
Abstract
The time needed to obtain functional regenerated bone tissue depends on the existence of a reliable vascular support. Current techniques used in clinic, for example after tooth extraction, do not allow regaining or preserving the same bone volume. Our aim is to develop a cellularized active implant of the third generation, equipped with human mesenchymal stem cells to improve the quality of implant vascularization. We seeded a commercialized collagen implant with human mesenchymal stem cells (hMSCs) and then with human umbilical vein endothelial cells (HUVECs). We analyzed the biocompatibility and the behavior of endothelial cells with this implant. We observed a biocompatibility of the active implant, and a re-organization of endothelial cells into clustered networks. This work shows the possibility to develop an implant of the third generation supporting vascularization, improving the medical care of patients.
Introduction
Recently, in the regenerative medicine field, a plethora of biomaterials based on polymeric PLA (poly lactic acid), PGA (polygly-colic acid), PCL (poly-ε-caprolactone) or natural (collagen, alginate, fibrin, chitosan) components were developed, aiming to offer an ideal environment supporting tissue regeneration after implantation. More particularly for bone tissue engineering, the implantation of collagen implants in a bone defect is a practice whose aim is hemostasis [1], commonly used after a tooth extraction for example. Collagen promotes the formation of a stable clot and helps reduce post-operative bleeding [2]. Moreover, the clinical use of collagenic biomaterials in dental surgery promotes guided bone regeneration, inter alia by means of tissue exclusion [3]. However, none of the techniques currently used in clinics to preserve or regain a good quality of bone or its initial volume (bone substitutes, allografts, xenografts, membranes of collagen for guided bone regeneration) gives satisfaction [4]. Furthermore, some xenografts have disadvantages such as high cost and low presence of autogenous bone in the rebuilt tissue volume, due to the low degradation of the material [5].
The deposit of a simple collagen implant into bone defects does not provide satisfactory results, compared to natural bone healing [6–10]. Thus, during these last decades, several kinds of active materials were developed [11–16]. These materials can be active by the addition of growth factors, or by the addition of living cells, to create a material of the third generation, which is specifically the case for regenerative medicine. Indeed, for bone regenerative medicine, collagen sponges have the advantage to be able to locally deliver active molecules (growth factors, antibiotics…) [17–20]. Studies have shown that the addition of bone morphogenetic protein (BMP) to collagen sponges significantly improved bone regeneration [21–24]. However, this technique also presents a major inconvenient: the local release of the molecules is too fast and thus, causes overdosing and adverse effects [18].
Another approach to influence the quality and speed of bone regeneration is the ability to facilitate the development of a vascular network in the bone tissue during regeneration. This network will provide the nutrients and minerals necessary for cells, conveying cellular waste [25–27], and therefore avoid the potential necrosis in the middle of bone defects of a moderate size. Nowadays, with the development of materials of the third generation, the single use of cells can be associated to the materials to increase efficiency of materials and tissue repair. The important use of human mesenchymal stem cells (hMSCs) in regenerative medicine comes from their important therapeutic effects [28,29]. These cells are not only able to directly contribute to tissue healing and repair by bone tissue differentiation, but also indirectly via paracrine secretion of angiogenic, neurogenic and anti-apoptotic factors [30]. Moreover, and particularly for the formation of vascular network, it was well demonstrated that these cells act as mural cells stabilizing blood vessels [31,32].
Our ultimate objective is to develop active materials of the third generation offering a perfect environment for vascularization. In this work, we used a porous collagen sponge, combined with hMSCs as a support for human umbilical vein endothelial cells (HUVECs) and we followed the biocompatibility and behavior in vitro of this combined scaffold.
Material and methods
Scanning electron microscopy (SEM)
Collagen sponges (Pangen®, Resorbable haemostatic collagen compress, Urgo Medical) were cut in pieces and fixed in paraformaldehyde (PFA) 4% for 10 minutes at 4°C. They were then dehydrated, and observed with a scanning electron microscope (SEM Hitachi™ 1000 or FEG Sirion XL; FEI) in conventional mode (high vacuum) with a secondary electron detector.
Cell culture
Collagen sponges (Pangen®, Resorbable haemostatic collagen compress, Urgo Medical) were cut (5 mm of diameter) and placed in multi-wall pates. They were then sterilized by 30-minutes exposure to UV light (254 nm, 30 W, distance 20 cm), and equilibrated in contact with 1 mL of serum-free Dulbecco’s modified Eagle’s medium (D-MEM) prior to cell culture. HUVECs and hMSCs were obtained from PromoCell (Heidelberg, Germany). The cells were cultured in specific growth medium supplemented with supplement mix (respectively endothelial cell growth medium, and mesenchymal stem cells growth medium, PromoCell). The cells were incubated at 37°C in a humidified atmosphere of 5% CO2. When cells reached sub-confluence, they were harvested with trypsin and subcultured.
Biocompatibility
Alamar Blue® (Thermo Fischer Scientific, Waltham, MA, USA) was used to assess cell metabolic activity over time. The Alamar Blue® test is a water-soluble, non-toxic, colorimetric redox indicator that changes color in response to cell metabolism.
Immunofluorescence
After 21 days of culture, samples were fixed with 4% PFA during 10 minutes at 4°C, rinsed with PBS, and permeabilized with 0.1% Triton X-100 for 1 h. Indirect immunostaining was performed after the fixation. To visualize specifically the surface of endothelial cells, samples were incubated overnight at 4°C using Rb Anti-CD31 (1/400, Santa Cruz Biotechnology Inc., Dallas, TX, USA). Alexa Fluor 488 anti-Rb (1/200, Life Technologies) was then applied to samples for 2 hours. After rinses with PBS, samples were incubated for 20 minutes with a solution of Alexa Fluor 546-conjugated phalloïdin (1/200, Molecular Probes, Life Technologies, Fisher Scientific, Illkirch, France). Finally, for nuclear staining, samples were incubated for 10 minutes with a solution of 200 nM DAPI (Sigma-Aldrich). Samples were then observed with a microscope equipped for epifluorescence (LEICA DM4000B).
Results
Scanning electron microscopy observations of the collagen sponge showed a porous biomaterial with a smooth surface (Fig. 1). These observations demonstrated clearly that this scaffold offer an adequate environment for cell colonization, recruitment and proliferation. To verify next the biocompatibility of the collagen sponge with human mesenchymal stem cells and with endothelial cells, we analyzed the evolution of their metabolic activity during the co-culture in vitro. This follow-up was performed using Alamar Blue® (Fig. 2). These tests showed a significant increase of cells metabolic activity from day 3 (D3) to day 14 (D14). Moreover this metabolic activity stabilized from day 14 (D14) to day 21 (D21). These results are not only consistent with the fact that this collagen implant equipped with mesenchymal stem cells is biocompatible for endothelial cells, but also for a cell reorganization. To next analyze the behavior of endothelial cells on the hMSCs coated collagen sponge, we performed a specific staining of HUVECs by indirect immunofluorescence against CD31 (Cluster of differentiation-31), a specific surface marker of endothelial cells. After 21 days of culture, we observed a reorganization of endothelial cells as “cluster” (Fig. 3).Taking together, these results clearly show the ability of the collagen sponge to support the reorganization of endothelial cells in the presence of human mesenchymal stem cells.
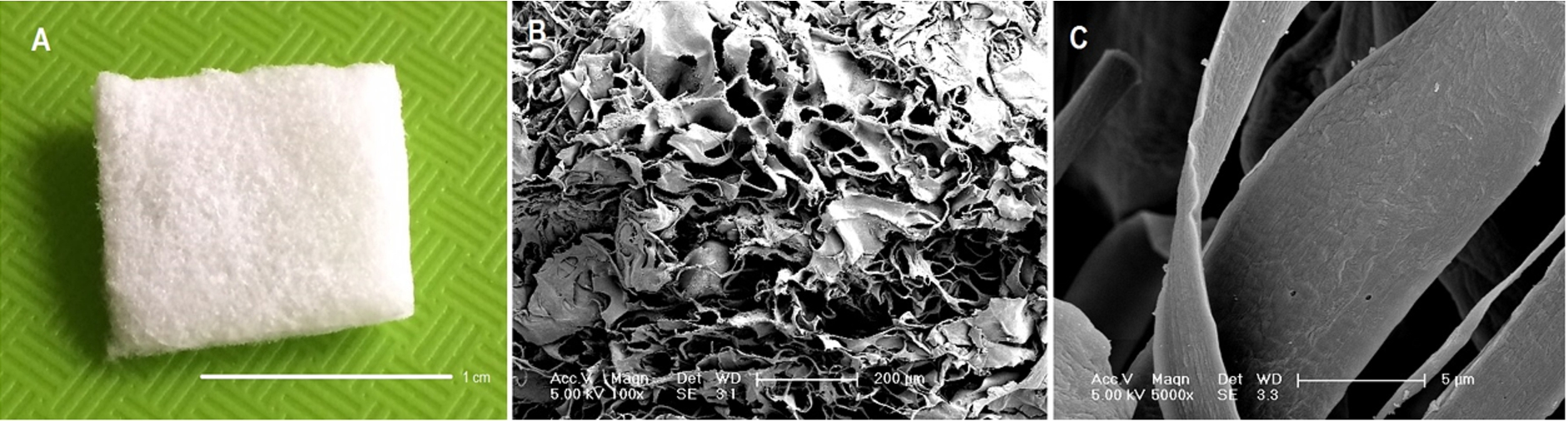
Urgo resorbable bovine collagen I implant. (A) Macroscopic view. (B), (C) Scanning electron microscopy of the collagen implant.

Biocompatibility of the collagen implant seeded with human mesenchymal stem cells and human endothelial cells. The metabolic activity of cells was analyzed (at D3, D14, D21) in vitro by an AlamarBlue® test during the culture period time (

Behavior of endothelial cells in collagen implant of the third generation. Collagen sponges (Urgo medical, Pangen®) were seeded with human mesenchymal stem cells and cultured during 7 days. After 7 days, human endothelial cells (HUVECs) were seeded on the same sample. The culture was maintained for a total of 21 days. (A) After 21 days, endothelial cells were observed by a specific immune-staining against CD31 (in green). (B) The total cells were also observed in red by phalloidin for actin and in blue by DAPI staining of the nuclei.
For efficient tissues repair, the formation of a functional vascular network plays an essential role for biomaterials host integration, providing essential nutrients necessary for the healing process. Different strategies improving vascularization and aspiring more healthy tissues construct were developed [33]. These strategies focus on the modeling of adequate scaffold morphology, the addition of growth factors, and/or the use of living cells [33]. In this work, we showed that the Urgo (Pangen®) collagen implant combined with human mesenchymal stem cell represents a biocompatible material of the third generation able to support the endothelial cells reorganization. This reorganization can be assigned to the great therapeutic potential of human mesenchymal stem cells. Indeed, these last years, it was well demonstrated and established that adult mesenchymal stem cells have an intrinsic angiogenic role [27]. Moreover, it has been shown that there is an interaction between MSCs and endothelial cells (ECs) within a co-culture [34–38], causing an increase in the secretion of growth factors [26,34,39] such as the Vascular Endothelial Growth Factor (VEGF) [27,40], and an increase in the osteogenic potential [26,41]. In our work, we chose to exploit the therapeutic effects of human mesenchymal stem cells, acting as maintainer of endothelial cells, and we were able to observe that a network reorganization of cells occurred without any additional input of VEGF.
VEGF is a protein involved in angiogenesis. VEGF is a pro-angiogenic factor inducing stem cell differentiation into endothelial cells [42–44]. Moreover, VEGF allows the recruitment of macrophages and mononuclear producing additional angiogenic factors [45]. New bone regeneration strategies are specifically focused on its use coupled with active materials [40,46]. In our previous works, we validated a strategy of nanocontainers using FDA-approved molecules, for an accelerated bone regeneration using BMP-7 or BMP-2, and adult mesenchymal stem cells [47–50]. This nano-strategy leads to a local delivery, cell-contact dependent of the growth factors, avoiding side effects after implantation [16]. More specifically for vascularization in bone tissue healing, we transferred this technology to a polymeric tridimensional implant equipped with VEGF nanoparticles able to promote endothelial cells reorganization and host blood vessels recruitment after implantation [51].
Our crucial purpose is to meet the demand from clinicians by developing a technique to enhance the quality and speed of bone vascularization and regeneration, using FDA-approved molecules. This could ensure a good quality of bone support and reduce the time before an implant surgery in dentistry for example, time during which the patient remains toothless or bearer of a potentially uncomfortable removable prosthodontics.
Conclusion
The current bone regeneration techniques used in the clinic today, for example after a tooth extraction, do not allow preserving or regaining the same volume and the same quality of bone. Natural bone healing process offers for example a usable dental implant support, but it happens that the volume of bone after healing is insufficient, and that the time before a possible implant surgery is crippling for the patient. We showed here that the combined use of a collagen sponge with human mesenchymal stem cells could represent a great support to endothelial cells reorganization. This promising approach of living implant of the third generation was biocompatible and allowed endothelial cells organization and vascularization. This new strategy could represent a real advantage to increase the speed of bone vascularization in bone tissue regeneration and filling.
Footnotes
Acknowledgement
The authors thank Valérie Demais for the characterization of the scaffolds by SEM.
Conflict of interest
The authors report no conflicts of interest in this work.