
Abstract
Prolonged cycling has previously been associated with external iliac artery stenosis, termed “cyclists' iliac syndrome.” However, no association between external iliac vein stenoses and cycling has been previously described. We describe a unique case of a 70-year-old cyclist presenting with an iliofemoral deep venous thrombosis owing to an external iliac vein stenosis. This is the first case of a potential association between cycling and iliac vein stenosis. Further study and follow-up will be required to assess whether angioplasty and stenting is the optimal method of therapy for iliac vein stenoses owing to cycling.
External iliac vein stenoses can cause iliofemoral deep venous thrombosis (DVT). 1 Pelvic collaterals develop poorly around external iliac vein stenoses and therefore are more prone to develop DVTs. 2 The two most common causes of iliac vein stenosis are DVT within the iliac vein and malignancy. Other rare conditions include May-Thurner syndrome, 3 giant ovarian tumors, 4 massively distended bladder, 5 pelvic irradiation, 6 cystic adventitial disease of the vein, 7 and prolonged femoral vein catheter insertion. 8 We report a unique case of a 70-year-old gentleman who presented with an external iliac vein stenosis and iliofemoral DVT presumably owing to repetitive microtrauma from cycling.
Case Report
A healthy 70-year-old Caucasian male presented with a 3-day history of a painful, swollen left leg. The swelling started after an intense 3 days of cycling, averaging 60 miles per day. At presentation, the patient complained of redness and swelling extending from his left ankle up to his groin, which had remained fairly constant over the 3 days before presentation. He denied any chest pain, progression of the swelling or redness, or previous episodes of leg swelling.
He was a type 2 diabetic and was treated for hypertension. The patient had no history of a hypercoagulable disorder, cancer, trauma, prior catheterizations, or pelvic irradiation. Forty years previously, he had fractures of his right tibia, left clavicle, and multiple ribs after falling off his bike. His only surgical history was the repair of these tibial and clavicular fractures. The patient denied having had a DVT previously. The patient was taking metformin, metoprolol, lisinopril, and hydrochlorothiazide at presentation. The patient denies taking any antiplatelet agents or statins or any performance-enhancing drugs. He denied any family history of clotting disorders and any alcohol or tobacco abuse. He estimated that he cycled approximately 50 to 80 miles/day but was never a competitive cyclist.
On examination, he appeared well. His vital signs were normal, as were his cardiac, respiratory, and abdominal examinations. He had left lower extremity pitting edema from his left ankle up to his groin. His skin was erythematous over areas of swelling. Both feet were warm, with good, equal capillary refill. Dorsalis pedis and posterior tibialis pulses were palpable in both lower limbs. The patient lacked any brawny edema, ulcerations, varicosities, or stasis dermatitis suggestive of long-standing venous hypertension to the limb.
The patient's admission hematologic and coagulation parameters were normal, without elevations of his urea or hematocrit. Neither serum tumor markers nor a hypercoagulable evaluation was performed. Ultrasonography was performed, revealing a left femoral DVT stretching from the inguinal ligament to the calf. The patient was then admitted for treatment and started on a heparin drip (5,000 U bolus, then 18 U/kg/h), with heparin levels measured to maintain the therapeutic anticoagulant effect.
Computed tomography (CT) of the abdomen, pelvis, and lower extremities with contrast was then performed, which revealed a circumferential filling defect of the lumen of the left popliteal vein extending proximally into the left external iliac vein. However, no common iliac vein thrombosis was visible. There was no evidence of any extrinsic compression of the left iliac venous system (Figure 1). The arterial system of the left lower extremity was normal. There was no evidence of pulmonary embolus or malignancy on the CT scan; moreover, there was no evidence of DVT in the contralateral limb on duplex ultrasonography or CT.
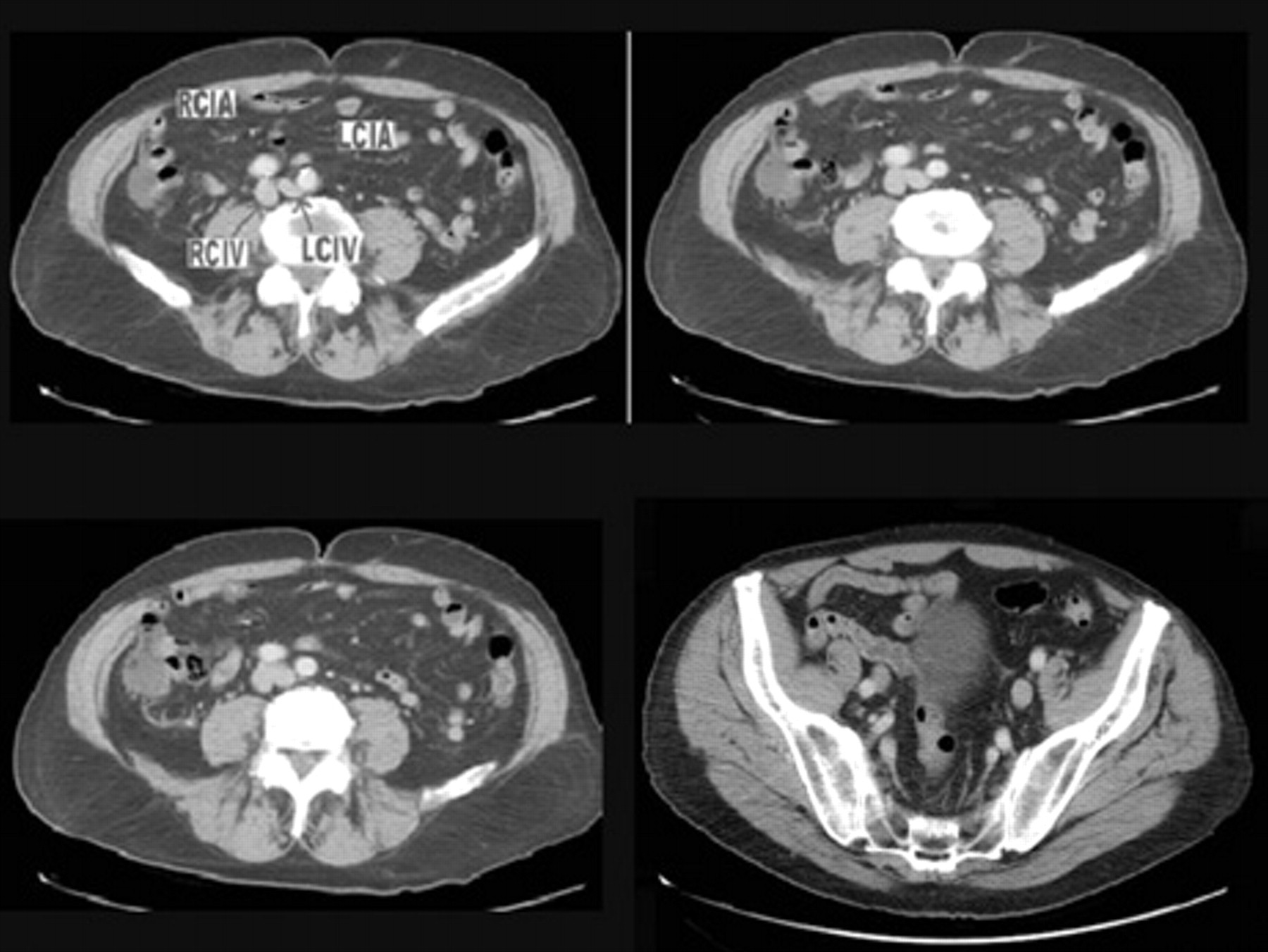
Ascending series of computed tomographic (CT) images excluding extrinsic compression by demonstrating an uncompressed left common iliac vein (LCIV). No other sources of external compression are found on the CT scan. No stenosis of the external iliac vein was appreciated by CT scan. LCIA = left common iliac artery; RCIA = right common iliac artery; RCIV = right common iliac vein.
The patient was counselled that therapeutic options included systemic anticoagulation alone versus thrombolysis in conjunction with systemic anticoagulation. Despite the heightened risk of bleeding complications because of his age, the decision was made to pursue catheter-directed thrombolysis owing to the improved venous patency and reduced valvular reflux after thrombolysis. 9 The next day, the patient was scheduled for catheter-directed thrombolysis. Venography during the procedure confirmed a diagnosis of left lower extremity DVT (Figure 2). A 50 cm multisidehole Uni-Fuse catheter (AngioDynamics Inc., Queensbury, NY) was inserted into the left popliteal vein with the patient in the prone position. The catheter was positioned through the thrombus in the external iliac and femoral veins, and a 2 mg bolus of alteplase was administered. This was maintained by a 0.5 mg/h infusion. The patient was also placed on a 500 U/h infusion of heparin through the sheath. No temporary inferior vena cava filter was placed. The patient tolerated the procedure without complications.

Venogram showing a 4.2 cm long clot (A) in the femoral vein and a stenosis in the external iliac vein (B).
After an uneventful night, left lower extremity venography and inferior vena cavography were performed the following day. These showed that the left superficial femoropopliteal vein had successfully responded to the thrombolytic therapy and was now widely patent with minimal residual thrombus. However, 2 cm above the inguinal ligament, a long, high-grade stenosis of the left external iliac vein was more easily visualized (Figure 3A).

A, Stenosis of the left external iliac vein post-thrombolysis, prestenting. B, Deployment of the Protege stent following unsuccessful balloon angioplasty. C, Completion venogram showing excellent flow through the stent.
The external iliac vein was serially dilated using a 6 mm, followed by an 8 mm, balloon. The stenosis remained, so the vessel was stented with a 10 mm × 8 cm eV3 Protege stent (Plymouth, MN). The stent was then postdilated with an 8 mm balloon, with an excellent angiographic result (Figure 3, B and C). Aspirin therapy was initiated to prevent bare metal stent thrombosis. The warfarin was given for the treatment of the DVT as per American College of Chest Physicians guidelines. 10
The operative and postoperative periods were uneventful, with the patient tolerating the procedure well. Vital signs were stable throughout the duration of his 3-day inpatient stay. He was discharged on hospital day 3 with good distal pulses, ambulating normally without pain. He was continued on warfarin, enoxaparin, and aspirin, as well as thigh-high compression stockings.
At the 1-month follow-up, the patient was free of left lower extremity swelling and erythema. Repeat ultrasonography was negative for thrombus. The patient had been counselled against further cycling as there was a risk of falling and injuring himself more severely owing to his warfarin administration; moreover, there was a risk of recurrent stenosis with stent fracture. The patient was adamant, however, that he had to return to riding his bike, although now he avoids long distances. The plan was to continue the warfarin for 3 months and the aspirin for the remainder of his life.
Discussion
Endurance athletes may suffer from a collection of conditions termed “nontraumatic vascular complications.” This includes iliac artery endofibrosis, stenosis, dissection, or kinking in flexion. Similar mechanisms may result in chronic damage to the external iliac vein, although no prior report has described an association between cycling and venous injury. Cyclists' iliac syndrome predominantly affects top-level athletes. The arterial stenosis develops secondary to endofibrosis (intimal hyperplasia) of the vessel, resulting in a beaded, stenotic appearance on angiography. This pathophysiologic process is presumed to occur owing to the aerodynamic position a cyclist adopts that causes high blood flow in this particular artery, which supplies the lower limbs. 9 Arteriography, sometimes with the patient assuming a crouched posture, is still required for diagnosis as other modalities, although promising, are less reliable at eliciting hemodynamically significant stenosis. 11,12
Two mechanisms may explain the damage sustained to the vein by cycling. First, similar to the artery, external iliac venous endothelial injury can occur from high venous flow. Second, compression or damage to the vein owing to the crouched body position and repetitive motion of cycling may result in chronic, repetitive compression against the inguinal ligament. These mechanisms could potentially convert the normally antithrombogenic endothelium to become prothrombotic by stimulating the production of tissue factor, fibronectin, and von Willebrand factor. 13
The patient had no risk factors for DVT other than age. Moreover, the patient did not have any evidence of dehydration on his admission laboratory tests. It has been reported that 80% of limbs with iliofemoral DVT have underlying extrinsic iliac compression-type lesions, 14 which were also excluded in this case. It is also possible that the patient may have suffered from a recurrent DVT from a scarred vein from a prior DVT; however, the patient lacked any history of a prior DVT or any sequelae of chronic venous hypertension to the left limb. Given that there was no specimen, histologic examination and definitive diagnosis were impossible. Etiologies other than cycling-induced repetitive microtrauma are well excluded by the history and physical examination. Furthermore, the appearance of the lesion on a venogram is consistent with the 5 to 6 cm stenoses found in the external iliac arteries of patients suffering from cyclists' iliac syndrome. 15
Conclusion
In summary, this case report describes a patient with an external iliac vein stenosis that appears to have been caused by vigorous cycling. This patient was treated by thrombolytic therapy followed by angioplasty and stenting of an external iliac vein stenosis discovered during treatment. Although external iliac vein stenoses are not well described, it appears that there is also a correlation between external iliac vein injury and cycling. Further patient follow-up will help determine whether balloon angioplasty and stenting represents the optimal method of managing cycling-induced iliac vein stenoses.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.