
Abstract
Bone morphogenetic protein 9 (BMP9) has previously been characterized as the strongest osteoinductive growth factor among the BMP family. The aim of the present study was to evaluate the possibility of combining rhBMP9 with an injectable biphasic calcium phosphate (I-BCP, maxresorb inject®), since I-BCP is an easy to handle biomaterial with ideal properties for bone augmentation procedures. The adsorption potential of rhBMP9 as well as the cell behavior of bone stromal ST2 cells were investigated on cell viability, adhesion, proliferation and osteogenic differentiation for I-BCP combined with/without rhBMP9 in vitro. I-BCP demonstrated excellent adsorption/retention potential of rhBMP9 with a slow and steady release over a 10 day period by ELISA. Cell attachment at 8 hours and cell proliferation at 1, 3 and 5 days was decreased on I-BCP with/without rhBMP9 when compared to control tissue-culture plastic. While I-BCP had little influence on osteoblast differentiation, its combination with rhBMP9 significantly increased ALP activity at 7 days and mRNA levels of osteoblast differentiation markers including ALP and osteocalcin at 14 days. I-BCP served as an excellent carrier for rhBMP9 clearly demonstrating its osteoinductive potential. We therefore confirm the great potential of rhBMP9 to serve as a future regenerative growth factor for bone applications.
Keywords
Introduction
Bone morphogenetic protein (BMP)-9 was first isolated from the fetal liver and has since been shown to play a positive role in stem cell proliferation [1,2]. Interestingly however, over a decade has passed since BMP9 was shown to be the strongest inducer of the BMP family in various in vitro and in vivo studies [3–7]. While these studies report on the potential for BMP9 to induce osteoblast differentiation experiments through adenovirus transfection experiments not yet approved by the FDA (gene therapy), our group very recently investigated for the first time the osteogenic behavior of recombinant human (rh)BMP9 in comparison to rhBMP2 [8,9]. It was found that rhBMP9 demonstrated markedly greater osteogenic differentiation when compared to rhBMP2 even at 10 times lower doses [8,9].
Despite positive results demonstrating the osteoinductive potential of rhBMP9 in comparison to the gold standard rhBMP2, critical to the success of osteoinductive biomaterials are their growth factor carrier system [10]. Recently, growing use of injectable bone biomaterials from various-sized syringes have become increasingly popular due to their ease of handling, fast delivery and paste like properties facilitating graft stability. In the present study, an injectable biphasic calcium phosphate (I-BCP) was selected as a potential carrier for rhBMP9 due to its well-balanced bone graft particle size and excellent osteoconductive properties [11–13].
BCP has the potential to act as a carrier for growth factors and contribute effectively to drug delivery. Several authors now report its potential to carry either rhBMP2 or rhBMP7 and induce bone formation in either animal or clinical studies [14–16]. Despite this, concerns have been raised over the true potential of growth factor adsorption to pure ceramic materials [17,18]. For these reasons, the ability to load growth factors within an injectable paste containing BCP bone particles is hypothesized to further improve the handling of growth factor delivery to bone defects. Therefore, the aim of the present study was first to determine the potential for I-BCP to load and adsorb rhBMP9 within its matrix and to investigate the release kinetics of rhBMP9 over a 10 day period. Thereafter, cell viability, attachment, proliferation and differentiation of bone stromal ST2 cells was investigated in vitro for cells seeded on I-BCP with/without rhBMP9 in comparison to standard tissue culture plastic.
Materials and methods
Regents and cell line
Recombinant human (rh) BMP-9 was purchased from R&D systems Inc (Minneapolis, MM). Injectable BCP (I-BCP, Maxresorb Inject®) was kindly provided by Botiss, Germany and is formulated from nano-hydroxyapatite water gel with biphasic calcium phosphate particles in a 60:40 HA:β-TCP ratio. For all in vitro experiments, the following 3 groups, (1) Control; tissue culture plastic, (2) I-BCP only, (3)
Scanning electron microscopy images
I-BCP samples were sputter coated using an ion coater device with 10 nm of gold and analyzed microscopically using a scanning electron microscope as previously described [19].
BMP9 adsorption quantification with ELISA
To determine the quantity of rhBMP9 adsorption to I-BCP, ELISA quantification assay was utilized. Briefly, after the coating period incubation of 100 ng/mL of rhBMP9 onto I-BCP bone biomaterials at 37 degrees Celsius in a shaking incubator, the remaining PBS solution, containing unattached protein was collected and quantified by an ELISA Duoset kit for BMP9 (DY3209,
Cell viability
ST2 cells were seeded in at a density of 12,500 cells/cm2 with I-BCP with or without rinsing in culture medium for 5 min 3 times on chamber slides (Sigma, St. Louis, MO, USA). At 1 day post cell seeding, cells were evaluated using a live-dead staining assay according to the manufacturer’s protocol (Enzo Life Sciences AG; Lausen, Switzerland) as previously described [20]. Fluorescent images were quantified with a fluorescent microscope (OLYMPUS BX51, Tokyo, Japan).
Adhesion and proliferation assay
Cells were quantified using absorbant MTS assay (Promega, Madison, WI) using an ELx808 Absorbance Reader (BIO-TEK, Winooski, VT) at 8 hours for cell adhesion and at 1, 3 and 5 days for cell proliferation as previously described [21].
Real-time PCR analysis for osteoblast differentiation markers
Total RNA was isolated using High Pure RNA Isolation Kit (Roche, Switzerland) at 3 and 14 days for osteoblast differentiation markers. Primer and probe sequences for genes encoding runt-related transcription factor 2 (Runx2), collagen 1α2 (COL1a2), alkaline phosphatase (ALP), osteocalcin (OCN) and glyceraldehyde 3-phosphate dehydrogenase (GAPDH) were fabricated with primer sequences according to Table 1. Real-time RT-PCR was performed using Roche Master mix and quantified on an Applied Biosystems 7500 Real-Time PCR Machine. A Nanodrop 2000c (Thermo, Wilmington, DE) was used to quantify total RNA levels. The
PCR primers for genes encoding Runx2, ALP, BSP, OCN and GAPDH
PCR primers for genes encoding Runx2, ALP, BSP, OCN and GAPDH
At 7 days, cells were quantified for alkaline phosphatase expression utilizing a cell imaging system. Alkaline phosphatase activity was monitored using Leukocyte alkaline phosphatase kit (procedure No. 86, Sigma) as previously described [9]. All images were captured on a Wild Heerbrugg M400 ZOOM Makroskop (WILD HEERBRUGG, Heerbrugg, Switzerland) at the same magnification and light intensity and imported into Image J software (NIH, Bethesda, MD). Thresholding was used to generate percent stained values for each field of view.
Mineralization assay
ST2 cells were seeded on
Statistical analysis
All experiments were performed in triplicate with three independent experiments for each condition. Data were analyzed for statistical significance using one-way analysis of variance with Tukey test (∗,
Results
Surface characteristics and BMP9 adsorption ability of I-BCP
In a first experiment, the surface morphology of I-BCP was investigated via SEM (Fig. 1). It was observed that I-BCP surfaces displayed a three-dimensional rough surface structure with numerous micro-pores on the surface of grafting particles. The high-magnified SEM images of I-BCP demonstrated an extremely rough surface nanotopography (Fig. 1(B)). Thereafter, ELISA was utilized to investigate the potential of I-BCP to act as a carrier for rhBMP9 by investigating the total amount of adsorbed BMP9 to I-BCP. It was first observed that nearly 90% adsorption of BMP9 was observed following a 5 minute pre-coating period (Fig. 2). The amount of BMP9 was slowly and gradually released over time from 15 minutes up until 10 days as depicted in Fig. 2. At 10 days, nearly 50% of the initial rhBMP9 was released from I-BCP bone grafts (Fig. 2).
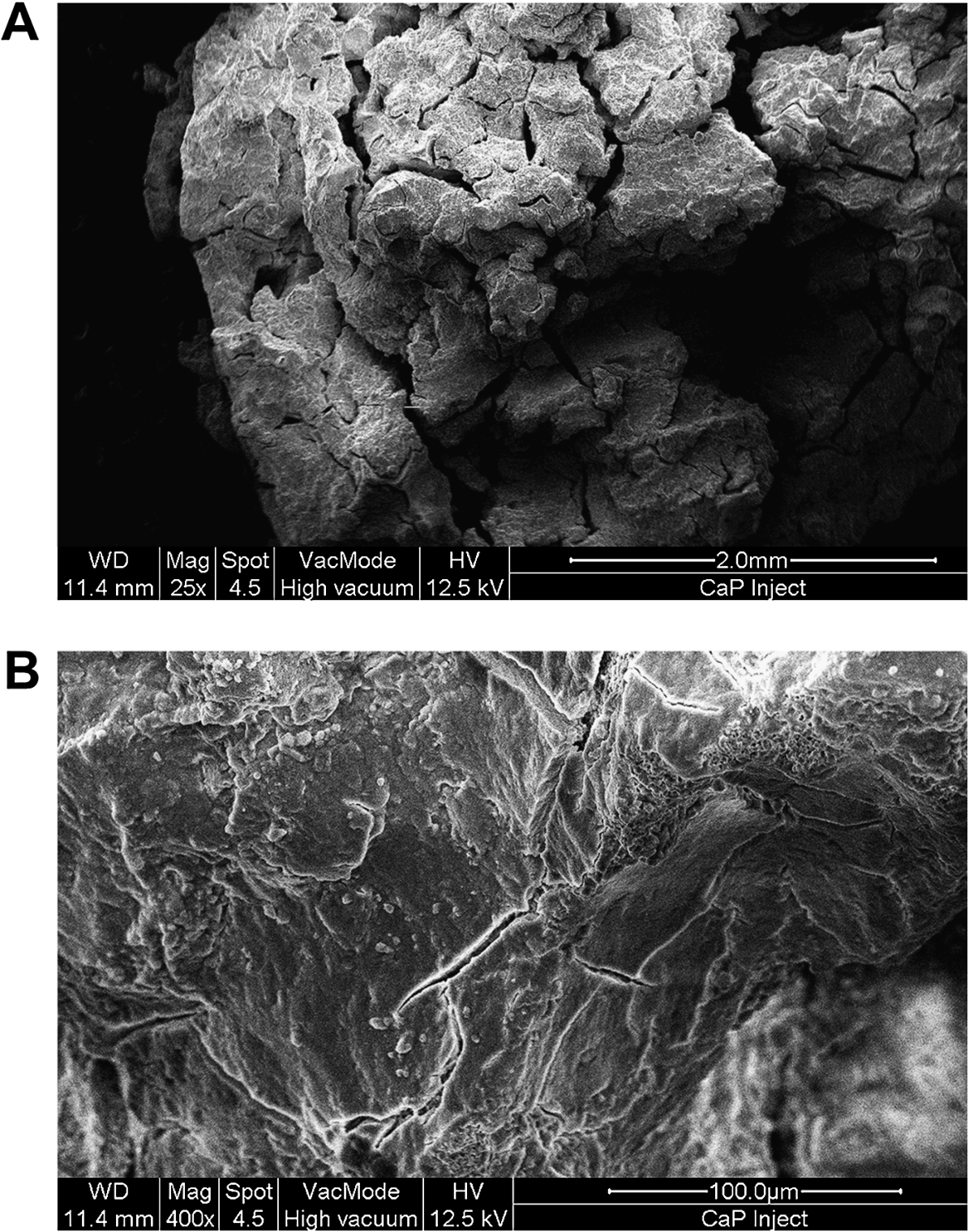
Scanning Electron Microscpy (SEM) images of I-BCP at low (A) and high (B) magnification. The I-BCP grafts display many macro- and nano-features on their surfaces characterized at high magnification imaging (

BMP9 adsorption potential of I-BCP at 15 min, 60 min, 8 hours, 24 hours, 3 days and 10 days after incorporation. The percentage of adsorption on I-BCP to the value of positive control sample (100 ng of rhBMP9) was quantified over time.

BMP9 adsorption potential of I-BCP at 15 min, 60 min, 8 hours, 24 hours, 3 days and 10 days after incorporation. The percentage of adsorption on I-BCP to the value of positive control sample (100 ng of rhBMP9) was quantified over time.Cell viability staining of ST2 cells at 24 hours post seeding when exposed to control, I-BCP only and
Thereafter, the effect of I-BCP combined with rhBMP9 was investigated on ST2 cell viability at 24 hours, cell adhesion at 8 hours and cell proliferation at 1, 3 and 5 days post seeding (Fig. 3, 4). It was first observed that I-BCP slightly decreased cell viability at 24 hours however pre-rinsing I-BCP prior to cell seeding improved significantly cell viability (Fig. 3). The additional incorporation of rhBMP9 within the scaffold did not affect cell viability in either scenario (Fig. 3(B)). Thereafter, the remaining experiments were carried out with a pre-rinse prior to cell seeding. Despite this, I-BCP alone significantly decreased cell attachment at 8 hours and cell proliferation at 1, 3 and 5 days when compared to control tissue culture plastic (Fig. 4(A), (B)). The addition of rhBMP9 did not affect the cell attachment or proliferation outcomes, except for the fact that a slight significant increase in cell number on I-BCP combined with rhBMP9 was observed at 3 days when compared to I-BCP alone (Fig. 4(B)).

Cell adhesion and proliferation assay of ST2 cells seeded on I-BCP in comparison to
The effects of I-BCP combined with rhBMP9 were then investigated on osteogenic differentiation of ST2 cells as assessed by ALP activity assay (Fig. 5) and real-time PCR for gene encoding Runx2, COL1a2, ALP and OCN (Fig. 6). While it was observed that I-BCP itself did not induce ALP activity, its combination with rhBMP significantly and markedly increased ALP staining on the surface of BCP scaffolds when compared to I-BCP alone (Fig. 6). The real-time PCR results further revealed that I-BCP alone has little effect on osteoblast differentiation (Fig. 6). While the combination of I-BCP with rhBMP9 did not affect Runx2 and COL1a2 mRNA levels, a significant 6 fold and 12 fold increase in ALP and OCN mRNA levels was observed at 14 days post cell-seeding respectively (Fig. 6(C), (D)).
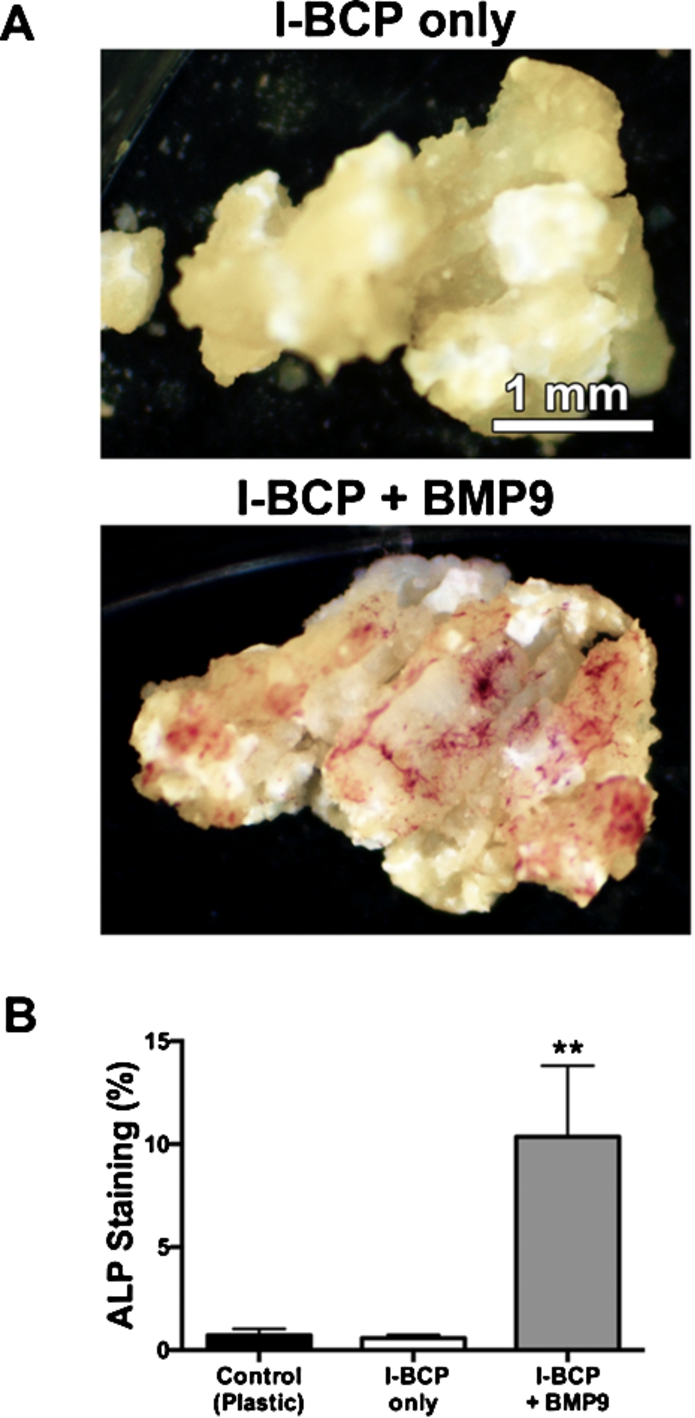
(A) Visualized images and (B) quantified data of Alkaline phosphatase (ALP) staining of ST2 cells treated on control plastic, I-BCP alone and
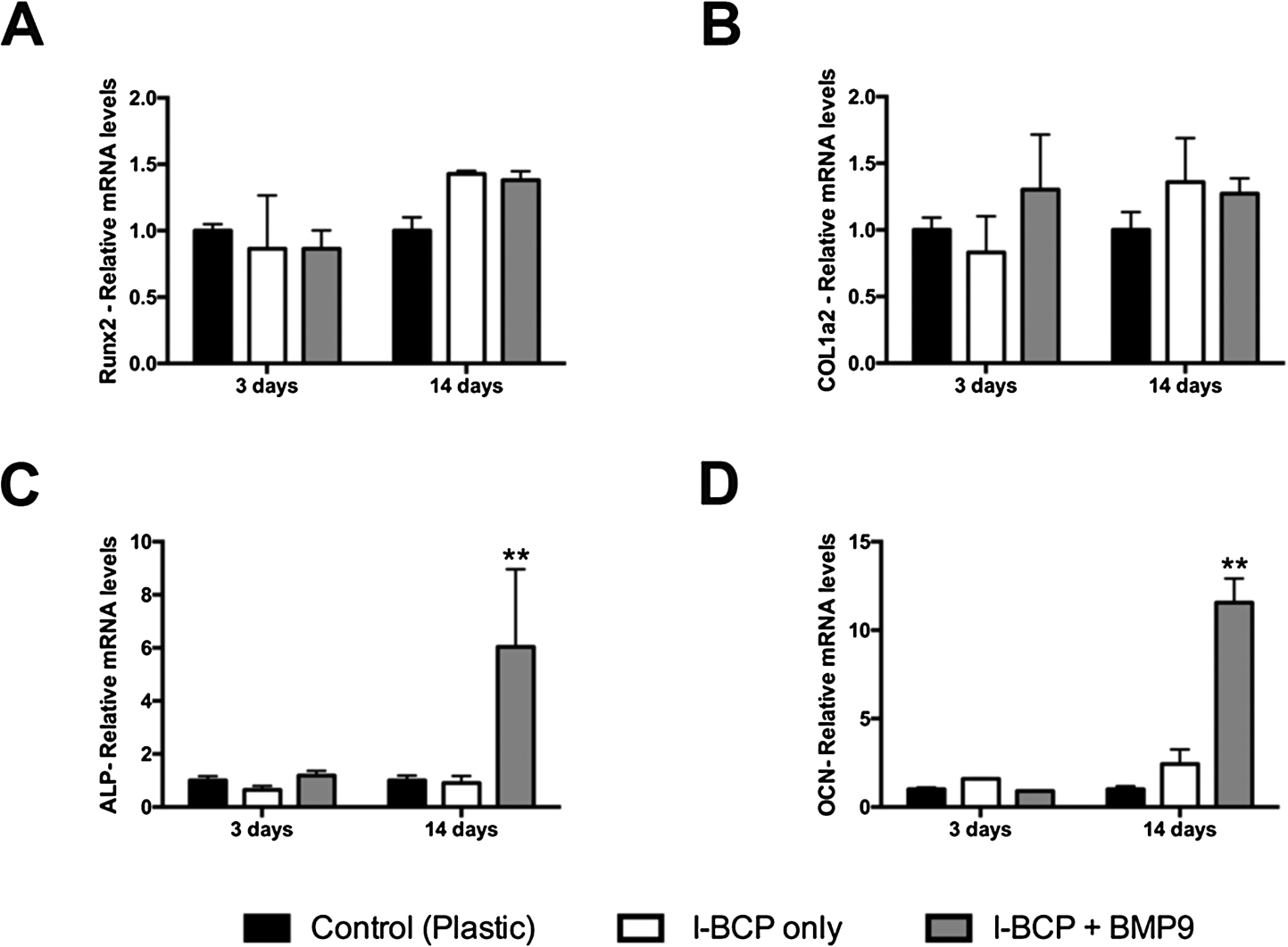
Real-time PCR of ST2 cells seeded on control plastic, I-BCP alone and
In modern medicine, combining bone grafting materials with growth factors has been utilized more commonly for complex bone augmentation procedures. This approach has been utilized to prevent the drawbacks and limitations towards harvesting large autogenous bone samples that include limited supply, additional patient morbidity, additional surgical time and additional surgical costs. BMP9 has been recognized as the most osteopromotive growth factors known to date, nevertheless very little research has investigated the possibility of combining BMP9 with a potential suitable bone biomaterial for future bone augmentation procedures. In the present study, we investigated the effect of combining for the first time the bone regenerative potential of rhBMP9 with an injectable bone graft (I-BCP) as a possible application tool for bone regeneration.
I-BCP first exhibited a surface topography suitable for growth factor retention and cell ingrowth by demonstrating a rough surface morphology with numerous micro-porosities within as visualized by SEM images (Fig. 1). BMP9 adsorption was further confirmed by ELISA, demonstrating that approximately 85% of the initial rhBMP9 concentration was loaded into I-BCP at 0 days and approximately 50% remained within the scaffold at 10 days. This confirms its suitability as a growth factor scaffold capable of slowly and gradually releasing rhBMP9 to the surrounding micro-environment over time (Fig. 2). It was previously reported by our group that BCP particles alone behaved similarly with initial adsorption of 85% but slower release of rhBMP9 with 70% remaining after a 10 day period [23]. The variation in release of rhBMP9 from I-BCP is likely caused by its paste-like formulation from the nano-hydroxyapatite water gel which clearly dissolves more rapidly than the bone grafting particles. In the present study it was found that this leads to the sustainable release of rhBMP9 with more ideal growth factor release for clinical administration. Previously, it has been reported that local burst administration of rhBMP2 may induce a number of side effects including formation of ectopic bone, sterile seroma, painful edema, inflammation and swelling [24–28]. Future research remains vital, especially granted the fact that the reaction of rhBMP9 in the human body is still unknown. Nevertheless, rhBMP9 represents a promising growth factor for future as it has more intrinsic bone regenerative potential and therefore can theoretically be administered at lower doses when compared to rhBMP2.
I-BCP unfortunately induced lower cell viability at 24 hours when compared to control tissue culture plastic and for these reasons, we decided to pre-rinse I-BCP prior to experimental seeding. Therefore, it remains to be investigated exactly what factor in these I-BCP bone grafts may be causing slight cell apoptosis (Fig. 3). I-BCP is a synthetic material composed of a mixture of 60% HA and 40% β-TCP containing nano-hydroxyapatite water gel. It is suggested that the nanoparticle components of hydroxyapatite of I-BCP might influence cell growth on ST2 cells as our laboratory has previous data demonstrating that BCP alone done not seem to cause any change in cell viability when utilized without its paste material [23]. Therefore, it remains of interest to our group to further evaluate paste materials utilized for injectable bone grafts. Currently there is very little investigation characterizing the influence of paste biomaterials on cell cytotoxicity despite their growing trends in use. Future study is paramount as it might facilitate the development of new formulations that further enhance new bone regeneration.
The osteogenic potential of I-BCP combined with rhBMP9 was further investigated (Fig. 5, 6). While I-BCP itself did not promote osteogenesis when utilized alone, its combination with rhBMP9 significantly increased ALP mRNA levels up to 6 fold, and OCN up to 12 fold respectively at 14 days post-seeding as well as ALP activities at 7 days. One of the objectives of this study was to further investigate the mineralization potential of I-BCP in vitro. Unfortunately, alizarin red staining was not adoptable to detect calcium nodules on I-BCP due to the fact that I-BCP alone was highly stained with alizarin red, which made the comparison among groups unreliable (Supp. Fig. 1). Therefore, animal research is now necessary to further characterize the regenerative potential of rhBMP9 in vivo. These preliminary in vitro experiments however highlight the strong potential of rhBMP9 combined with I-BCP to act as a growth factor/biomaterial combination capable of bone induction and the results are certainly favorable for future in vivo investigation.
Conclusion
From the experiments performed in the present study, tested injectable bone graft substitutes (I-BCP) demonstrated the ability to load rhBMP9 and favored its slow and gradual release over time. The potential of I-BCP to act as an attractive osteoinductive growth factor favoring osteoblast differentiation when combined with rhBMP9 may serve as a future regenerative tool for bone applications because of its easy handling property and strong osteopromotive potential.
Footnotes
Acknowledgements
We would like to thank Professor Tateyuki Iizuka, Department of Cranio-Maxillofacial surgery, Inselspital at the University of Bern, Switzerland, who provided the financial support for this study.
Conflict of interest
The authors have no conflict of interest to report.