
Abstract
BACKGROUND:
Obesity and leptin deficiency are associated with compromised bone regeneration.
OBJECTIVE:
This study aims to investigate the role of locally administrated low-dose BMP2+leptin on bone regeneration in leptin-deficient obese (ob/ob) mice.
METHODS:
Wildtype (WT) and ob/ob mice were divided into 3 groups (4 mice/group): BMP2 (5 μg) group, BMP2+low-dose leptin (1 μg) group, and BMP2+high-dose leptin (2.5 μg) group. WT mice were used as control mice. An equal size absorbable collagen sponge was prepared by loading the BMP2 or/and leptin and implanted subcutaneously. After 19 days, samples were collected and analyzed by micro-CT and H&E staining.
RESULTS:
No significant difference in bone regeneration among the three groups in WT mice. Quantification of newly formed bone parameters from micro-CT and H&E staining showed that low-dose BMP2 treatment formed less new bone in ob/ob mice compared to WT. BMP2+low-dose leptin treatment substantially rescued the compromised bone regeneration in ob/ob mice up to the level in WT mice. However, the BMP2 and high dose of leptin failed to rescue the compromised bone regeneration in ob/ob mice.
CONCLUSION:
Our findings suggest that a combination of the low-dose BMP2 and leptin could be a strategy to promote osteogenesis in obese populations with leptin deficiency.
Introduction
Obesity is a risk factor seriously threatening human health such as insulin resistance, type 2 diabetes, liver steatosis, which is resulted from genetic, environmental, and hormonal factors [1]. Epidemiological studies showed that obesity increases the incidence of fragility fracture [1]. Obesity is related to higher bone marrow adipose tissues causing alterations in bone architecture, finally reducing bone quality [1]. Obese bone fragility increases the risk of bone defects as a result of trauma, infection, etc. Therefore, it is essential to develop therapeutic strategies to increase bone regeneration in obese individuals with bone defects.
Leptin is a 167 amino acid cytokine-like hormone, which is encoded by the obese gene. It demonstrated that leptin is primarily produced by adipose tissue. Impairment of leptin signaling will result in several diseases such as obesity, metabolic diseases, etc [2,3]. Leptin signaling is related to normal bone growth, however, the function of leptin on osteogenesis is subject to controversy. It has been reported that leptin inhibits bone formation acting through the central nervous system [4]. While neuromedin U deficiency rescues the leptin-induced bone loss [5]. However, other reports demonstrated that leptin contributes to osteogenesis. It has been demonstrated that hypothalamic leptin usage increases bone mass [6]. Leptin receptors are expressed in osteoblasts and bone marrow stromal progenitor cells [6] and leptin administration has been shown to inhibit osteoclastogenesis and promote osteogenesis [7,8]. Intriguingly, leptin overexpression by recombinant adenoviruses improves osteogenesis in vivo [9]. Based on these findings, leptin seems to be an adipokine that can improve bone formation. However, overdosed leptin may generate certain side defects, such as leptin resistance [3]. Moreover, leptin administration solely requires multiple injections that are time-consuming and did not prove to be effective for bone repair [8].
Leptin-deficient mice (ob/ob) are widely used in the study of skeletal abnormalities. ob/ob mice show significant obese phenotypes and exhibit considerable signs of decreased mineralization with increased fragility and decreased bone thickness compared to WT mice [10]. Philbrick et al. demonstrated that exogenous leptin administration increases bone formation with minimal effect on Jak/Stat signaling and neurotransmitters in the hypothalamus [11]. Furthermore, leptin induces loss of bone marrow adipocytes and promotes bone formation in ob/ob mice [12]. Recently, Wu and colleagues demonstrated that leptin by systemic injection changes the callus vascular endothelial growth factor (VEGF) levels and promotes bone healing in ob/ob mice [13]. Together, in the case of obesity, combined treatment by leptin supplementation and another osteogenic factor may be a solution to promote bone formation.
Recombinant human bone morphogenetic protein-2 (BMP2) has several clinical applications such as spinal fusion, bone regeneration in dentistry, and maxillofacial surgery. However, a high dose of BMP2 administration is associated with several local and systemic adverse effects such as postoperative inflammation, ectopic bone formation, cervical spine swelling, and tumorigenesis [14]. Since, exogenous leptin had shown bone regenerative potential, in this study, we hypothesized that the combination of leptin and an absorbable collagenous sponge (ACS) together with low dose BMP2 is used in the clinic [15]. BMP2 might promote bone regeneration in leptin-deficient individuals. Such a combined approach may reduce the required dose of BMP2 and as such will minimize the risk of a high dose of BMP2-associated adverse effects. We added BMP2 (5 μg), BMP2 (5 μg) + 1 μg leptin, or BMP2 (5 μg) + 2.5 μg leptin in ACSs and implanted these in wildtype (WT) and ob/ob mice ectopically. Bone regeneration was evaluated on day 19 by micro-CT and histology. BMP2 (5 μg) + 1 μg leptin group showed the highest bone regenerative potential compared to other groups.
Materials and Methods
Animals
Eight-week-old C57BL/6J male ob/ob mice (n = 24) and WT (n = 24) were obtained from Viewsolid Biotechnology Co., Ltd (Beijing, China). ob/ob mice are deficient in the leptin gene. The National Institutes of Health guide for the care and use of Laboratory Animals (NIH Publications No. 8023, revised 1978) has been followed. The experiment has been approved by the medical ethics committee of the First Affiliated Hospital of Guangzhou Medical University (Approval no. 2017-087). The experimental flowcharts are shown in Fig. 1.
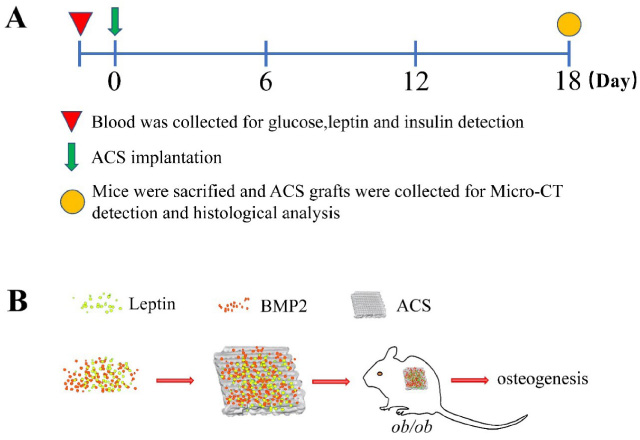
Experimental flowchart. (A) The inverted triangle indicates the time for blood collection, the green arrow indicates the time for ACS implantation, and the circle indicates the time for mice sacrifice and ACS graft collection. (B) Preparation and implantation of ACS grafts. ACS: absorbable collagen scaffold.
For each strain, male mice were treated by one of the following interventions (1) Group 1: 5 μg BMP2 + ACS (0/5), (2) group 2: 5 μg BMP2 + 1 μg leptin + ACS (5/1), (3) group 3: 5 μg BMP2 + 2.5 μg leptin + ACS (5/2.5) This study used 4 mice/group and 4 grafts/mice. Different dosages of recombinant human leptin (Sijia Biotechnology Co., Ltd, Guangzhou, China) and recombinant human bone morphogenetic protein-2 (BMP2) (Medtronic Sofamor Danek, TN, USA) were dripped into identical ACSs (Medtronic Sofamor Danek, TN, USA) samples (4 mm × 4 mm × 4 mm) one day before the surgery. BMP2 and leptin (10 μL) mixed solution was added to each sample.
The mice were anesthetized via an intraperitoneal injection of 50 mg/kg pentobarbital sodium (Sigma-Aldrich). After shaving and disinfecting, a 2 mm skin incision was made in the middle of the back of mice followed by blunt separation. Four ACS samples were implanted subcutaneously. The wound was closed with 3-0 sutures and penicillin (Sigma-Aldrich) (50 thousand unit/kg) was intraperitoneally injected. The wound was observed every day and the suture was removed on day 5. Eighteen days later, mice were anesthetized using isoflurane and sacrificed by cervical dislocation. All the samples were retrieved together with the adjacent tissues and chemically fixed in 4% paraformaldehyde overnight.
Biochemical detection
Before ACS implantation, fasting glucose was determined using a One-Touch glucometer (Abbott Diabetes Care, FreeStyle Freedom, USA) in blood taken from a tail vein nick. Blood was collected from tail vein nick or terminal bleed and stored on ice before centrifugation at 15,000 g for 10 min. Serum was subsequently flash-frozen and stored at −20 °C before analysis. Serum leptin amounts were measured with a mouse leptin ELISA kit (Crystal Chem Inc., Chicago, IL, USA). Serum insulin amounts were measured with a mouse insulin ELISA kit (Crystal Chem Inc., Chicago, IL, USA).
Micro-CT scanning
To observe the morphological changes in the collected ACS samples, samples were stored at the 4% paraformaldehyde for 24 h, following Micro-CT scanning (Bruker, Belgium). The X-ray tube was operated at 60 kV and 96 μA using a 0.5 mm Al filter with a resolution of 7.93 μm pixels. Scanning was performed by 180° rotation around the vertical axis, camera exposure time of 1300 ms, rotation step of 0.6°, frame averaging of 2, and random movement of 10. Each sample was scanned for a total of 30 min. Three-dimensional images were made using CTvox software (Bruker, Belgium). Dataviewer software (Bruker, Belgium) was further used for linear analysis. To analyze the trabecular parameters CT data were reconstructed with CT analyzer software (Bruker, Belgium).
Tissue preparation, histological procedures, and H&E staining
After Micro-CT scanning, the specimens were decalcified, dehydrated, then paraffin-embedded, and cut into tissue sections of 4 μm thickness. Then the samples were sectioned in paraffin and stained with hematoxylin and eosin (H&E) according to the methods previously reported [16]. The new bone area was quantified using Image J software. Five typical fields excluding the attached peripheral area in each slide were chosen. An average of 4 slides from each mouse was used for statistical analysis.
Statistical analysis
All data are presented as mean values together with the Standard Deviation (SD). Differences between the experimental groups were analyzed using the one-way ANOVA-test and the Bonferroni post-hoc test was implemented for comparison of mean values between strains. Significant differences were defined at p < 0.05. All statistical analyses were performed with Graphpad Prism 5 software.
Results
The characteristics for ob/ob mice
ob/ob mice were deficient in leptin and insulin resistance. As shown in Fig. 2A, the bodyweight of ob/ob mice was significantly increased compared to that of WT. Serum glucose levels in ob/ob mice were significantly increased by 39.9% compared to those in WT (Fig. 2B, p < 0.01). Leptin serum levels in ob/ob mice were reduced by 95.2% compared to those in WT (Fig. 2C, p < 0.01). We also noticed significantly increased insulin levels in ob/ob mice compared to WT (Fig. 2D).

The characteristics of the ob/ob mice. (A) The body weight, (B) serum glucose, (C) serum leptin, and (D) serum insulin concentration. Data are presented as mean ± SD, n = 6. Significant effect compared to WT, ∗∗ p < 0.01.
The bone formation was generated by adding BMP2 in both WT and ob/ob mice. In WT mice there was no significant difference in bone volume among the 3 groups treated (Fig. 3A, B). BMP2 group showed lower bone volume in ob/ob mice compared to WT (Fig. 3A, B). Bone volume in the BMP2 + 1 μg leptin group in ob/ob mice showed to be higher than that in the BMP2 group or BMP2 + 2.5 μg leptin treated ob/ob mice (Fig. 3A, B). However, in ob/ob mice BMP2 + 2.5 μg leptin treatment did not add any osteogenic effect compared to BMP2 treatment only (Fig. 3B). These results suggest that BMP2 + 1 μg leptin has higher bone regenerative potential compared to BMP2 alone or BMP2 + 2.5 μg leptin treatment.

The bone volume in ACS/BMP2/leptin constructs grafted in WT and ob/ob mice. (A) Micro-CT detection of ACS/BMP2 constructs in the presence or absence of 1 or 5 mg/mL leptin. (B) Quantitative analysis of the bone volume. Data are presented as mean ± SD, n = 4. Significant effect: compared to WT, ∗ p < 0.05, and compared to BMP2-treated ob/ob mice, ## p < 0.01.
Micro-CT showed that a robust amount of trabecular numbers in the BMP2 + 1 μg leptin treated ob/ob group compared to all other groups (Fig. 4A, B). No difference was observed in the trabecular numbers, trabecular thickness, and trabecular separation among the 3 WT groups (Fig. 4B, C, D). In BMP2 groups, trabecular numbers were decreased in ob/ob mice compared to WT (Fig. 4B). In BMP2 + 1 μg leptin groups, ob/ob mice showed higher trabecular numbers compared to WT (Fig. 4B). In ob/ob mice, BMP2 + 1 μg leptin treatment robustly increased trabecular numbers compared to the BMP2 group (Fig. 4B). Trabecular number in BMP2 + 2.5 μg leptin-treated ob/ob group was up to the level of the BMP2 + 2.5 μg leptin-treated WT group (Fig. 4B). BMP2 + 1 μg leptin-treated ob/ob group showed increased trabecular thickness compared to the BMP2 ob/ob group (Fig. 4C). BMP2 ob/ob group showed higher trabecular separation compared to BMP2 WT (Fig. 4D). Dramatic reduction of trabecular separation was observed in the BMP2 + 1 μg leptin ob/ob group compared to the BMP2 ob/ob group (Fig. 4D). In ob/ob mice, the stimulation of 1 μg leptin in combination with BMP2, the trabecular number was increased by 1.84-fold compared to the BMP2 only group, while this number was decreased by 5 μg leptin in combination with BMP2 compared to the 1 μg leptin group. The highest trabecular number was obtained by the treatment of 1 μg leptin/5 μg BMP2 in ob/ob mice (Fig. 4A, 4B). Furthermore, no significant difference in trabecular thickness was noticed between WT and ob/ob mice except for BMP2 stimulation only. No significantly different trabecular separation was found in the WT and ob/ob mice (Fig. 4D). Here, we demonstrate that leptin/BMP2 could increase the bone quality in ob/ob mice with appropriate concentration.
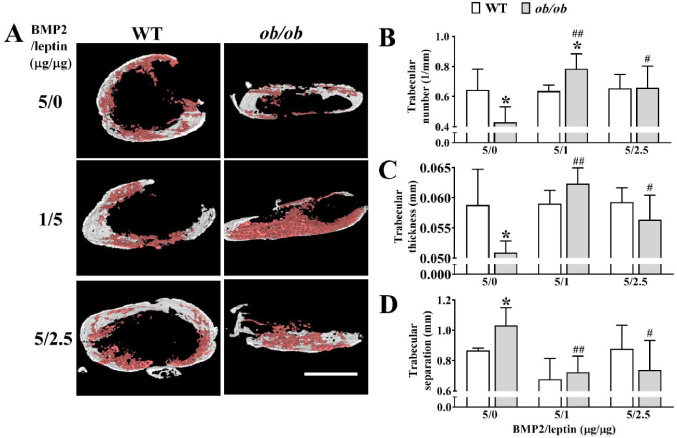
Quantification of trabecular parameters. (A) Micro-CT images of trabecular distribution. White parts show the shell of collagen carrier material; Pink parts show the trabecular formation inside of collagen carrier material. Scale bar = 1 mm. Quantitative analysis of trabecular parameters: (B) trabecular number, (C) trabecular thickness, and (D) trabecular separation. Data are presented as mean ± SD, n = 4. Significant effect: compared to WT, ∗ p < 0.05, and compared to BMP2-treated ob/ob mice, # p < 0.05, ## p < 0.01.
To further characterize newly formed bone, we detected the overall bone structure by H&E staining (Fig. 5). An almost similar extent of newly formed bone was observed in all 3 groups of WT mice. BMP2 + 1 μg leptin-treated ob/ob mice showed the homogenously formed bone throughout the ACS graft. The newly formed bone area was most prominent in the BMP2 + 1 μg leptin-treated ob/ob mice compared to all the other groups (Fig. 5B). And the bone marrow-like structures were observed between the newly formed bone. Bone marrow regions have been reported to be relevant for bone regeneration [17]. In BMP2 + 2.5 μg leptin-treated ob/ob mice, the number of newly formed bone regions was higher compared to BMP2 treated ob/ob mice but lower compared to BMP2 + 1 μg leptin-treated ob/ob mice. This result is in accordance with the findings from micro-CT results, indicating a synergistic effect of BMP2 and 1 μg leptin on bone regeneration in ob/ob mice. A bone lacuna is a small cavity within the bone matrix, containing an osteocyte. Distinct bone lacunae were visualized in BMP2 and 1 μg leptin-treated group. Similarly, osteoclast-like cells were observed on the surface and cavities of the newly formed bone in the BMP2 and 1 μg leptin treated ob/ob group. All these results indicate the active bone regeneration and bone remodeling in BMP2 and 1 μg leptin treated ob/ob group.

H&E staining of tissue sections of ACS/BMP2/leptin constructs. (A) The whole presentation of ACS/BMP2 constructs in the presence of 0, 1, or 2.5 μg leptin. (B) High-resolution images showing bone regeneration and active bone remodeling, demonstrated the new bone tissue (b), remaining collagen carrier material (c), bone marrow-like elements (m), bone lacuna (green arrow), and osteoclast-like cells in cavities (blue arrow) and surface (black arrow).
Obese individuals show a higher risk for bone fractures [1]. Therefore, it is essential to explore efficient strategies for bone repair in the obese population. Some obese individuals have been associated with the reduction of leptin levels resulting from frameshift mutation or points mutation [18–20]. Leptin secreted from adipose tissue is involved in osteogenic differentiation. Wong et al. reported that reduced leptin in ob/ob mice inhibits cortical bone formation by increasing neuropeptide Y expression [21]. Also, leptin regulates chondrogenic differentiation in tibial and vertebral epiphyseal plates through STAT and ERK signaling [22]. BMP2 has been successfully applied in clinics for bone regeneration in the field of dentistry and maxillofacial surgery [23]. Here, we investigated whether synergic administration of BMP2 and leptin could be used for bone repair in obese individuals.
Previously, we have shown that 5, 10, or 20 μg BMP2 adsorbed in ASCs does not affect bone regeneration [23]. Due to negative side effects of higher BMP2 doses, such as tumorigenesis, adipogenesis, etc, minimizing the BMP2 concentration is crucial for clinical application [24]. Here, we used 5 μg BMP2 as the experimental concentration. BMP2 promotes bone formation in WT mice but the effect was minimum in ob/ob mice (Fig. 3). The addition of 1 or 2.5 μg of leptin did not significantly promote bone formation in the WT mice (Fig. 3A). Leptin has been reported to regulate osteogenesis in dose-dependent manner [25]. Furthermore, BMP2 alone failed to promote bone regeneration in ob/ob mice. BMP2 in presence of 1 μg but not in 5 μg leptin robustly promoted osteogenesis in ob/ob mice indicating a synergistic effect of BMP2 and low dose leptin on osteogenesis during leptin deficiency. It demonstrated that betulinic acid could augment the BMP2 induced bone formation via Smad1/5/8 and p38 pathways [26]. In addition, mollugin, a natural product isolated from the root of Rubia, potentiates the osteogenic action of BMP2 in C2C12 cells via the p38-Smad pathway [27]. Previously, it has been shown that leptin stimulates the autocrine effects of BMP2 in human chondrocytes initiating the catabolic response through the JAK2-STAT3 pathway [28]. In the current study, we found the synergistic effect of leptin and BMP2 on osteogenesis in ob/ob mice. And the synergistic application may reduce the BMP2 doses, finally balancing the side effect and osteogenic function of BMP2.
In ob/ob mice, most new bone was formed with the addition of 1 μg leptin and 5 μg BMP2 (Fig. 5). The dose of BMP2 used in this study was relatively low (5 μg) compared to the BMP2 dose used in previous studies (20 μg, or even higher amount) [29,30]. A low dose of BMP2 formed a relatively low amount of new bone in ob/ob mice compared to in WT mice. However, the combination of 1 μg leptin and 5 μg BMP2 successfully rescued the compromised bone regeneration in ob/ob mice and the amount of newly formed bone was even more than in WT mice. Bone lacunae are morphological small spaces containing osteocytes that are important for bone mechanosensing and remodeling. A higher number of bone lacuna and bone marrow-like structures were observed in the combined BMP2 + 1 μg leptin-treated ob/ob mice. Similarly, central canal-like structures for blood vessel penetration were observed. Bone resorbing osteoclast-like giant cells and bone lining osteoblast-like cells were also visible on the surface of the newly formed bone, suggesting the active bone remodeling in BMP2 + 1 μg leptin treated ob/ob mice. Overall, our results indicate that the BMP2 in combination with a low dose of leptin has the potential to augment bone regeneration in ob/ob mice. This approach could apply to bone tissue engineering applications in leptin-deficient individuals and reduce the dose of BMP2 application avoiding the risk of high dose BMP2. The limitation of this study is that we did not test the bone regenerative potential in situ. However, the robust bone regeneration in the ectopic model warrants even higher bone regenerative potential in situ bone environments. The mechanism of BMP2 + leptin-induced bone regeneration should be further investigated.
Conclusion
This study elucidated the bone regenerative potential of low-dose BMP2 and leptin in leptin-deficient mice. Our results provide the foundation of a novel approach for bone regeneration in leptin-deficient individuals.
Footnotes
Acknowledgements
This study was supported by National Natural Science Foundation of China (82150410451), Guangdong Provincial Natural Science Foundation (2018A030310182), High-level University Construction Funding of Guangzhou Medical University (02-412-B205002-1003017 and 06-410-2106035) and Science and Technology Program of Guangdong Province (2014A030304069, 2015A030303016).
Conflict of interest
None to report.