
Abstract
The surgical management of aortic aneurysms in kidney transplant patients is a difficult clinical scenario where preservation of the kidney allograft during aortic cross-clamping is paramount. We describe a novel technique for renal protection during abdominal aortic aneurysm repair with in situ oxygenated pump perfusion of the transplanted kidney. A percutaneous approach is used for common femoral artery and vein cannulation and a cardiopulmonary bypass circuit to provide retrograde oxygenated pump perfusion to the transplanted kidney. This technique allows adequate kidney perfusion during warm ischemia and minimizes morbidity by using a percutaneous access technique.
As the long-term durability of kidney transplantation improves, surgeons are increasingly required to manage the late complications associated with arteriosclerotic vascular disease in transplant recipients. Kidney transplant recipients are often at heightened risk for atherosclerosis-related conditions secondary to associated hypertension, diabetes, and prior hemodialysis. 1,2 The management of abdominal aortic aneurysms (AAAs) in kidney transplant patients is a particularly difficult scenario given the demand for preservation of the precious kidney allograft. With favorable anatomy, endovascular repair of AAA is feasible in these patients. 3 However, in patients with compromised renal function, the contrast burden during the endovascular procedure and frequent surveillance requirements are detrimental. This patient population often requires open AAA repair, during which renal protection strategies are warranted. We describe AAA repair in a patient with a kidney allograft using a novel renal protection strategy.
Case Report
The patient was a 67-year-old male with a history of end-stage kidney disease secondary to hypertensive nephrosclerosis and an asymptomatic 5.5 cm infrarenal AAA. He also had a history of hyperlipidemia and coronary artery disease, which was previously treated with coronary artery bypass grafting. He was maintained on hemodialysis for 3 years prior to transplantation. He received a living-unrelated (wife) donor kidney transplant. The kidney allograft was placed in his right lower quadrant in the standard fashion with iliac artery and vein anastomoses. The transplanted kidney had been functional well before he presented to us for aneurysm repair. Prior to AAA repair, his baseline creatinine was 1.7 mg/dL.
His AAA was discovered incidentally during evaluation for kidney transplantation 3 years previously. At that time, the AAA measured 4.0 cm. The AAA was monitored with interval imaging and was noted to progressively increase in size. Prior to the decision for AAA repair, a computed tomographic angiogram was obtained and demonstrated a 5.5 cm fusiform AAA with a 2 cm infrarenal neck and no aneurysmal involvement of the iliac arteries (Figure 1). The patient was offered endovascular repair, but given the significant risks of contrast nephropathy to his transplanted kidney, the patient elected for open repair.
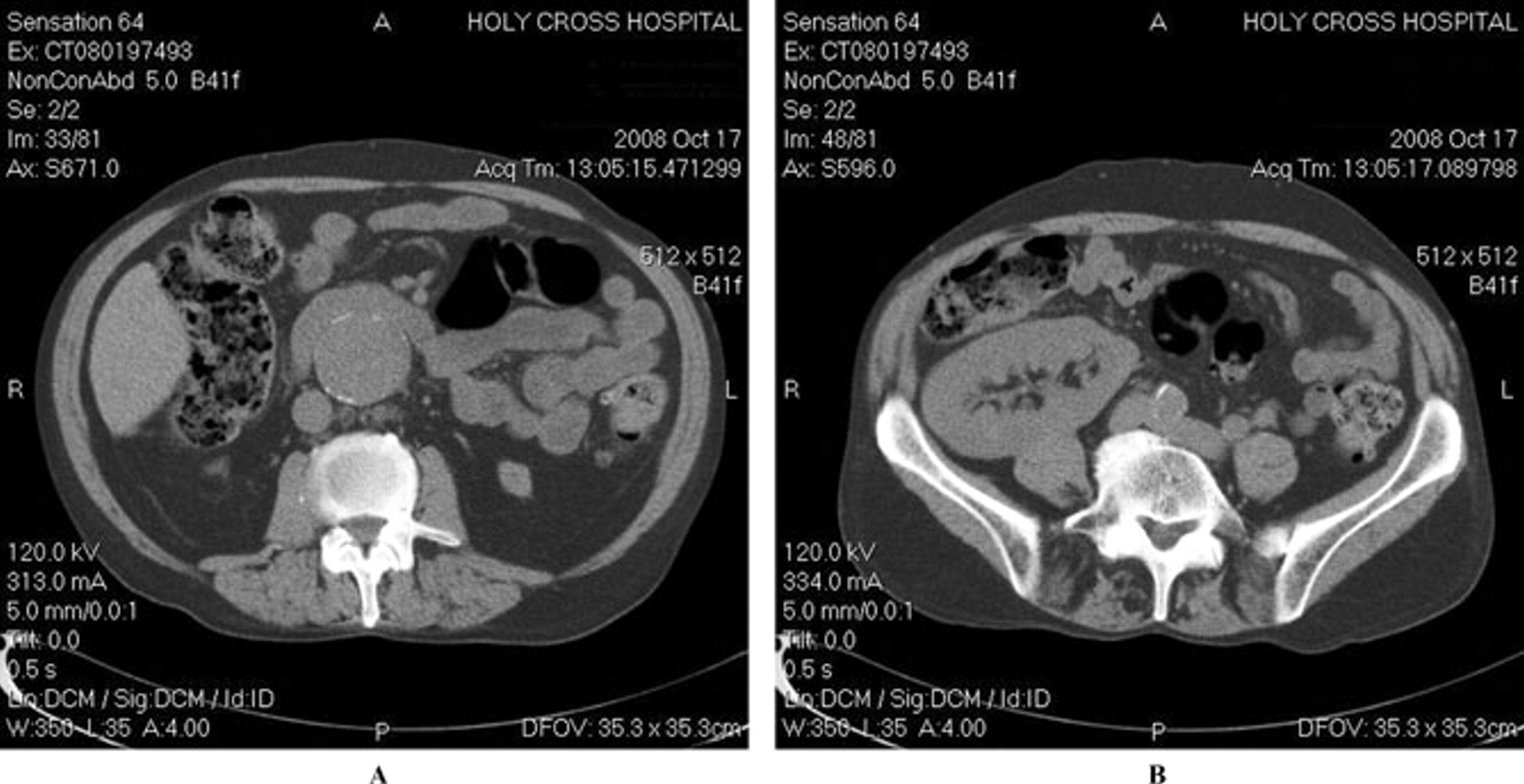
A, Preoperative computed tomographic (CT) scan showing an infrarenal abdominal aortic aneurysm. B, Preoperative CT scan showing a transplanted kidney.
The patient underwent open AAA repair with a 16 mm Hemashield interposition tube graft. The transplanted kidney was preserved during aortic cross-clamping with in situ oxygenated pump perfusion. Postoperatively, the patient recovered uneventfully. He was administered intravenous steroids until he was tolerating an oral diet, at which time his preoperative immunosuppressive regimen was reinstituted. He was discharged home on postoperative day 5 with a creatinine level of 1.6 mg/dL. He was seen at 1 year and was doing well, with stable renal function.
Technique
Percutaneous access of the right common femoral artery is gained with a 19-gauge needle, and an 0.035-inch wire is advanced into the right ileofemoral vessels. Two 6F Perclose ProGlide devices (Abbott Vascular, Abbott Park, IL) are placed at 30° angles in a “V” configuration and fired with the sutures in place for closure of access at the end of the case. The artery is dilated up a 16F arterial cannula for inflow from the pump oxygenator. Percutaneous access of the right common femoral vein is gained in similar fashion and a 16F venous cannula is placed.
The AAA is exposed using a transperitoneal approach. The patient is heparinized with 10 U/kg. The right common iliac artery is then occluded, and flow into the pump oxygenator is established and oxygenated blood is infused via the right iliac artery into the transplanted kidney (Figure 2).

Schematic showing perfusion of isolated transplanted kidney with oxygenated blood using a pump oxygenator. Inova Fairfax Hospital Pediatric Extracorporeal Membrane Oxygenation Circuit: 1 = CDI Venous Saturation Probe; 2 = Better Bladder Compliance Reservoir; 3 = pressure transducer (negative inlet pressure alarm); 4 = arterial roller-head pump (¼″ tubing); 5 = pressure transducer (premembrane, positive alarm); (6) Terumo Baby RX hollow fiber membrane oxygenator (Terumo, Ann Arbor, MI); 7 = CDI Arterial Blood Gas Analyzer (continuous inline); 8 = pressure transducer (postmembrane, positive alarm); 9 = Sorin SIII Ultrasonic air bubble detector.
Prior to initiating pump flow, the system is primed with 350 mL lactated Ringer solution, 12.5 g of 25% mannitol, 125 mg of methylprednisolone, and 500 units of heparin sodium. Renal perfusion is initiated at 200 mL/min and gently increased to 375 to 400 mL/min during the case. Perfusion temperature is maintained at 35°C during the case. Activated clotting time assays are performed every 20 minutes and kept above 180 seconds.
The infrarenal aorta and left common iliac artery are now occluded and the aneurysm is opened. A 16 mm Hemashield interposition graft is sutured in place with 3-0 polypropylene. On completion, flow is established through the interposition graft first into the left iliac artery and then into the right common iliac artery to prevent embolization to the kidney allograft.
Perfusion with the pump oxygenator is discontinued and the cannulas are removed. The ProGlide sutures on the femoral artery are activated and the access site is closed. Manual hemostasis is applied over the femoral vein. Heparin is reversed with protamine and blood is reinfused from the cell saver. The patient is closed in the standard fashion.
Discussion
The surgical management of aortic aneurysms in kidney transplant patients is a complex clinical situation where preservation of the kidney allograft during warm ischemia is key. Although AAA repair with no adjunctive protection of the transplanted kidney has been described, 4 postoperative renal dysfunction is common and may predispose the patient to early allograft loss. In patients with impaired baseline transplant function or difficult surgical anatomy, renal protection measures are mandatory. We describe a novel method for transplant kidney preservation during AAA repair using a percutaneous approach.
We employed in situ oxygenated pump perfusion of a transplanted kidney as an adjunctive renal protection strategy in a patient with baseline transplant dysfunction. The common femoral artery and vein were cannulated using a percutaneous approach. A cardiopulmonary bypass circuit was used to deliver retrograde oxygenated blood to the kidney allograft at 350 mL/min. There were no complications related to the percutaneous access site, and the patient was discharged with a creatinine level at baseline.
A similar technique using oxygenated pump perfusion of a transplanted kidney during AAA repair has previously been reported; however, an open femoral cutdown was described. 5 The use of a percutaneous approach for the femoral artery and vein access reduces the potential morbidity of a groin incision. To our knowledge, this is the first report of a percutaneous approach for in situ oxygenated pump perfusion of a transplanted kidney during AAA repair.
Various other renal protection methods have been described in the literature. These include in situ renal perfusion with cold (4°C) lactated Ringer solution through the common iliac artery, 6 temporary axillofemoral bypass, 7 and general hypothermia. 8 Each of these methods is associated with additional surgical morbidity risk. In situ renal perfusion with cold (4°C) lactated Ringer solution requires exposure of the transplanted kidney for application of sterile ice around the kidney. Dissection of the transplanted kidney may lead to inadvertent injury to the organ and is disadvantageous. Temporary axillofemoral bypass requires an additional operation with associated morbidity, and sufficient general hypothermia for adequate renal protection is difficult to achieve. Use of a nonoxygenating biopump (eg, Bio-Medicus) is not recommended as the transplanted kidney would not be perfused with oxygenated blood.
Endovascular repair of AAA in patients with kidney transplants has also been described. 3 However, the contrast burden during the endovascular procedure and frequent surveillance requirements, often using contrast-based imaging, are detrimental, particularly in a patient with compromised baseline kidney function. 9,10 In addition, some aortic aneurysms are not amenable to endovascular repair for unfavorable anatomic conditions.
Conclusion
We describe a novel technique for transplant kidney preservation during AAA repair. A percutaneous approach for in situ oxygenated pump perfusion of the kidney allograft provides adequate renal protection during aortic cross-clamping with minimal additional procedural morbidity.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.