
Abstract
The value of emergency endovascular aneurysm repair (EVAR) in the setting of ruptured abdominal aortic aneurysm remains controversial owing to differing results. However, interpretation of published results remains difficult as there is a lack of generally accepted protocols or standard operating procedures. Furthermore, such protocols and standard operating procedures often are reported incompletely or not at all, thereby making interpretation of results difficult. We herein report our integrated logistic system for the endovascular treatment of ruptured abdominal aortic aneurysms. Important components of this system are prehospital logistics, in-hospital treatment logistics, and aftercare. Further studies should include details about all of these components, and a description of these logistic components must be included in all future studies of emergency EVAR for ruptured abdominal aortic aneurysms.
Keywords
Emergency endovascular aneurysm repair (eEVAR) has been advocated by some as a better way than open repair (OR) to treat patients with ruptured abdominal aortic aneurysms (RAAAs) provided that they have suitable anatomy. Numerous single-center reports, collected series, and meta-analyses have observed lower mortality and morbidity after eEVAR than after OR. However, in some of these reports, EVAR has been used on more stable or otherwise more favorable patients. Moreover, some controlled series have shown no superiority for EVAR treatment of RAAA patients. The value of eEVAR in the RAAA setting remains controversial.
It is our belief that many factors contribute to the differing results that have been observed for eEVAR in the treatment of RAAAs. Institutional logistics is probably one of the most important of these factors and may even outweigh patient selection, differences in management strategies, and technical factors, which also contribute to outcome differences. We have previously described our approaches to these latter three factors and suggested their importance in achieving good results with the eEVAR treatment of RAAAs in large institutional series. 1–3 The purpose of the present article is to describe one logistic approach in a single institution that has achieved excellent outcomes in more than 100 RAAA patients. 1 This logistic approach is only one of many that are possible. However, this approach may be useful to others seeking to optimize their results with the eEVAR treatment of RAAAs. This logistic approach includes staffing, equipment, institutional geography and transport issues, endovascular disposable supplies, stocking of necessary endograft components, and standard operating procedures (SOPs). Obviously, all parts of this approach must be combined with other aforementioned optimal management strategies and technical considerations 1–3 to achieve the best possible patient outcomes.
Standard Operating Procedures
In the industrial setting, it is generally accepted that SOPs help minimize production failures and communication problems. Recently, it has also been accepted that SOPs in the form of clear reporting standards, algorithms, and protocols also improve the outcomes of medical treatments. This applies particularly to the management of patients with RAAAs because of the involvement of many different specialties (eg, emergency staff, anesthetists, surgeons, and radiologists), the stress of involved staff members, and limited time to make correct decisions. 4–6
SOPs for the management of patients with acute aortic lesions (including RAAAs) must consider the whole process from the first contact (external telephone call from emergency staff or referring hospital) to the discharge of the patient (Figure 1). In addition, clear algorithms for the long-term follow-up must be defined (Figure 2).
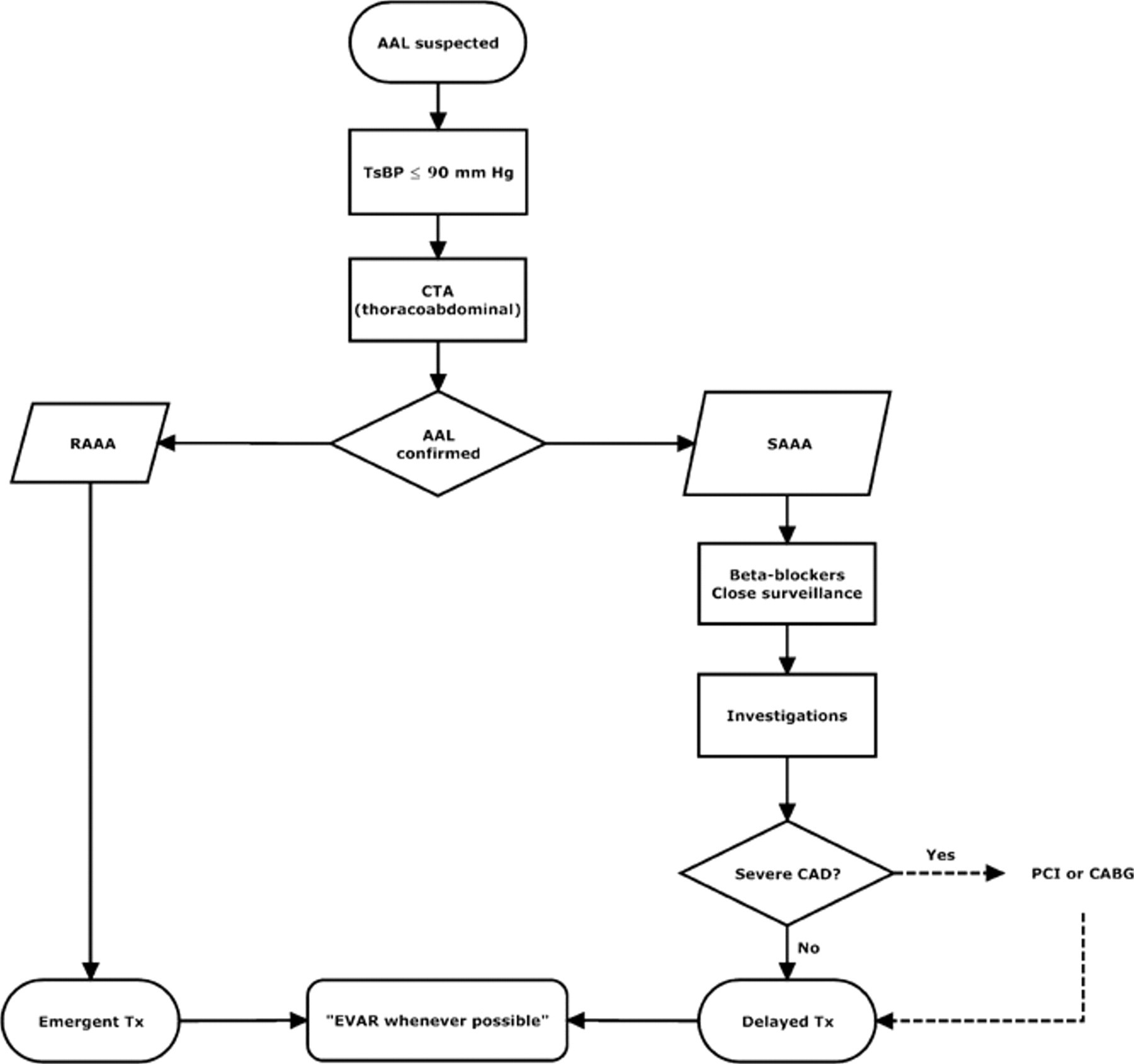
Diagnostic and treatment algorithm for acute aortic lesions. AAL = acute aortic lesion; CABG = coronary artery bypass graft; CAD = coronary artery disease; CTA = computed tomographic angiography; EVAR = endovascular aneurysm repair; PCI = percutaneous coronary intervention; RAAA = ruptured abdominal aortic aneurysm; SAAA = symptomatic abdominal aortic aneurysm; TsBP = target systolic blood pressure; Tx = treatment.

Endovascular aneurysm repair (EVAR) aftercare algorithm. ABI = ankle-brachial index. ASA = acetylsalicylic acid; CTA = computed tomographic angiography; FUP = follow-up; OA = oral anticoagulation (warfarin); XR = x-ray.
Prehospital Logistics
When the treating hospital is contacted initially by referring physicians, it is most important to ask whether the patient is hemodynamically stable and whether the systolic blood pressure is above or below 90 mm Hg. It also has to be determined whether the patient has received vasoactive medication and/or intravenous fluids (electrolyte solutions or blood). Advice is then given to stop all fluid administration and to actively lower the blood pressure below 90 mm Hg (preferably with a beta-blocker), if possible. With this so-called “hypotensive hemostatic approach,” 7 bleeding will be minimized and further bleeding during transportation may be avoided. Moreover, coagulation problems will be minimized because of less blood loss. One misconception is that RAAA patients have to be stabilized and transfused before transportation. As in trauma management, 8 a “scoop and run” tactic, preferably by helicopter, is suggested after explanation of the hypotensive hemostatic approach.
While waiting for the patient's arrival, an interdisciplinary team consisting of a dedicated vascular surgeon, a radiologist, an anesthesiologist, and a specialized scrub nurse is quickly mobilized and the endovascular emergency kit (Figure 3 and Table 1), also containing a balloon for transfemoral (supraceliac) aortic occlusion, is transferred to the shock room in the emergency department. A team leader, usually the vascular surgeon, is appointed.

Simple emergency endovascular aneurysm repair (EVAR) kit containing the most used endovascular tools and an aortic occlusion balloon. Endograft components are taken from the regular in-house stock as needed (see Table 1 for the contents of this kit).
EVAR Emergency Kit At Our Institution*
*The composition of a distinct emergency EVAR kit helps avoid mistakes and speeds up management.
Treating Hospital Logistics
Patient Management
On arrival in the shock room of the emergency department, a simple, quick, surgical and anesthetic evaluation and initial treatment are carried out in which a brief history is obtained and a physical examination is conducted, intravenous access lines are inserted with one or two 14-gauge peripheral cannulas, and a radial artery line is placed. Testing of the patient's coagulation profile should also be part of the rapid routine laboratory (blood) evaluation to avoid delay in correcting coagulation factor deficits. Immediately thereafter, the patient undergoes a rapid thoracoabdominal computed tomographic angiogram (CTA) unless one is provided by the referring institution.
Should the patient become hemodynamically unstable at any time, a large sheath (> 14F) and a transfemoral balloon are inserted percutaneously under local anesthesia and fluoroscopic control. 9 CTA may be performed with the occlusion balloon in place. The CTA can and should be done within 10 to 20 minutes.
Immediately after the CTA, anesthetic preparation (central venous line placement and insertion of tubes in the bladder and stomach) is carried out. Simultaneously, the specialized surgeon and radiologist analyze the thoracoabdominal CTA and decide on the best treatment option (endovascular or open).
Diagnostics
CTA is the gold standard for diagnosis and planning of the optimal treatment of abdominal aortic aneurysms in elective patients. In the emergency setting, the possibly negative effect of the short time delay to obtain a CTA is offset by the advantages of the information obtained, although this is still controversial. However, it has been shown that only a minority of RAAA patients (12%) will die within the first 2 hours after hospital arrival even if not treated. 10 Currently, many institutions (including our) have rapid access to a CT scanner, with results available within 10 to 20 minutes. Recently, this approach has been shown to exert no negative effects on the outcome of RAAA patients. 1,11 However, some groups without rapid CTA access have shown that in certain patients, it might be feasible to go directly to the operating room and carry out eEVAR using only fluoroscopic arteriography for decision making (OR vs EVAR) and endograft measurements. 7
A separate emergency shock room close to a CT scanner and the operating theater constitutes the ideal infrastructure. In most institutions, however, the radiology department is at some distance from the emergency department. Although most of the patients will be stable enough for short in-hospital transports, some may be excluded from CTA before eEVAR because of transportation delays.
Anatomic suitability for EVAR is better defined with modern 64- or 128-channel multidetector CTA than with older 4- or 16-channel CT scanners. It is crucial to have an up-to-date and fast workstation that allows quick reconstruction and analysis of the images taken when working with modern high-resolution CT scanners. The CT scanner and workstation should be accessible to the treating physicians and operable at all times.
EVAR Experience
Volume-outcome relationships have been described as a predictor of outcomes for the management of several vascular pathologies. For endovascular treatment of RAAAs, no such relationship has yet been defined. However, in a recent study, Forbes and colleagues considered whether an institution's prior endovascular experience influenced the learning curve of subsequent surgeons for elective EVAR. 12 Optimal results were achieved following 10 to 20 EVAR cases for a surgeon introduced to EVAR when the institution had already gained experience, as opposed to 60 cases in the initial experience at their institution. Although transfer of this knowledge to the emergent setting is difficult, it might be postulated that an institution setting up an eEVAR service needs to have considerable EVAR experience and that individual surgeons in this institution should have carried out at least 40 elective EVAR procedures before starting eEVAR cases. If only aortouni-iliac or femoral endografts will be used, a personal experience of less than 40 procedures may be adequate for optimal results.
Interdisciplinary Team Approach
Emergency endovascular treatment of RAAAs is ideally carried out by an interdisciplinary team of vascular surgeons, radiologists, anesthetists, and specialized scrub nurses. However, good results are reported even in institutions where RAAAs have been treated solely by dedicated vascular or general surgeons. 13
Facilities
Most of the RAAA patients anatomically suitable for eEVAR can be adequately managed under fluoroscopic control in a normal operating room with portable C-arm fluoroscopy. However, in some obese patients with large retroperitoneal hematomas, such imaging may be inadequate to visualize the renal arteries clearly. The ideal solution to this problem would be a hybrid operating room with fixed ceiling-mounted fluoroscopy, which is not available in most institutions. At our institution, such patients are transferred from the shock room of the emergency department to an angiography suite with better radiologic equipment whenever possible. This suite is 15 minutes away but is equipped also for open surgical procedures.
Permanent easy access to intensive care unit beds is a prerequisite for the treatment of RAAA patients. Although patients managed by eEVAR usually require less intensive care (workload and length of stay), this advantage might be counteracted by an increased patient load owing to RAAA patients.
Human Resources
The temporary lack of properly skilled human resources has been responsible for the exclusion of anatomically suitable RAAA patients from eEVAR. 6 Accordingly, some authors emphasize the importance of having trained staff 24 hours a day, 7 days a week. 4,5
At our institution, fully trained staff are available at all times. This staff consists of fully trained endovascular scrub nurses, surgeons, interventional radiologists, and cardiovascular anesthesiologists. In case of an RAAA emergency, the group can be ready to intervene within 30 minutes after the first call.
Stocking and Supply Issues
The lack of an adequate stock of endograft components has been a critical issue in the exclusion of RAAA patients anatomically suitable for eEVAR. 4 High-volume EVAR clinics (such as ours) already have a large stock of bifurcated endograft components that should suffice for the needs of an eEVAR service. This stock should also include aortouni-iliac endograft components for patients with only one inaccessible iliac artery system. Table 1 shows the eEVAR kit used at our institution. During our 11 years' experience, this kit has been used in treating up to 88% of RAAAs by eEVAR in recent years. Low-volume EVAR clinics might have in their RAAA emergency kit only aortouni-iliac or femoral components, which would mean a smaller stock with a relatively lower cost than also stocking bifurcated systems.
Endograft components are a major cost factor in the emergent endovascular treatment of RAAAs, especially when all options (infra- and suprarenally anchored systems, bifurcated and aortouni-iliac endografts) are to be offered. However, there are several ways to reduce costs. One method would be to have an arrangement with industry to have an endograft stock on consignment and pay only for the components after they are used. If this is not possible, an emergency kit with an aortouni-iliac or femoral system with only a few components should suffice to treat most RAAAs by EVAR. 2,14
Education
Paramedical and medical staffs caring for RAAA patients must be regularly educated and trained so that they know well the defined and accepted SOPs and algorithms. Every center treating RAAAs should implement educational programs for external staff (such as emergency medical teams, general practitioners, and personnel from referring hospitals) and internal staff (emergency department personnel, anesthesiologists, radiologists, surgeons, nurses, and other technicians).
In addition, academic lectures should be instituted for future paramedical and medical staff members to sensitize them to the entity of RAAAs.
Aftercare
Long-term follow-up for endovascular management of non-RAAAs is mandatory and its need unchallenged. 15,16 These requirements also hold for EVAR-treated patients with RAAAs, even though eEVAR may be regarded as a bridge to definitive OR by some authors. 17 However, clear algorithms for the aftercare of RAAA patients are still lacking, and various groups adhere to quite different protocols. During our 11 years' experience, we have refined the aftercare of EVAR patients including those with RAAA that takes into account the size and morphology of the aneurysm and the findings of the CTA performed immediately after the intervention (see Figure 2).
Evidence to Date
Complete implementation of all of the above-mentioned considerations has proven to be beneficial at our institution. In the largest published series of 102 RAAA patients, 30-day mortality was only 14% despite the inclusion of hemodynamically unstable patients (19 of 102; 19%). 1 Moreover, Veith and colleagues recently reported the results of 13 centers where 680 RAAA patients had been treated by EVAR. 3 By adhering to similar guidelines, the 30-day procedural mortality was 20% (134 of 680) in this collected experience.
Conclusion
The logistics of treatment in RAAA patients represents a multilevel approach to various conditions linked with the (endovascular) management of RAAAs. Institutional, staffing, preparation, supply stock, educational, and financial factors play a key role when setting up a dedicated eEVAR service to treat the majority of RAAA patients in a less invasive manner. Any detail omitted weakens the whole system and will worsen an institution's treatment outcomes for this condition. Clearly, logistics must be included as a major descriptor in all future studies of eEVAR for RAAAs.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.