
Abstract
An association between abdominal aortic aneurysm (AAA) and abdominal wall hernia has been suggested, possibly reflecting a common collagen disorder. The same mechanism may also cause a greater frequency of diastasis recti among patients at risk of developing AAA. Diastasis recti could be used to identify patients at risk of AAA, with implications for AAA screening. The aim of this study was to determine whether an association between diastasis recti and AAA could be demonstrated.
The preoperative computed tomographic (CT) scans of 75 male patients undergoing elective AAA repair were retrospectively examined and linea alba width recorded at supraumbilical and subumbilical levels. Measurements were compared with controls frequency matched for age.
Fifty patients with AAA were observed to have supraumbilical diastasis recti on preoperative CT compared with 47 controls. Mean linea alba width was not significantly different between the two groups at either the supraumbilical (19.3 mm vs 20.7 mm, p = .45) or subumbilical (3.6 mm vs 4.3 mm, p = .43) level.
The findings do not support the hypothesis that the presence of diastasis recti can serve as an indication to select male patients for screening for AAA.
Abdominal aortic aneurysm (AAA) is a common cause of morbidity and mortality with an approximate prevalence of 5 to 10% in males aged 65 to 79 years. 1 Mortality among patients with acute aneurysm rupture approaches 80%. 2 The comparatively low operative mortality from elective AAA repair means that it is desirable to detect aneurysms before rupture. Screening for AAA among the general population is not currently undertaken in Australia, although a Cochrane review suggested that screening among males aged 65 to 79 years produces a significant reduction in aneurysm-related mortality. 3 Apart from the recognized associations of increasing age, male sex, smoking, a positive family history, and the presence of concomitant atherosclerotic disease, few more specific risk factors for the development of AAA are known. 4 Screening may be more cost-effective if individuals who are at increased risk of developing AAA can be more specifically identified.
An increased incidence of abdominal wall hernias among patients with AAAs has been described in the literature. 5–14 It has been proposed that a common abnormality of connective tissue accounts for this reported greater frequency of abdominal wall hernias among aneurysm patients, and there are mounting experimental data documenting a range of collagen and matrix protein abnormalities as possible etiologic factors. 15–21
The linea alba is an anterior midline fibrous structure into which the aponeuroses of the anterior abdominal wall muscles insert. Normally, there is a short distance between the medial border of each rectus abdominis muscle, with the linea alba interposed. An increase in this distance produces diastasis recti. The clinical correlate of diastasis recti is referred to as divarication of the rectus abdominis muscles.
The same disorder of connective tissue proposed to account for an association between AAA and abdominal wall hernias might similarly involve the linea alba and result in a higher incidence of diastasis recti among patients at risk of developing AAA. Should this be true, the clinical observation of divarication of the rectus abdominis muscles would provide a means of identifying patients at increased risk of developing AAA. This population could be selected as a subgroup for screening.
Accurate correlation between computed tomographic (CT) measurement of linea alba width and intraoperative direct measurement has been established. 22 Additionally, normal values for linea alba width have been defined (≤ 15 mm above the umbilicus and ≤ 14 mm below). 23 Using these data and preoperative CT imaging, the prevalence of diastasis recti in a population of patients with AAA was examined. Comparison was then made with the prevalence of diastasis recti in a cohort of patients without AAA.
Methods
Retrospective analysis was undertaken of preoperative computed tomographic angiogram (CTA) studies performed on patients undergoing elective AAA repair at a single institution over a 5-year period (August 2002–August 2007). CTA data were obtained from the Christchurch Hospital Department of Radiology Patient Archiving and Communication System. Each computed tomographic urogram (CTU) was obtained using helical data acquisition with coronal and axial reformatting consisting of contiguous 2.5 mm slices. AAA was defined as aortic dilatation greater than 55 mm in maximum short axis dimension as measured on preoperative CT imaging in the transverse plane. Patients were excluded if there had been previous midline anterior abdominal wall surgery or if imaging was unavailable for review. Female patients were not included owing to the confounding effect of the gravid abdomen.
On each CTA, the CT measurement tool was used to determine the maximum width of the supraumbilical and infraumbilical linea alba (Figure 1). Several measurements were taken above and below the umbilicus, and the largest obtainable values of supraumbilical and infraumbilical width were recorded. A single operator (T.M.) performed all measurements to ensure consistent measurement technique. Diastasis was defined as being present when the linea alba width exceeded 15 mm above the umbilicus and 14 mm below the umbilicus. Radiologic assessment alone was employed in defining the presence or absence of diastasis, and patients were not physically assessed to determine whether there was evidence of clinically apparent divarication.
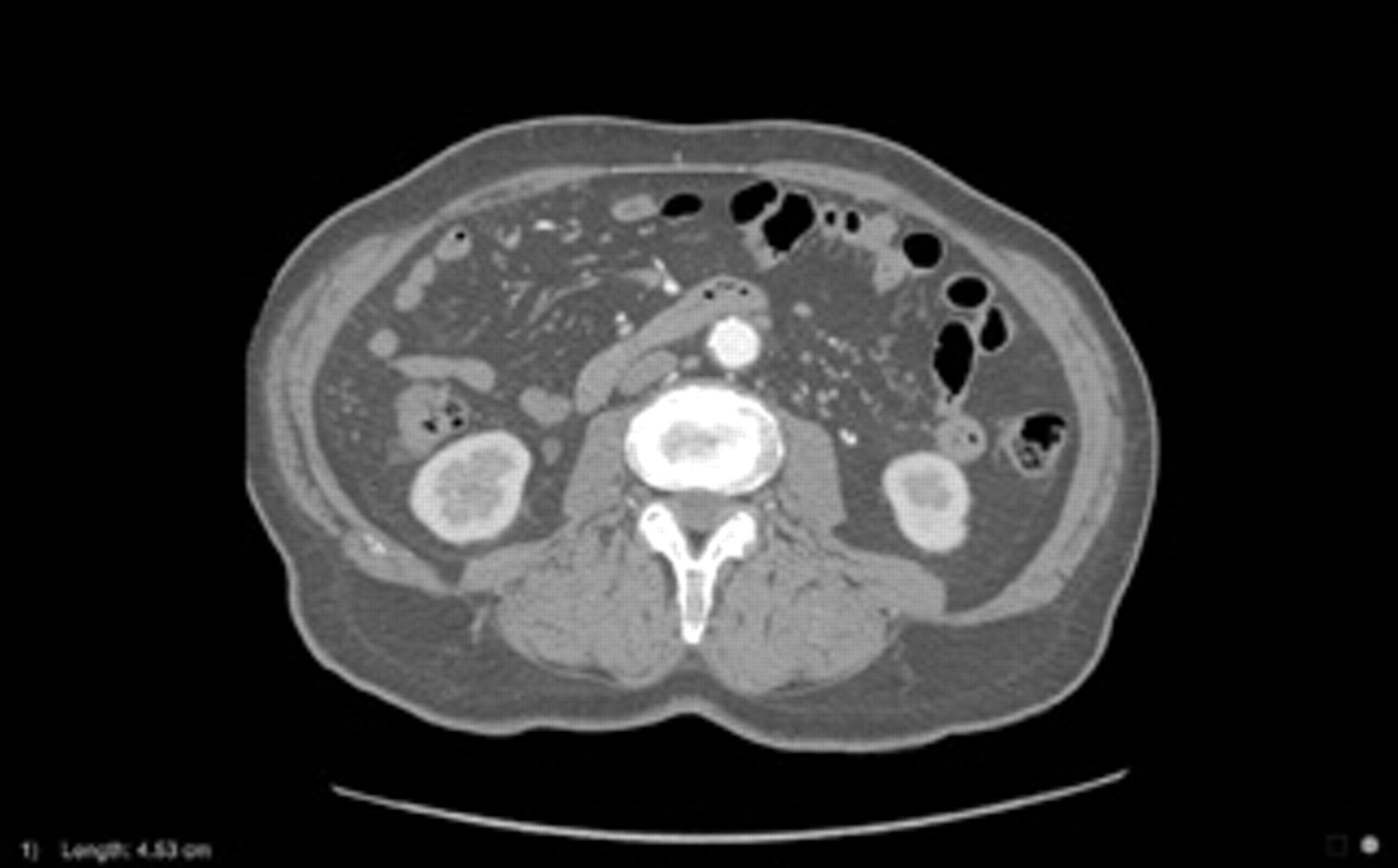
Transverse computed tomographic (CT) angiogram demonstrating supraumbilical diastasis recti and measurement of linea alba width with the CT measurement tool.
Control data were obtained through review of CTU studies from male patients frequency matched for age within 5-year intervals. Again, patients were excluded if there had been previous midline anterior abdominal wall surgery and if the maximum short axis abdominal aortic diameter exceeded 30 mm.
Proportions were compared using the program Confidence Interval Analysis. 24 Chi-square tests for contingency tables were also calculated. Means were compared using t-tests for independent groups, with Satherwaite's adjusted degrees of freedom if the folded F comparison of variances was significant. As a check, the nonparametric Wilcoxon test was also used where distributions were skewed. The statistical software SAS 9.1 (SAS Institute, Cary, NC) was used for these analyses.
Results
Seventy-five patients were included in the study cohort, with a mean age of 71 years (range 48–85 years, median age 73 years). The control cohort consisted of 75 individuals with a mean age of 71 years (range 47–92 years, median age 72 years). Fifty patients with AAA demonstrated diastasis recti at the supraumbilical level compared with 47 of the control patients, with the difference not being statistically significant (χ 2 = 0.26, df = 1, p = .61). Six patients in the case group and six patients in the control group had infraumbilical rectus diastasis (Table 1).
Number of Patients Meeting Criteria for Diastasis Recti in Case and Control Groups
Difference between two proportions: 0.04 (95% confidence interval −0.11, 0.19), p = .61.
The mean width of the supraumbilical linea alba was 19.3 mm (95% confidence interval [CI] 17.0, 21.6; SD = 10.1) among the AAA patient group and 20.7 mm (95% CI 17.8, 23.6; SD = 12.5) among the control patients. The mean difference was 1.4 mm (95% CI −2.3, 5.1; p = .45). At the subumbilical level, the mean width of the linea alba in the study population was 3.6 mm (95% CI 2.3, 4.9; SD = 5.6) compared with 4.3 mm (95% CI 3.0, 5.7; SD = 5.8) among control patients. The mean difference was 0.7 mm (95% CI −1.1, 2.6; p = .43) (Table 2). The distribution of the width at the subumbilical level was very skewed within both groups, so a square root transformation was applied. This reduced the skew but still did not reveal differences between the groups (t = 1.36, df = 148, p = .18). Likewise, the nonparametric Wilcoxon test also showed no significant difference (p = .16).
Diameter of Supra- and Subumbilical Linea Alba (mm) in Case and Control Groups
CI = confidence interval.
Discussion
A high prevalence of supraumbilical diastasis recti was found both among patients coming forward for elective AAA repair and among control subjects without AAA (67% and 63%, respectively). There was no statistically significant difference in the observed frequency of diastasis between the two groups. At the subumbilical level, the same number of patients in each cohort demonstrated diastasis recti by anatomic criteria. The mean linea alba width was also concordant between the groups. These results suggest no increased prevalence of anatomically defined diastasis recti among patients with AAA greater than 55 mm and infer that no benefit would likely be gained by selecting patients with clinically apparent divarication for screening procedures.
The hypothesis of an association between diastasis recti and AAA is an extrapolation from previous work documenting an association between AAA and abdominal wall hernia. 5–14 Given that a common biochemical defect in connective tissue integrity is proposed as the basis of this finding, it seems plausible that a similar association between AAA and rectus divarication might exist. Research demonstrating an increased prevalence of diastasis recti among AAA patients in comparison with individuals with peripheral vascular disease but absent aortic dilatation further supports this hypothesis. 25 Assuming such an association to be real, our study could be criticized on the basis that the relatively small patient cohort may have resulted in subsequent analysis lacking sufficient strength to detect a subtle but true association. Such a criticism is valid and acknowledged. Conversely, however, any association between diastasis recti and AAA sufficiently strong to be used in the selection of patients for screening should be detectable even in a relatively small cohort, such as the group examined.
Conceivably, diastasis recti seen on CTA may not correlate with divarication seen clinically. Given that linea alba width measured on preoperative CTA has been demonstrated to so closely approximate direct measurement, it was considered reasonable to use this commonly performed and readily obtainable examination modality as a surrogate for clinically based assessment of a possible association between diastasis recti and AAA. The hypothesis, proposing utility of such an association for screening purposes, would reasonably seem to require demonstration of a significant anatomic difference between the study and control populations, regardless of the means by which this was accomplished. Arguably, it is equally as valid to attempt to demonstrate a radiologic difference as it is a clinical one, although it is acknowledged that when proposing extrapolation of radiologically based conclusions to clinical correlates, some caution must be employed.
Patients coming forward for CTU generally have a low prevalence of potentially confounding concurrent intra-abdominal pathology and were regarded to be a more preferable group than the general inpatient population from which to derive control data. This choice may, however, have introduced bias into the findings. Obvious sources of bias, such as previous abdominal surgery and pregnancy, were controlled for through exclusion; however, the possibility of latent variables influencing results must be acknowledged. Additionally, the study population, comprising individuals coming forward for elective repair of AAA, may not precisely represent the population of all individuals with AAA, and, further, not all individuals with either AAA or clinical divarication come forward for CT imaging. The selective nature of the study population and control cohort must be acknowledged as having the potential to introduce bias into the results and conclusions derived.
Ultrasound screening has the potential for significant reduction in mortality among the population of patients with AAAs, particularly among males aged 65 to 79 years. 3 It is noted, however, that such screening remains controversial, for reasons that include the fact that patients with AAA do not necessarily die from ruptured aneurysms. Additionally, knowledge of the presence of an aneurysm can cause significant patient anxiety, and the balance of risk of surgery versus risk of rupture is difficult to establish. The issue of cost-effectiveness was not assessed by the Cochrane Collaboration, although other groups have indicated the cost of screening to be £28,400 per life-year gained and approximately £36,000 per quality-adjusted life-year, although these figures do diminish with time. 26 With such significant associated economic costs, it is clearly advantageous to select at-risk individuals prior to screening.
At the time of writing, we are aware of only one other publication examining the association between AAA and diastasis recti. 25 This clinically based investigation compared the prevalence of diastasis recti between patient groups that demonstrated either AAA or peripheral arterial disease (PAD). Given this contrasting methodology, limited direct comparison between this publication and our own is possible. It is of interest, however, that a significantly higher incidence of diastasis was present among patients with AAA compared with those with PAD alone.
A number of groups have previously demonstrated an association between abdominal wall hernias (in particular incisional and inguinal hernias) and AAA, although recent work has failed to corroborate these earlier results. 5–14,27 Any such association has been postulated to derive from a common underlying connective tissue deficiency, and substantial experimental work exists describing various fascial collagen abnormalities and matrix collagenase aberrations, especially in relation to members of the metalloproteinase family of proteolytic enzymes, that potentially form the basis for this. 15–21 Although a similar association involving AAA and rectus divarication would seem plausible, our research has failed to demonstrate this after a review of imaging studies. This would suggest that a clinically significant association is highly unlikely.
Conclusion
This observational study suggests that diastasis recti, as defined anatomically (and by implication rectus divarication), is a common finding both among older male patients without AAA and among individuals with demonstrated AAAs in excess of 55 mm. No significantly increased prevalence of diastasis recti was apparent among patients with AAA when compared with nonaneurysmal controls. These results do not support the proposition that patients with rectus divarication should be targeted with screening for the presence of AAA.
Footnotes
Acknowledgments
We wish to acknowledge Dr. Elisabeth Wells, Department of Biostatistics, University of Otago, for her assistance with the statistical analysis.
Financial disclosure of authors and reviewers: None reported.