
Abstract
Background:
The simulated Doppler blood flow signals are widely used to assess the performance of the clutter filters for removing wall components while reserving low-velocity signals scattered from physiological blood flow approaching the inner vessel-wall injured by a stenosed lesion.
Objective:
By simultaneously taking into account the natural attributes of the Doppler equipment, blood flow as well as vessel wall of pulsatile carotid arteries with a stenosis, a computer simulation method is presented to produce the compound Doppler ultrasound blood flow signals.
Methods:
The in-phase and quadrature (I/Q) axial as well as radial blood flow signals are simulated by superposing a series of cosine functions regulated by the spectrograms estimated from the axial and radial velocity profiles firstly obtained through the solution of the incompressible Navier–Stokes equations, respectively. Meanwhile, the I/Q Doppler signals echoed from pulsatile near (anterior) and far (posterior) walls are reproduced based on their radial movements during a cardiac cycle. Ultimately, those confirmed quadrature signals are summed to generate the compound Doppler signals including the contribution from both blood flow and stenosed vessel-wall.
Results:
The compound Doppler ultrasound signals echoed from both axial and radial blood flows as well as vessel walls with obstruction grades of 0% (normal arteries), 10% and 25% are simulated respectively. The real signals from the left carotid artery with an approximately 10% stenosis degree are also collected for further assessing the believability of simulated versions.
Conclusions:
The simulated and clinical tests demonstrate that the proposed computer simulation method can produce compound Doppler signals with confirmed qualitative and quantitative characteristics resembled with the clinical versions, which could be used as an theoretical data source for evaluating the performance of the signal separation between pulsatile blood flows and vessel walls with mild stenosed-lesions.
Keywords
Introduction
Stenosis is one of the most common arterial illnesses, which can confine the blood vessels, and may give rise to elevated blood flow velocity and shear stress, degressive or subtractive pressure at the narrowest position of stenosis, as well as decreasing shear stress, flow separation, wall contraction or even collapse at the downside of the stenosis [1,2]. These may be the fundamental reasons for thrombus generation and plaque cap fracture directly leading to heart attack and apoplexy [3]. Therefore, it is important to pay close attention to the early and correct identification of the risk factors affecting the stenosis formation and development for diagnosis of cardiovascular diseases.
Doppler ultrasound technique is a noninvasive, dynamic and easily accessible means widely adopted in diagnosis of cardiovascular diseases by assessing and quantifying the dynamic behaviours of blood vessel walls and the conditions of pulsatile blood flow. Some studies [4,5] have been carried out to acquire the acceleration as well as deceleration of blood vessel wall for noninvasively estimating the dynamic compliance of vascular substitutes as well as their pulsatile behaviour. It has been found that the obtained results can be used to reflect the degree of atherosclerotic changes in the vessel walls, which are benefit to conduct more detailed diagnosis of the arterial lesion.
While with the onset and development of cardiovascular lesions, the blood flow may be disarranged by atherosclerotic plaque attached to the inner membrane of vessel wall leading to the emergence of vortices or turbulence [6,7]. It seems reasonable to believe that more susceptive and exact inspection of the slight abnormal slowly-moving blood flow in proximity of the vessel wall could promote improvements in the diagnosis efficiency and medical outcomes. In recent years, a number of computational analysis and detection methods have been proposed to quantify blood flow distribution, involving that approaching the inner vessel-wall, to assess the wall shear rate (WSR) and the flow rate profiler (FRP) [8–13]. Because of the contamination of the low-frequency and great-amplitude clutters scattered from surrounding slowly-moving tissues (such as vessel walls), special clutter or wall filters for removing clutters from compound signals have been extensively researched [14–25]. In these studies, several wall removal approaches were presented, and their filtering performances were tested by employing compound Doppler signals achieved from either synthesis or simulation models.
The synthesis models [14–17] commonly employed the complex exponentials with a designated basic frequency and a corresponding phase shift superimposed by a random component with narrow band Gaussian distribution to synthesize mixed Doppler signals scattered from a random distribution of blood cells and the slowly-moving vessel wall passing through a sample volume. The synthesis models are limited to generate desirable simulation signals to test the capability of wall removing approaches because of insufficient consideration of the natural or physiologic attributes of the blood flow,artery walls as well as Doppler equipments. Several simulation approaches have been introduced [18–25] on account of the inherent features of blood flow, normal arteries (without stenosis) enclosed by the elastic tissue and ultrasound technique to produce compound Doppler signals. The composite simulated-signals present a similar form to those observed in Doppler instruments. The results also demonstrated that the simulation models ameliorated the believability and reality of compound simulation signals as they have controllable characteristics close to those obtained from clinical experiments. However, these simulation models mentioned above are restricted to produce the compound signals echoed from blood flow with only axial velocity component in healthy arteries. Therefore, it is necessary to simultaneously take into account the contribution of the both axial and radial blood flows due to the disturbance of the atherosclerotic plaque as well as pulsatile vessel walls when the study of the simulation mode is conducted to achieve the compound Doppler ultrasound signals from pulsatile carotid arteries with a stenosed lesion.
The aim of this paper is to present a computer simulation method to produce compound Doppler ultrasound signals scattered simultaneously from both blood flow and vessel wall of pulsatile common carotid arteries. To simulate the full in-phase and quadrature (I/Q) blood flow signals, the radial blood flow velocity distribution under the stenosis condition is obtained by an extension study from previous researches on the Doppler signal simulation of the axial blood flow [26,27] by solving the NSEs in view of the center velocity of a normal vessel and geometric characteristics of the stenosed vessel, and then, the signals are simulated by superposing a series of cosine functions regulated by the spectrograms estimated from the axial and radial velocity profiles, respectively. Meanwhile, the I/Q Doppler signals echoed from pulsatile near and far walls (close to and far away the ultrasound probe, respectively) are reproduced based on their radial movements during a cardiac cycle. Ultimately, the confirmed quadrature signals incorporating the moving information backscattered from both axial and radial flows as well as pulsatile vessel walls are summed to generate the compound Doppler signals with regard to a definite sample volume. Both of the simulated and clinical trials are carried out to examine the performance of the introduced simulation method.
The rest of this paper is constructed as follows. Section 2 concentrates on a detail description of the method to simulate compound Doppler signals from axial and radial blood flows, as well as pulsatile vessel walls with the gentle regional-stenosis, respectively. Section 3 treats the simulation and clinical experiments for evaluating the performance of the presented simulation method. The last covers the results, discussions and conclusions.
Methods
The geometric shape of a stenotic artery
The stenotic artery can be described as a sine-shaped tube fraction with a radially and axially symmetrical circular cross section, which is displayed in Fig. 1 and delineated as
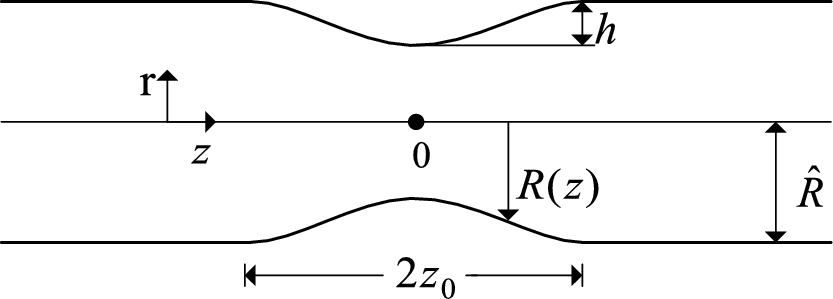
The geometric model of the artery with a stenosed lesion.
It is supposed that the pulsatile blood flow in the obstructed vessel fragment with a sine appearance is axisymmetrical, and exhibits the property of an incompressible Newtonian fluid. The momentum and continuity equations related to this pulsatile blood flow could be described by the linear NSEs [26] expressed as Eq. (2) under the cylindrical coordinate system where z stands for the longitudinal coordinate taking along the axis of the artery while r is the radial coordinate.
The relevant modulus (pressure, pressure gradient and velocities) could be expanded as complex Fourier series as follows due to the periodicity of blood flow:
Based on the axial and radial velocity profiles determined by Eq. (6), the corresponding theoretical blood flow spectrograms can be reckoned by employing the overall-distribution nonparametric estimation (ODNE) method [28] in which the power spectral density (PSD) of the Doppler blood signals comprises the contributions of all blood cells flowing through the sample volume (SV), which is separated into a series of basic volumes (BVs) in the axial and radial directions, respectively. The separation of the SV for estimating the theoretical spectrograms is displayed in the left of Fig. 2.

The division of the vessel lumen for the blood flow spectrogram calculation (the left) and the vessel wall for the simulation of the Doppler signal from the wall motion (the right).
Ultimately, the cosine-superposed method proposed by Mo [29] is employed to generate the complex quadrature axial (
In order to carry blood from heart to all parts of the human body, the cross-section area of the artery alters with blood pressure during the cardiac cycle. Due to the elastic feature of the vessel walls composed of monolayer cell and basement membrane, the near and far walls can be found to be expanded outwardly to maximum vessel diameter during the systole and rebounded slowly to the normal conditions during the final phase of diastole. The radial pulse of vessel wall also brings the frequency variation in Doppler ultrasound signals. The phase adaption related to the slowly-pulsing near and far nonlinear elasticity vessel walls can be written respectively as [25]:
The appropriate division of the vessel wall in the SV into a series of BVs along the ring-shaped circumference is carried out and displayed in the right of Fig. 2. Then the entire wall signal,
The composition of the blood and wall signals
The I/Q Doppler ultrasound signals including the moving information backscattered from both axial and radial blood flows as well as vessel walls of pulsatile stenosed-common carotid arteries are achieved by summing the obtained blood flow and vessel wall signals with respect to the determined sample volume by:
Experiments
To assess the performance of the presented simulation method, compound quadrature-Doppler ultrasound signals from the pulsatile axial as well as radial blood flow and vessel walls with various stenosis grades of 0% (normal arteries), 10% and 25% in the SV axially ranging from
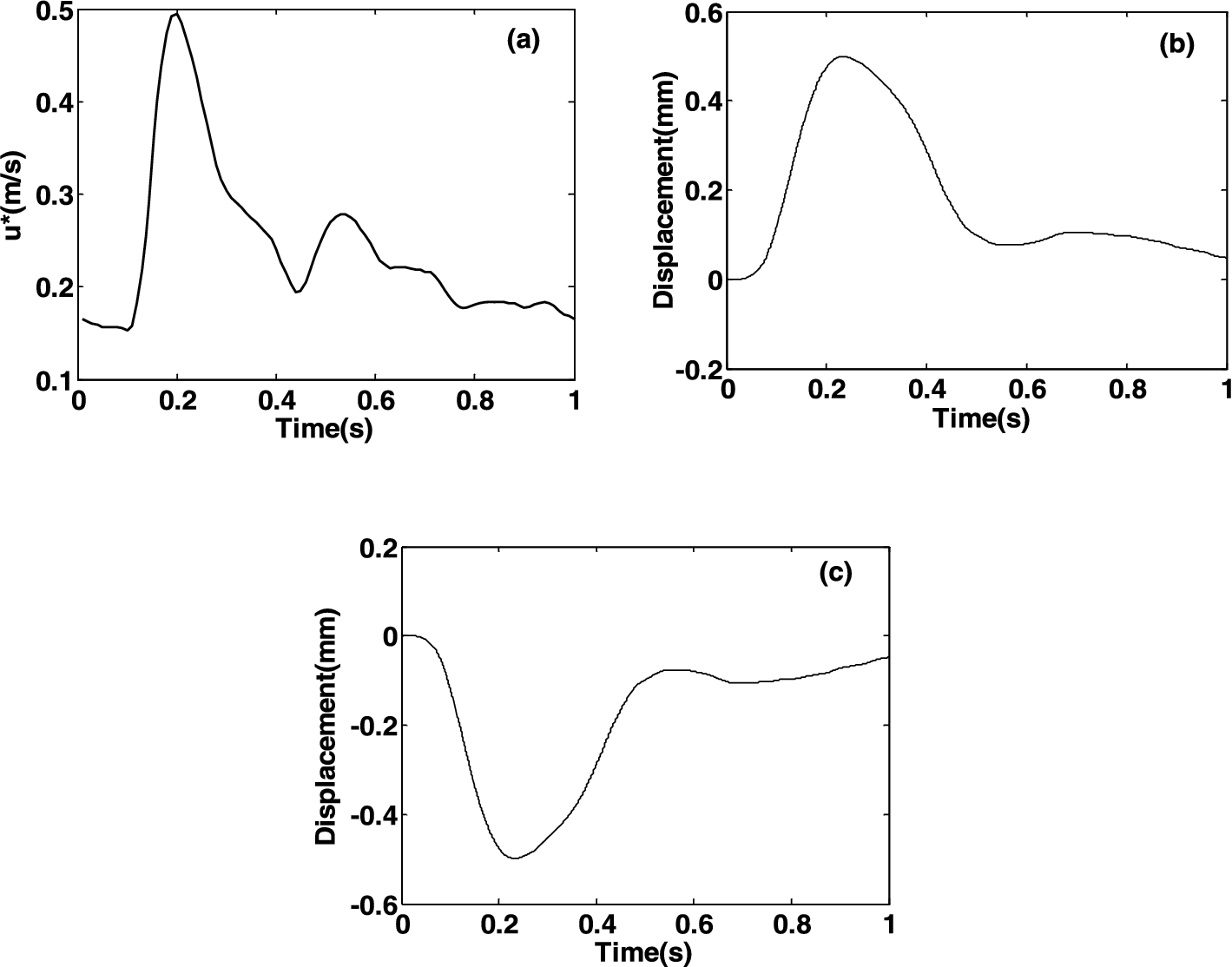
The waveforms of the axial centerline velocity waveform
In the experimental study, I/Q Doppler blood signals scattered from pulsatile axial and radial blood flow in the healthy vessel and stenosed vessels with obstruction grades of 10% and 25% axially located in
For further assessment of the proposed simulation method,the real signals from the left carotid artery with an approximately 10% stenosis degree determined previously by the CT and MRI are also collected in accordance with the ethical standards of the responsible committee on human experimentation. The compound I/Q Doppler ultrasound signals are firstly obtained from the determined male patient aged 55 years by using the continuous-wave Doppler blood flow detection instruments (VersaLab, Nicolet vascular Incorporated, CO, USA) with a 8 MHz transducer. The traditional vessel wall filter known as HPF is shut off to obtain the quadrature analog demodulation signals scattered from the pulsatile carotid arteries including both the blood flow and vessel wall. Then the corresponding digitized signals can be obtained by using an external sound blaster with two sampling channels inserted into a conveyable PC by an USB interface. The 22.5 MHz sample rate and 16 bit word length are used in digitization. The STFT-based spectrograms of the compound real signals and the signals extracted by using the HPF with cut-off frequency of 400 Hz (100 Hz intervals) are respectively achieved based on the same methods employed in the simulation experiments. The STFT-based spectrograms and spectra obtained from the real signals are compared with those derived in the simulation cases. All of the simulation and comparative experiments are implemented in Matlab 7.8 (The Mathworks, Inc., Natick, MA, USA).
As shown in Fig. 4(a)–(c), the velocity profiles of axial blood flow for the healthy artery (Fig. 4(a)) and artery with obstruction grades of 10% (Fig. 4(b)) and 25% (Fig. 4(c)) are respectively achieved according to Eq. (6) based on the symmetry axis (
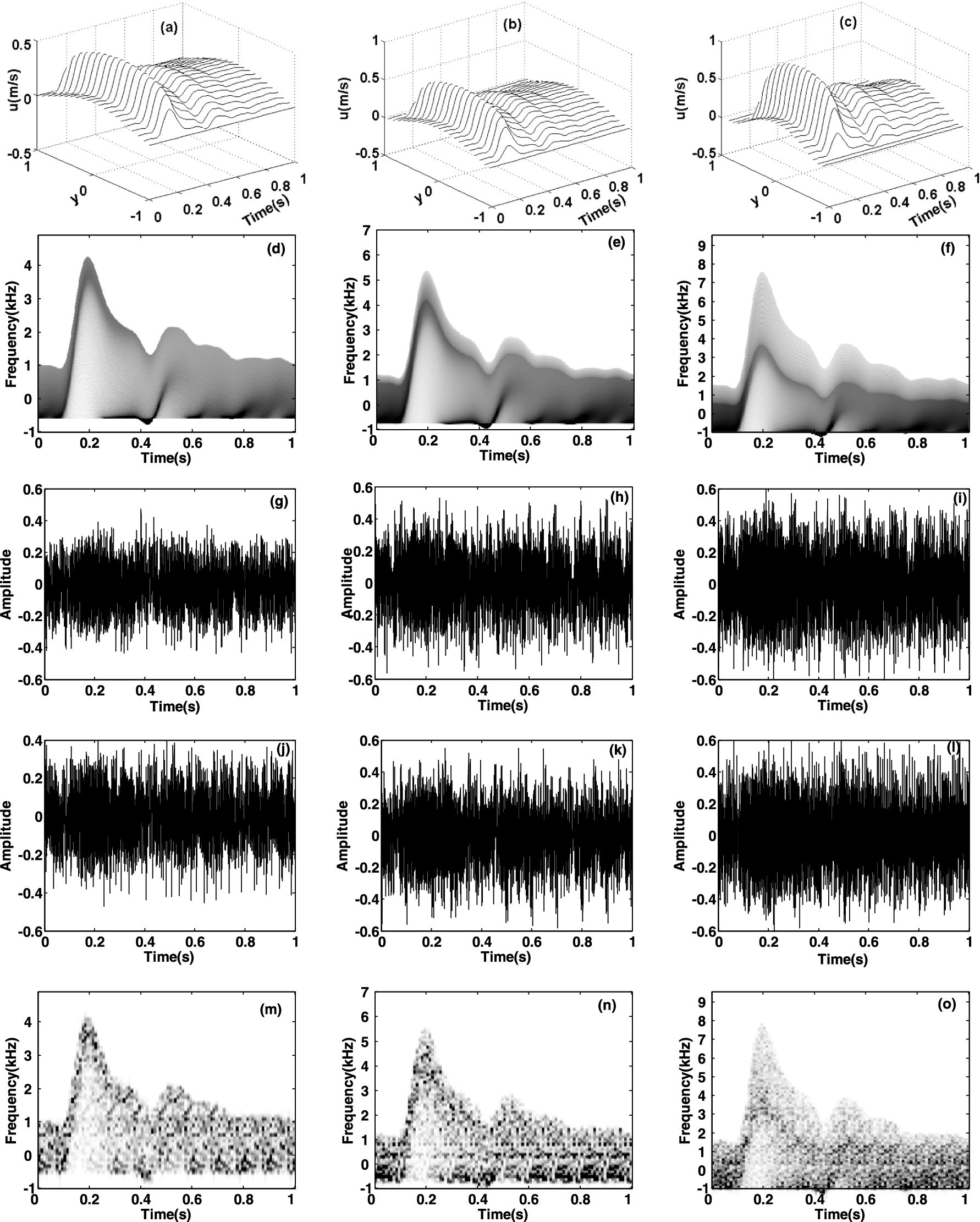
The velocity distributions (a)–(c), theoretical spectrograms (d)–(f), the simulated in-phase (g)–(i) and quadrature (j)–(l) Doppler signals, and their STFT spectrograms (m)–(o) of the axial blood flow signals in the normal vessel ((a), (d), (g), (j), (m)) and vessel with obstruction grades of 10% ((b), (e), (h), (k), (n)) and 25% ((c), (f), (i), (l), (o)) over the axial range from
The theoretical spectrograms of the axial blood flow in the SV with extent 20 mm centered on
Figure 4(g)–(l) show the in-phase (Fig. 4(g)–(i)) and quadrature (Fig. 4(j)–(l)) simulated Doppler signals echoed from axial blood flow in the artery with different obstruction grades of 0% (Fig. 4(g) and (j)), 10% (Fig. 4(h) and (k)) and 25% (Fig. 4(i) and (l)). All of them are stochastic allocation reflecting the time-varying nonstationary characteristic of axial blood flow and their distinctions are undoubtedly hard to be achieved. In order to evaluate their validities, their time-varying spectrograms are calculated by employing STFT with a 10 ms temporal window and exhibited in Fig. 4(m)–(o). The results show that STFT-based spectrograms present high consistencies with the corresponding theoretical versions (Fig. 4(d)–(f)). In addition, the Doppler speckles emerging in the STFT-based spectrograms have a considerable similarity with those observed in sonographies of actual Doppler blood flow signals in clinic.
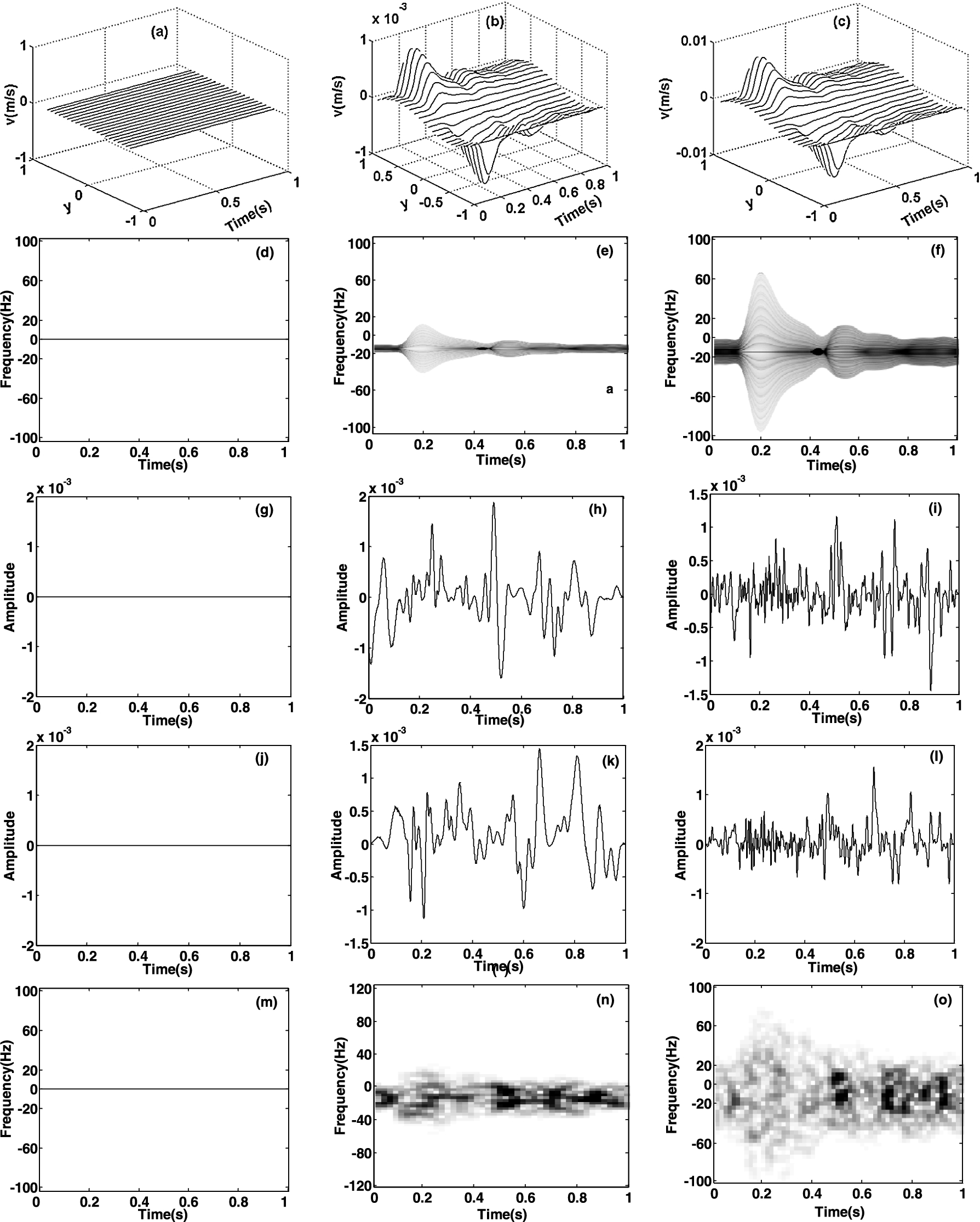
The velocity distributions (a)–(c), theoretical spectrograms (d)–(f), the simulated in-phase (g)–(i) and quadrature (j)–(l) Doppler signals, and their STFT spectrograms (m)–(o) of the radial blood flow signals in the normal vessel ((a), (d), (g), (j), (m)) and vessel with obstruction grades of 10% ((b), (e), (h), (k), (n)) and 25% ((c), (f), (i), (l), (o)) over the axial range from
Figure 5 shows the velocity profiles (Fig. 5(a)–(c)), the theoretical spectrograms (Fig. 5(d)–(f)), the in-phase (Fig. 5(g)–(i)) and quadrature (Fig. 5(j)–(l)) waveforms as well as their STFT-based spectrograms (Fig. 5(m)–(o)) of the simulated Doppler signals from radial blood flow in the healthy artery (Fig. 5(a), (d), (g), (j) and (m)) and arteries with stenosis grades of 10% (Fig. 5(b), (e), (h), (k) and (n)) and 25% (Fig. 5(c), (f), (i), (l) and (o)). Figure 5(a) indicates that the velocity of radial blood flow in normal vessel is zero everywhere at any point as the blood flows in normal vessels are laminar without radial components. Thus, the corresponding theoretical spectrogram (Fig. 5(d)), simulated I/Q Doppler signals (Fig. 5(g) and (j)) as well as the STFT-based spectrogram (Fig. 5(m)) are null. These results for radial blood flow in the healthy artery are coincided with clinical findings of laminar blood flow in healthy vessels [7].
But the axially antisymmetrical velocity profiles of radial blood flow in the arteries with obstruction grades of 10% and 25% are apparent as shown in Fig. 5(b)–(c). These can be attributed to that the blood flows in the stenosed vessel are disarranged by atherosclerotic plaques resulting in the appearance of vortices or turbulence with radial components. For a certain time, the absolute velocities in stenosis vessels (Fig. 5(b)–(c)) reach their maximums at radial locations of
Figure 6 shows the simulated I/Q Doppler ultrasound signals scattered from the near and far pulsatile vessel walls as well as its STFT-based spectrogram. Compared with the axial (Fig. 4(g)–(l)) and radial (Fig. 5(g)–(l)) Doppler blood flow signals, the wall signals characterize relatively greater amplitude, lower frequency shift, and coexistence of the positive as well as negative frequency components as they are scattered from the slowly bi-direction pulsing vessel walls, which are more powerful Doppler ultrasound reflector than the blood flow suspension scattered-particles.
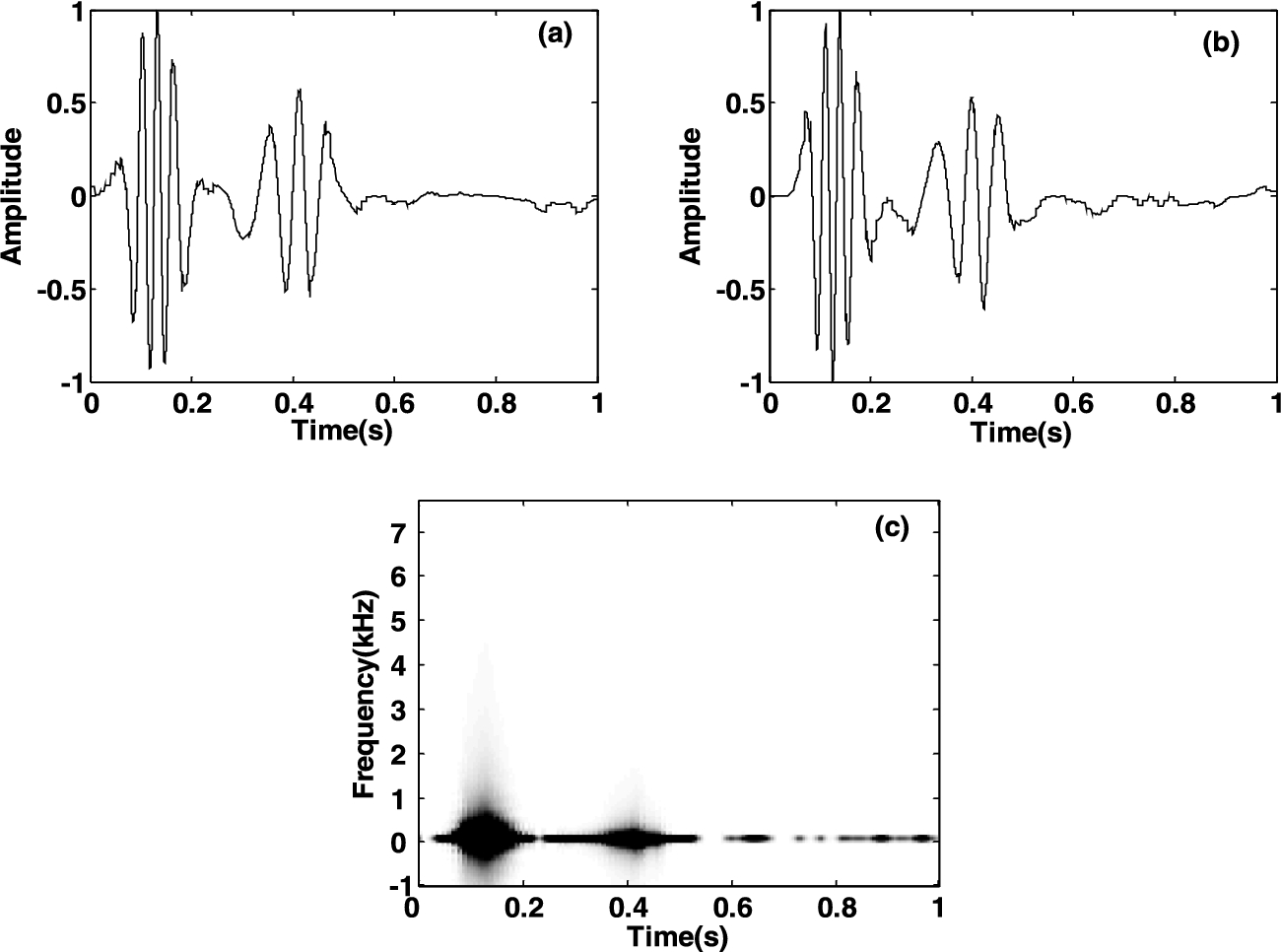
The in-phase (a), quadrature (b) simulated-Doppler signal from the vessel wall and its STFT-based spectrogram (c).
The results of the compound Doppler ultrasound signals echoed from both axial and radial blood flows as well as vessel walls of pulsatile carotid arteries with stenosis grades of 0%, 10% and 25% over the axial range from
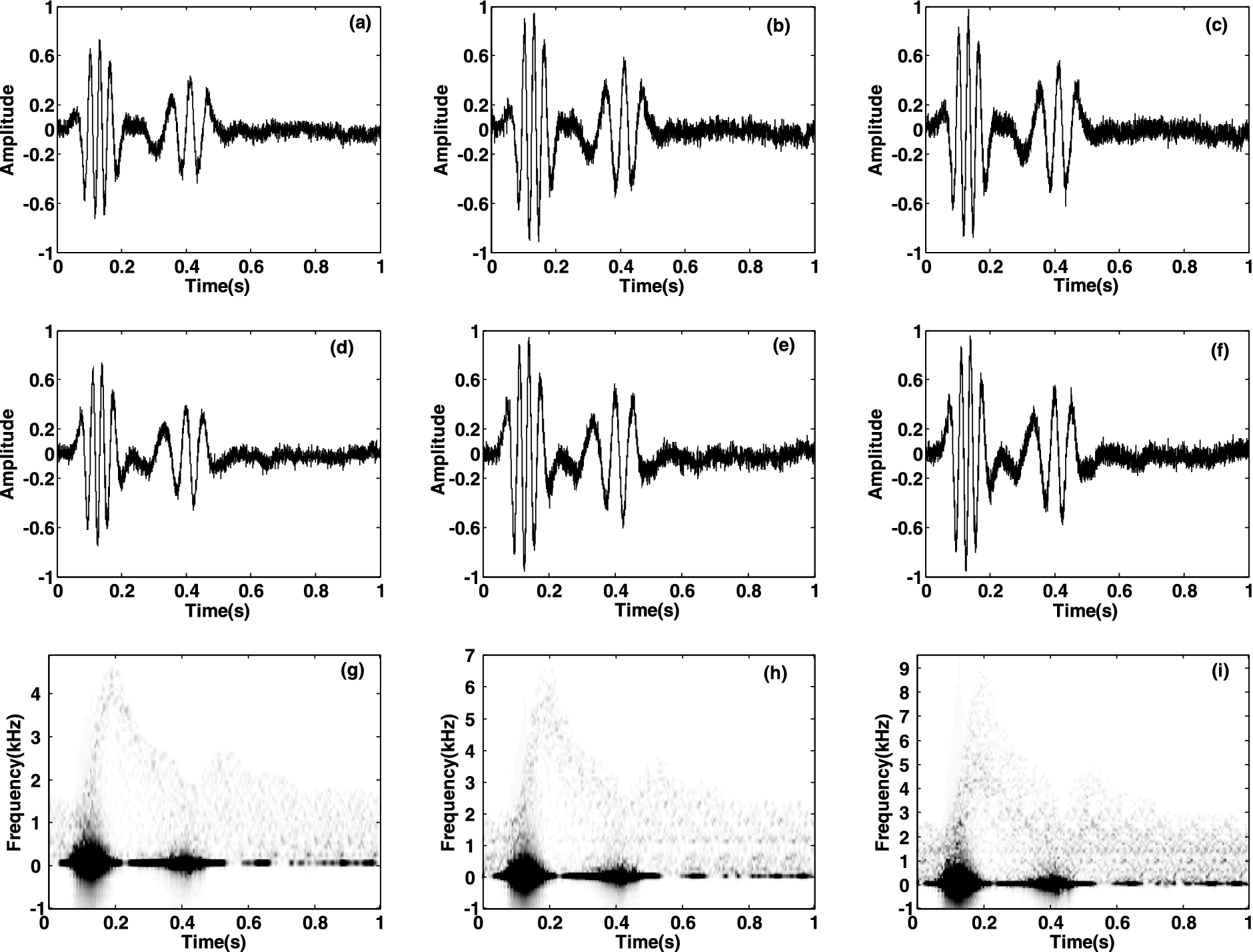
The simulated I/Q compound Doppler signals (the in-phase component (a)–(c), the quadrature component (d)–(f)), and their STFT-based spectrograms (g)–(i) involving the motions backscattered from both axial and radial blood flows as well as the vessel walls of pulsatile normal artery ((a), (d), (g)) and artery with stenosis degrees of 10% ((b), (e), (h)) and 25% ((c), (f), (i)).
For the sake of comparison study, compound Doppler ultrasound signals from a carotid artery with an approximate 10% stenosis degree are detected by using the continuous-wave Doppler blood flow detection instruments with a 8 MHz transducer by shutting down the wall filter. Figure 8 reports the in-phase (solid curves) and quadrature (dashed curves) time-domain waveforms (Fig. 8(a)) of the real I/Q compound signal, the STFT-based compound-spectrogram (Fig. 8(b)), as well as the blood flow- (Fig. 8(c)) and wall-spectrograms (Fig. 8(d)) separated by using a HPF with 400 Hz cut-off frequency. Figure 8(b) indicates that the contamination from the stenosed carotid artery walls is so considerably strong that it is hard to extract diagnostic features from the blood flow signal, especially that in the region approaching vessel walls for diagnosis of stenosis diseases. After the low-frequency components in the compound signal are filtered out, the major blood flow-spectrogram (Fig. 8(c)) presents the similar characteristics to those found from simulated axial-versions in Fig. 4(n), such as a rapid upstroke during the systolic period, a quick descent within early diastole, a slight oscillation during the late diastole and so on. At the same time, the wall-spectrogram shown in Fig. 8(d) also presents better consistency with the simulated version shown in Fig. 6(c), which demonstrates that the proposed computer simulation method can produce compound Doppler signals sharing similar characteristics with the clinical versions.
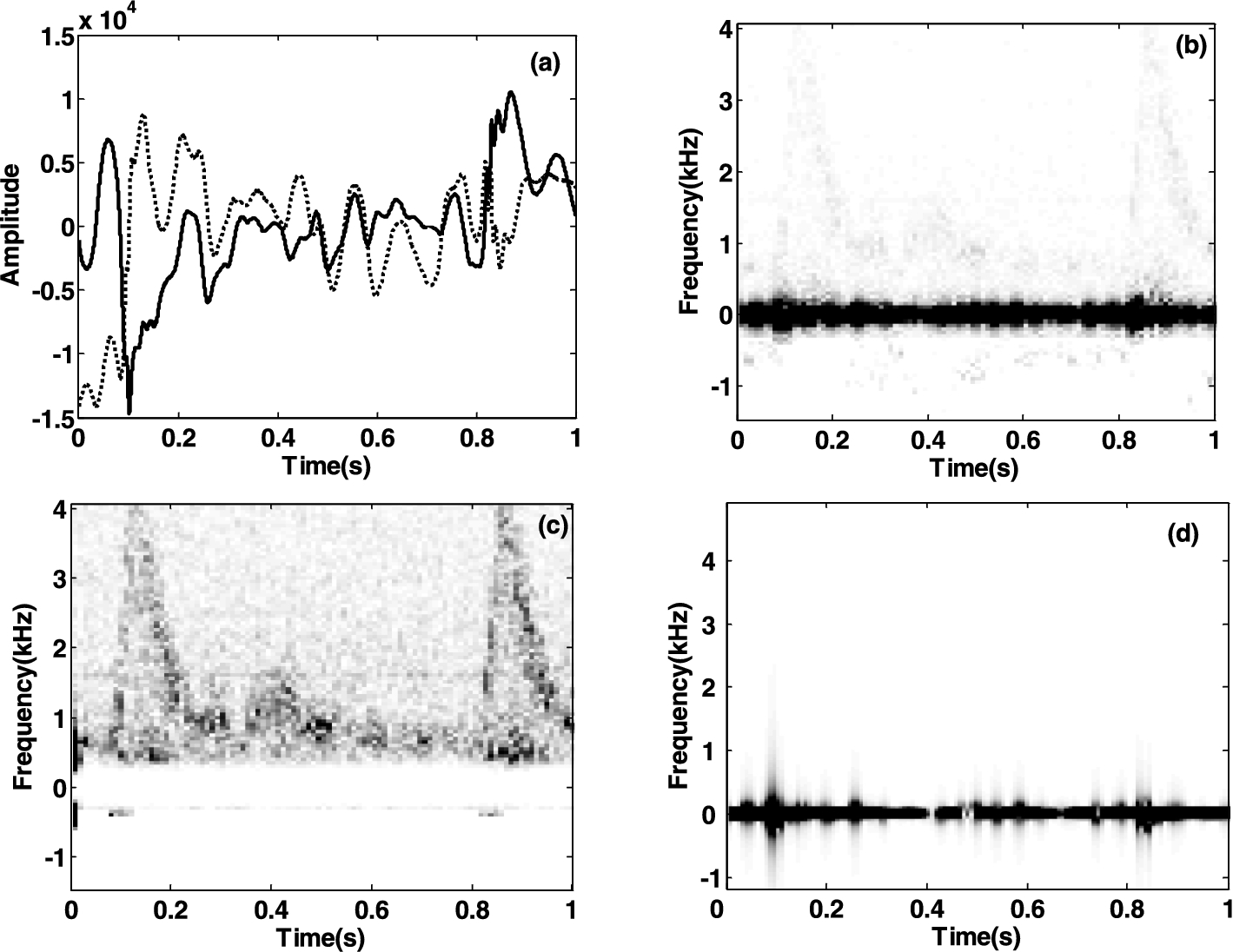
The in-phase (solid curves) and quadrature (dashed curves) time-domain waveforms (a) of a real I/Q compound signal obtained from the carotid artery with an approximate 10% stenosis degree, the STFT-based compound-spectrogram (b), the blood flow- (c) and wall-spectrograms (d) separated by using a HPF with 400 Hz cutoff frequency.
In order to obtain a data source to evaluate the performance of the clutter or wall filters for removing clutters from compound blood signals, a set of synthesis [14–17] or simulation models [18–25] have been proposed in recent years. Compared with the synthesis models, these simulation versions could produce more credible compound signals, while they were limited to pulsatile normal-vessels in which only axial blood flow exists. In an effort to advance the previously published simulation model, a method is proposed in this work to produce compound Doppler ultrasound signals including the contribution of the both axial and radial blood flows as well as pulsatile stenosed-common carotid walls. Although the geometric shape of the atherosclerotic plaque is theoretically simplified as the sinusoidal shape with a radially and axially symmetrical characteristic, it results in the alteration of the velocity profiles of axial blood flow and the emergence of the non-zero radial velocity-components at the region near the vessel walls. The simulated compound signals under these comprehensive conditions could a more objective data source for evaluating the performance of the signal separation between pulsatile blood flows and vessel walls with mild stenosed-lesions to a certain degree.
According to a set of results about the calculated velocity profiles (Figs 4 and 5(a)–(c)) based on the solution of the Navier–Stokes equations, as well as their theoretical spectrograms (Figs 4 and 5(d)–(f)) of axial (Fig. 4) and radial (Fig. 5) pulsatile blood flows, it is clear that the blood flow state tends to change from lamina to turbulence with the raise of the stenosis degrees in the stenosed vessels due to the disturbance of the atherosclerotic plaque. These results are coincided with clinical findings of vortices or turbulence in stenosed carotid arteries [7]. The STFT-based spectrograms of the simulated axial (Fig. 4(m)–(o)) and radial (Fig. 5(m)–(o)) blood flow signals, and pulsatile vessel wall signals (Fig. 6(c)), as well as the compound Doppler signals (Fig. 7(g)–(i)) suggest the similarities between the simulated and corresponding theoretical versions. Moreover, obvious random Doppler speckles appear on these STFT-based spectrograms of the simulated signals also resemble the observation in the clinical ones. These results provide valuable visual-comparisons for demonstrating the validation of the proposed simulation method. Furthermore, the validation of the simulation method reported in this study is quantitatively demonstrated by the small MSDs of NRMSESs between the theoretical and averaged STFT-based spectrograms of mixed signals for the stenosis grades of 0%, 10% and 25% over the 30 realizations. It is worth noting that the proposed method is used to simulate a continuous wave (CW) Doppler ultrasound system, which receives compound Doppler signals scattered from the pulsatile blood flow and stenosed common carotid arteries in view of the determined sample volume. However, the cosine-superposed method denoted in Eq. (11) is unsuitable for the simulation of a pulse wave (PW) system due to its small duration and sample volume leading to the non-Rayleigh amplitudes distributions of the received signals. To simulate the real PW Doppler system, the radio frequency echo signals of the moving scatterers in the entire arterial lumen with axial and radial velocity profiles determined by Eq. (6) could be firstly achieved by employing FIELD II software proposed by Jensen [30]. Then the radio frequency echo signals during a specific range locating at a transmission axial-position from the face of the transducer are selected and demodulated to produce the envelops to achieve the corresponding pulse wave Doppler signals. Another limitation to this simulation method is embodied in the assumption of the movement independence between the blood flow and arterial walls, which does not completely describe the influence on the blood flow profile by the elastic vessel wall. By considering the physiologically cyclic interactions between the blood flow and stenosed vessel walls, future work could be implemented for improving the performance of the presented simulation method to obtain more desirable results.
Conclusions
A computer simulation method is presented to produce compound Doppler ultrasound signals scattered simultaneously from both blood flow and vessel wall of pulsatile common carotid arteries with a stenosis. To simulate the I/Q blood flow signals, the axial and radial velocity profiles of pulsatile blood flow are firstly obtained by solving the NSEs in view of the center velocity of a normal vessel and geometric characteristics of the stenosed vessel, and then, the signals are simulated by superposing a series of cosine functions regulated by the spectrograms estimated from the axial and radial velocity profiles, respectively. Meanwhile, the I/Q Doppler signals echoed from pulsatile near and far walls are simulated based on their wall radial movements during a cardiac cycle. Ultimately, the confirmed quadrature signals incorporating the moving information backscattered from both axial and radial flows as well as pulsatile vessel walls are summed to generate the compound Doppler signals with regard to a definite sample volume. The simulator competency to generate the compound Doppler signals with the features resembled to those obtained in clinic has been illustrated in the experimental results. It can be concluded that the proposed computer simulation method can produce compound Doppler signals with confirmed qualitative and quantitative characteristics resembled with the clinical versions, which could be used as an theoretical data source for evaluating the performance of the signal separation between pulsatile blood flows and vessel walls with mild stenosed-lesions.
Footnotes
Acknowledgements
This work was supported by the Grant (61261007), (61361010), (61561049) from the National Natural Science Foundation of China and the Grant (2013FA008) from the Key Program of Yunnan Natural Science Foundation.
Conflict of interest
The authors have no conflict of interest to report.