occlusion, or infection of prosthetic extra-anatomic bypass grafts. 20
In this anecdotal case, we have shown that allograft replacement and endovascular exclusion for a secondary AEF are bridge solutions to a late extra-anatomic bypass grafting when the patient is better able to benefit from this kind of definitive treatment.