
Abstract
Over 95% of abdominal aortic aneurysms (AAAs) rupture into the retroperitoneal space. Rare types of AAA ruptures comprise ruptures into the inferior vena cava with aortocaval fistula formation (ACF), ruptures into the duodenum with formation of a primary aortoduodenal fistula (ADF), and chronic contained ruptures (CCRs). This article presents a study of 41 cases with unusual forms of ruptured AAA of a series of 506 patients with AAA rupture treated within a 14-year period. There were 11 cases of CCR, 5 cases with ADF, and 25 cases with ACF. The correct preoperative diagnosis was established in 6 (of 11) cases of CCR, in 2 (of 5) cases of primary ADF, and in 13 (of 25) cases of ACF. AAA replacement was performed in 8 cases using a tube graft, whereas a bifurcated graft was used in 31 patients because of the distant extent of the atherosclerotic/aneurysmatic lesions engaging iliac arteries. Two patients had an axillobifemoral bypass. The overall 30-day mortality rate was 19% (8 of 41), with subgroup mortality rates of 0 (CCR), 60% (ADF), and 20% (ACF). Diagnosis and treatment are simplest in cases of CCR and the most complicated in cases of ADF.
Rupture is the most frequent and potentially fatal complication of abdominal aortic aneurysms (AAAs). More than 95% of AAAs rupture into the retroperitoneal space, forming a retroperitoneal hematoma. 1–13 Rare types of AAA ruptures are rupture into the inferior vena cava with aortocaval fistula (ACF) formation, rupture into the duodenum with formation of a primary aortoduodenal fistula (ADF), and chronic contained rupture (CCR). The aim of this article is to present our experience of these uncommon forms of ruptured abdominal aortic aneurysms (RAAAs). 14–24
Materials and Methods
Owing to AAA, between January 1991 and June 2005, 1,784 consecutive patients in our department underwent surgery. Of this population, 506 (28.36%) patients suffered from RAAA. Forty-one cases of unusual types of RAAA were included in the study (11 patients with CCR of an AAA, 5 patients with a primary ADF, and 25 patients with ACF owing to an RAAA). The demographic characteristics of the patients, risk factors, associated cardiovascular diseases, and operations are presented in Table 1.
Demographic Characteristics of the Patients, Risk Factors, Associated Cardiovascular Diseases, and Operations
The criteria used to identify CCR were set by Jones and colleagues in 1986. 22 Patients with CCRs of an AAA, already diagnosed with an AAA, had a history of back pain or collapse during a period lasting between 21 days and up to 3 months (39.2 days) prior to admission. The hematocrit, pulse rate, and arterial tension of all patients were normal at admission. Physical examination revealed a pulsatile abdominal mass. Preoperative duplex ultrasonography identified an infrarenal AAA with a “lobular” extra-aneurysmal mass that compressed the inferior vena cava in three cases, whereas a “saccular” infrarenal AAA was detected in two patients. The angiography showed compression of the right renal artery in three cases. Computed tomography (CT) or magnetic resonance imaging (MRI) revealed a retroperitoneal hematoma in five patients. Posterior localization of aneurysmal ruptures with an organized retroperitoneal hematoma was found intraoperatively in all CCR cases. The correct preoperative diagnosis of CCR of an AAA was established in six cases, whereas it was suspected in five cases (Figure 1). The replacement of AAAs was performed using a tube graft in four cases, whereas a bifurcated graft was used in seven cases.
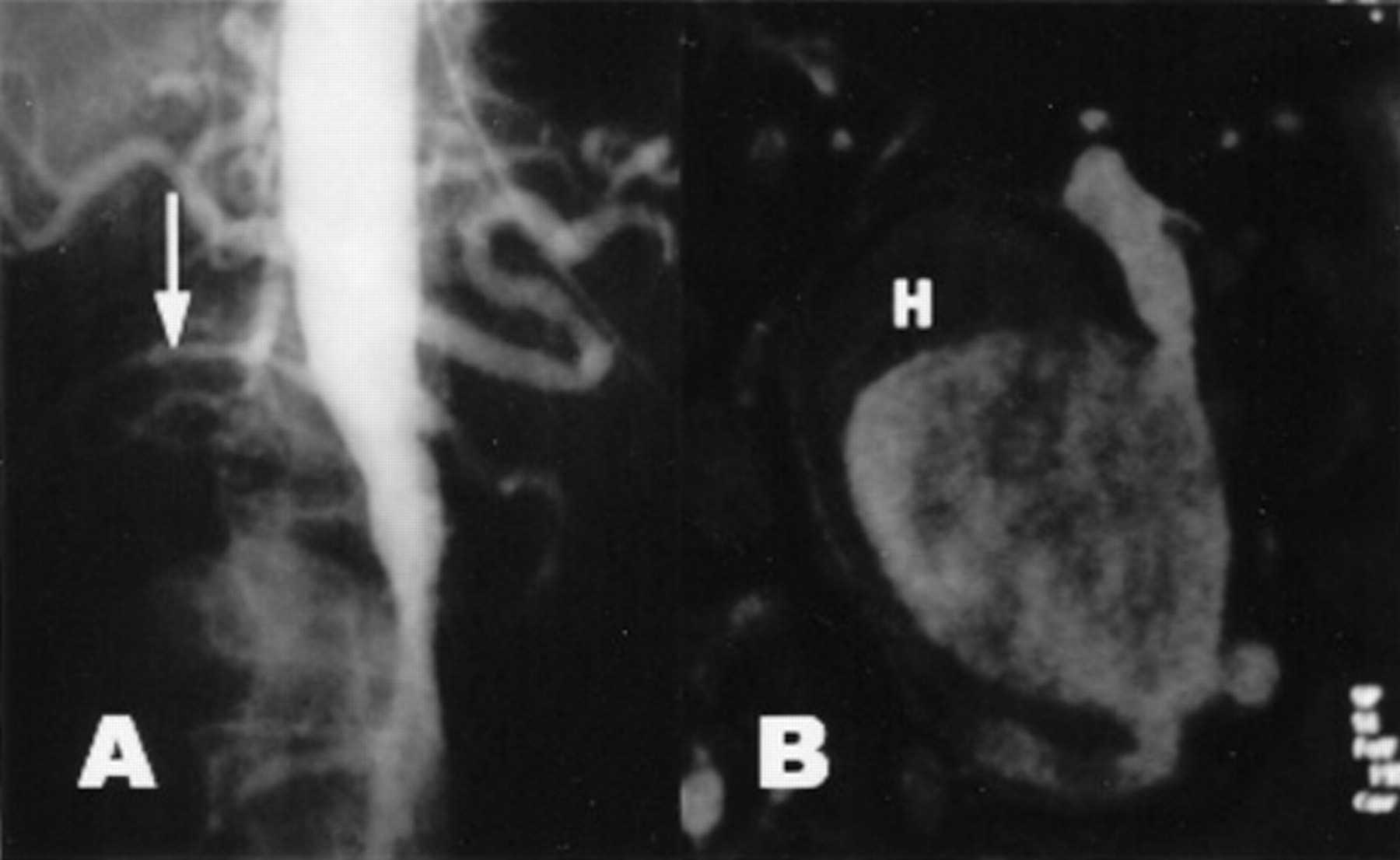
A, An angiogram shows a giant abdominal aortic aneurysm compressing the right renal artery (arrow). B, A magnetic resonance image of the same patient shows that the right renal artery is compressed by a retroperitoneal hematoma (H). Chronic contained aneurysmal rupture had developed 40 days earlier.
All five patients with a primary ADF had lower gastrointestinal bleeding; four of them suffered lower back pain, whereas two patients had a palpable abdominal mass, and in three patients, hemorrhagic shock occurred at admission. In two cases, the definitive diagnosis was established using gastroduodenoscopy, and in the other three cases, the diagnosis was established intraoperatively (Figure 2).

The intraoperative finding of a patient with rupture of an abdominal aortic aneurysm into the duodenum.
After an aneurysmal resection in patients with a primary ADF, the revascularization of the lower limbs was accomplished with an extra-anatomic axillobifemoral bypass graft in two cases and with in situ graft placement in three patients as no evidence of gross retroperitoneal contamination was present. The duodenal defect was closed transversely with a standard two-layer suture technique followed by fistula excision in four cases. Partial duodenal resection followed by duodenojejunostomy and an additional Brown enteroenteroanastomosis was performed in one case by a general surgeon. In order to prevent the eventual infection of in situ placed grafts, we practiced the following procedures: thorough irrigation of the retroperitoneum with a mixture of saline and antibiotics, the use of a silver bonded graft, covering of the graft with débridement aortic wall and fibrin sealant and wrapping with a viable pedicle of omentum, postoperative antibiotic treatment tailored to the cultured organismus of the aortic wall samples and its sensitivity or empiric prophylactic antibiotics were given when culture samples were negative.
Twenty-five patients with ACF seemed to have a typical ruptured aneurysm with lower back pain and a palpable pulsating abdominal mass. Abdominal bruit presence was the most reliable physical sign (18 patients; 72%). Some of them were in a state of hemorrhagic shock at admission (18 patients; 72%). Table 2 presents more details about the clinical manifestation of an ACF owing to an RAAA.
Clinical Presentation of Aortocaval Fistulae
CHF = congestive heart failure; CVP = central venous pressure.
The diagnosis of ACF had not been established prior to operative treatment in 12 (48%) cases. For diagnostic purposes, we used duplex ultrasonography in 9 (36%), CT in 8 (32%), MRI in 3 (12%), and angiography in 7 (28%) cases. The urgency of surgical procedures was indicated by physical examination of six patients (24%) who had a palpable pulsating abdominal mass and abdominal bruit but were in a state of severe hemorrhagic shock. The diagnosis of these six patients was suspected correctly, but the lack of time did not allow objective imaging examination to prove ACF (Figure 3).

Ruptured abdominal aortic aneurysm into the left common iliac vein with fistula formation.
In 17 cases, the ACF was located between the infrarenal aorta and the inferior vena cava; in 6 cases, it was between the aorta and left common iliac vein; and in 2 cases, it was between the aorta and right common iliac vein. The bleeding from the inferior vena cava after aneurysmal opening was controlled by direct finger tamponade or by instruments pressing proximally and distally from the fistula site in 22 cases. The intraluminal balloon occlusive catheter, introduced through the femoral vein, was used in three cases. The operative technique included, as an obligatory procedure, transaneurysmatic fistula repair. The reconstruction of the abdominal aorta was performed with a tube graft in 3 patients and with a bifurcated graft in 22 cases. More details on the type of reconstructive vascular procedures performed on all described patients are presented in Table 3.
Reconstructive Vascular Procedures
AFF = aortobifemoral bypass; AII = aortobi-iliac bypass; AxFF = axillobifemoral bypass; tube = tube graft interposition.
Patients who survived the first 30 postoperative days were followed until June 30, 2005. The follow-up protocol included clinic visits with a physical examination and duplex ultrasonography or CT scan at 3 and 6 months and annually thereafter.
Results
The median duration of follow-up was 102 months (range 24–186 months) for ACF, 49 months (range 6–120 months) for CCR, and 99 months (range 12–186 months) for ADF; during follow-up, there were five deaths (one ADF, one CCR, three ACF) from causes unrelated to a previous operation on the aorta. Two patients refused further follow-up, one after 45 months (ACF) and the second one after 24 months (CCR). During follow-up, there was no graft failure or recurrent fistula.
Table 4 presents the early mortality rate after surgery for all 41 patients. In all patients with an ADF, when anatomic in situ reconstruction with a synthetic graft had been performed, a retroperitoneal infection developed that caused a secondary duodenal fistula and hemorrhage or sepsis and multiple organ failure (MOF), and these patients died during the first 30 postoperative days. It is important to note that all deaths, after a surgically treated ACF caused by an RAAA, were related to patients who were misdiagnosed prior to surgery and who were in hemorrhagic shock at admission.
Early Mortality Rate (the First 30 Postoperative Days)
MOF = multiple organ failure.
Discussion
Explanation of the relative high proportion of ruptures in our series can be found in the high occurrence of risk factors (eg, the high rate of heavy smokers, which is characteristic of the region; stress) and poor primary health care (no ultrasound screening program, inadequate monitoring of risk factors), which are results of the economic crisis and war that was waged in this region for more than 10 years. These socioeconomic factors also explain the prevalence of duplex scans and angiograms: they are the least expensive imaging modalities for preoperative evaluation in comparison with the CT scan or MRI, not to mention logistical issues (there is only one CT scanner and one MRI machine available to all clinics within the Clinical Centre of Serbia). Endovascular aneurysm repair is not used for the same reasons (high cost).
CCR is a rare outcome of RAAA. The term was introduced by Jones and colleagues in 1986. 22 “Sealed,” 21 “spontaneously healed,” 24 and “leakage” 23 RAAA are synonyms used in previous reports. The sealed RAAA was first described by Szilagyi and colleagues in 1961. 21 In their case study, the rupture was small and hemorrhage was effectively encircled by the surrounding tissue reaction. The slow rate of blood loss allows the patient to remain hemodynamically stable. There are two mechanisms of chronic contained RAAA. 25,26 In cases with small aneurysms, the aortic wall is still structurally fairly strong and the small aneurysm tear tends to be limited in extent. When it comes to larger aneurysms, the enlargement of the aneurysm creates adherence to the surrounding structures, producing scar tissue, so when the perforation occurs, it is limited by the strong perianeurysmal reaction. 25 The posterior localization of the rupture (present in all of our cases) is a very important factor for the development of chronic contained RAAA. 15,26 Strepetti and colleagues described the posterior rupture in 62.5% of their 16 cases. 25 The surrounding structures behind the posterior aortic wall (vertebral bodies, inferior vena cava, paravertebral muscles) can cover the defect on the aortic wall after the initial rupture and limit bleeding. 21,25,27 In 1986, Jones and colleagues classified the clinical concept of CCR. 22 Their criteria to identify this entity are previous knowledge of the AAA; previous symptoms or signs that may have been resolved; normal arterial tension, pulse rate, and hematocrit at admission; a retroperitoneal hematoma detected by duplex ultrasonography, CT, or MRI; and intraoperative and histologic confirmation of an organized retroperitoneal hematoma. The time interval between the suspected initial rupture and its diagnosis in our cases of CCR was 39.2 days (21 days up to 3 months). Ohtake and colleagues described a 2-year interval between the initial rupture and diagnosis. 27 In one of the largest studies, consisting of 16 cases of chronic contained RAAA, the time interval between the initial rupture and diagnosis ranged from 4 weeks to 4 months. 25 The preoperative finding of the organized retroperitoneal hematoma detected by duplex ultrasonography, CT, or MRI is the most important preoperative sign of chronic contained RAAA. 27 Sometimes that hematoma is described as a “lobular mass” 15,28 or a “pseudoaneurysm.” 29 The angiography can show a “saccular” AAA or compression on the renal arteries or inferior vena cava. 15,25,28,29 The surgical treatment of chronic contained RAAA is simpler owing to hemodynamically stable patients. The operative mortality rate in the case of chronic contained RAAAs is lower in comparison with the typical form; however, they both require urgent treatment.
A primary ADF is usually a result of AAA erosion into the duodenum (third or fourth portion of the duodenum). The incidence of the primary ADF is low, ranging from 0.1 to 0.8%. 17,18,30,31 However, because of its very high mortality rate, ranging from 14 to 70%, it is of great medical importance. 16–18,30,31 For the first time, in 1829, Sir Astley Cooper described a primary aortoenteric fistula (AEF) caused by an AAA rupture. 32 The first successful treatment of a primary AEF by suture of the duodenal defect and aneurysmorrhaphy was performed by Haberer in 1957. 33 Numerous authors had the intention of identifying additional symptoms and signs that would detect the presence of an AEF more precisely, which is of vital importance considering the fact that gastrointestinal bleeding is a sign of a great number of different diseases. A primary AEF is surely present if there is gastrointestinal bleeding, lower back pain, data on an AAA, or a palpable abdominal mass. 34,35 That was the case in two of our patients with a primary AEF. Thanks to the analysis of 28 primary AEF cases, Dutch authors found the following frequencies of its symptoms and signs: gastrointestinal bleeding, 100%; abdominal pain, 64.28%; and pulsatile abdominal mass, 67.85%. 17 Another report by Danish authors, which includes 46 cases with a primary AEF during the period between 1958 and 1973, showed this frequency of its symptoms and signs 18 : hematemesis, 78%; lower gastrointestinal bleeding, 50%; combined lower and upper gastrointestinal bleeding, 28%; and combined abdominal pain, a palpable abdominal mass, and some forms of gastrointestinal bleeding, 28%. Many diagnostic procedures are used in identifying AEF owing to the involvement of two different organ systems (the gastrointestinal and the aorta). A positive endoscopic finding is absolute proof of an ADF. 36,37 Gastrointestinal bleeding in a patient suspected of having an AEF is an indirect sign, 35,38 disregarding negative endoscopic findings in the esophagus, gaster, and proximal part of the duodenum. The most obvious angiographic sign of an AEF is the extravasation of the contrast material, which is rarely found because of the closed fistula with thrombus. 38–40 That is the reason why angiography during the diagnosis of an AEF shows a great number of false-negative results. Treatment of an AEF is complicated as it requires a procedure on two different organ systems (gastrointestinal and aorta) and has four phases of development: proximal bleeding control from the aorta, closing of the gastrointestinal defect, eradication of the infection, and revascularization of the lower limbs. 41–45 The simplest method by which to perform duodenal fistula closure is a transverse two-layer suture. Prior to a suture, an abundant excision of the fistula with surrounding unvital tissue is necessary. 34,37,39,45 This procedure was performed in four of our cases. When the fistula is large, partial duodenal resection followed by end-to-end anastomosis or duodenojejunostomy is indicated. In such cases, additional Brown enteroenteroanastomosis is very useful (one of our cases). 39 Lower limb revascularization can be performed by two different procedures: anatomic (in situ) or extra-anatomic. 34,37,46,47 It has been proved to be better to perform an anatomic procedure with a cadaveric homograft. 48 In all three of our cases, when anatomic in situ reconstruction with a synthetic graft was performed, a secondary infection developed, and these patients died during the first 30 postoperative days (sepsis and MOF had developed in two patients and secondary duodenal fistula and hemorrhage in one patient). Two of our patients with extra-anatomic axillobifemoral bypasses survived the first 30 postoperative days. In cases of a primary ADF caused by an RAAA, we recommend fistula excision followed by closure in two transverse layers, as well as lower limb revascularization with extra-anatomic axillobifemoral bypass grafting. The relationship between an AEF and endovascular aneurysm repair (EVAR) is very specific. Both AEF following EVAR 49,50 and endovascular repair of AEF 51 are described. Persisting communication between the enteric fistula and the endograft after EVAR of an AEF lead to the development of new AEF formation. 52,53 For this reason, endovascular treatment of an AEF is better used as a bridge procedure to definitive conventional treatment after hemodynamic stabilization of the patient. 52,53
The most common cause of an ACF is an aneurysm rupture. 14,54,55 According to published figures, the incidence of an ACF is quite low and occurs between 0.22% and 6.04%. 19,20 When the typical clinical manifestation is identified (abdominal mass, abdominal bruit, acute increased heart rate), the diagnosis is obvious. According to published studies, half of diagnosed patients have unusual features. 56 In our study, 12 patients (48%) were not given the proper diagnosis. This failure to establish the correct diagnosis was emphasized earlier. 14,57 Several factors may contribute to misdiagnosis. The mural thrombus within the aneurysmal sac may be the reason for partial or total fistula obstruction. The temporary obliteration of the fistula may cause loss of typical continuous abdominal bruit. 56,58 Seven of our patients did not have this sign. The predominant feature of clinical presentation is a large venous inflow producing congestive heart failure and possible heart decompensation. 56 We have noted only three (12%) such patients. In cases of RAAA with aortocaval communication, compression on adjacent veins (usually the vena cava or proximal left iliac) exists that can decrease flow toward the heart and augment peripheral venous flow and pressure. This kind of disturbance results in the redirection of the blood flow toward the pelvis and extremities, producing regional venous hypertension. 57 Consequences of such disarrangement most often include the swelling of the lower extremities combined with other symptoms: hematuria, renal insufficiency, scrotal edema, and rectal bleeding owing to superficial colorectal mucosal vein rupture. 57–59 Urgent surgical repair is required in the case of an ACF, especially one caused by an RAAA. Proximal aortic cross-clamping decreases the blood flow through the fistula. The problem of controlling the venous bleeding originating from the fistula is most important and the first to be solved. It is possible for a surgeon to provide immediate control by using the fingers to manage a tamponade. On the other hand, it is possible to use balloon occlusive catheters previously inserted via the femoral veins positioned proximally and distally. 19,20,54 Data published in studies provide facts about the operative mortality rate, related to ACF, ranging from 16 to 66%. 20,54,60–65 In our study, the mortality rate was 20% and all five deaths occurred in patients who suffered hemorrhagic shock at admission and were incorrectly diagnosed prior to surgery, which led to inadequate operation planning and uncontrolled intraoperative hemorrhage. As an important clinical entity, ACF demands urgent operative treatment with a proper preoperative diagnosis. 61 Successful endovascular treatment of infrarenal aortic aneurysms ruptured into the inferior vena cava, 66–68 as well as of traumatic ACF, is described in the literature. 69
Conclusions
CCR, as well as ADF and ACF, are rare types of RAAAs. Diagnosis and treatment are simplest in cases of CCR, whereas the most complicated are cases of primary ADF.