
Abstract
Background:
There are few reports of Low-intensity pulsed ultrasound (LIPUS) treatment for fresh forearm fractures in children.
Objectives:
LIPUS stimulation was applied after surgery of forearm fractures in children and the efficacy and safety of combination therapy of LIPUS treatment were evaluated.
Patients and methods:
Children with both radius and ulna fracture, twenty-five diaphysis (mid-R&U) and nineteen metaphysis (dist-R&U) fractures, were treated with intramedullary nailing followed by cast and splint mobilization. Thirteen patients in the mid-R&U fracture group and eight patients in the dist-R&U fracture group were combined with LIPUS stimulation postoperatively.
Results:
Periosteal callus appeared significantly earlier after surgery in the LIPUS-treated groups than in the groups without LIPUS treatment. The duration of external fixation was significantly shorter in the dist-R&U fracture group treated with LIPUS stimulation compared with that in the mid-R&U fracture group without LIPUS treatment. Furthermore, the time span needed for bone union in the groups with LIPUS stimulation was significantly shorter than in the groups without LIPUS stimulation.
Conclusions:
It is suggested that LIPUS stimulation can lead to a reduction of treatment periods of unstable forearm fractures safely after operation even in children.
Keywords
Introduction
Closed reduction and cast immobilization is usually chosen in the treatment of forearm fractures in children, however, re-displacement in the cast occurs frequently in up to 25% of forearm fractures [1,2]. Therefore, open reduction and fixation using intramedullary nails is often indicated for treating unstable diaphyseal forearm fractures in children [3]. This operative procedure is technically easy, and allows for micromotion at the fracture site, that is beneficial for fracture healing [4]. However, more than 5% of re-displacement is reported without cast immobilization [5] because intramedullary nailing is biomechanically unstable with forearm pronation and supination [6]. Moreover, the mid-diaphysis of ulna is termed as a “watershed area” in the intraosseous blood circulation, which is supplied from the anterior and posterior interosseous arteries [7,8]. Hence, pseudarthrosis or delayed union caused by circulatory disturbance in the region is concerned when fractured. In such a case, low-intensity pulsed ultrasound (LIPUS) stimulation is expected as an ancillary technology to facilitate fracture healing including delayed union [9], nonunion [10,11] and a fresh fracture [12,13]. However, there are few reports of LIPUS treatment for fresh forearm fractures including both radius and ulna diaphysis as well as metaphysis in children. In this study, LIPUS stimulation was applied after intramedullary nailing for both radius and ulna diaphysis or metaphysis fracture in children, and the efficacy and safety of combination therapy of LIPUS treatment on such unstable fracture healing were evaluated.
Patients and methods
Forty-four children with both radius and ulna fracture, twenty-five diaphysis (37 males and 7 females, 4–15 years, mean age
In cases operated between January 2011 and December 2012, LIPUS stimulation was not applied after surgery. Subsequently, between January 2013 and March 2016, operated patients were treated with a LIPUS system (SAFHS 4000J, Teijin, Tokyo, Japan) post-operatively. LIPUS treatment was continued until bone union once per day for 20 minutes for each fracture using the following parameter configuration: average intensity
Anterior-posterior, lateral and oblique radiographs were taken immediately after operation, and every week postoperatively until bone union was verified. The fracture healing process was assessed radiographically by an attending doctor for hand surgery and a radiologist for a radiolucent fracture line with or without marginal sclerosis, sharp or blurry fracture margins, callus appearance and its bridging over involved cortices. Periosteal callus was observed even in the cast and became clear as it had matured, however, newly formed callus could not always be confirmed definitely in the fracture site of both radius and ulna coinstantaneously in the cast. Therefore, the time of callus appearance was defined as the first appearance of callus in the fracture site of either radius or ulna. By evaluating a loss of fracture margins or development of a bone-to-bone callus bridge, bone union of each bone was defined when bridging of more than 3/4 of the involved cortices was completed, in the anterior, posterior, medial and lateral regions [14]. The time of complete bone union was defined when both radius and ulna fractures were united. Functional recovery, including wrist extension and flexion as well as forearm pronation and supination, was measured until its improvement plateaued, which was evaluated as a percentage of range of motion (ROM) in the fracture site compared with that in the uninjured site.
The baseline data of the patient including age and waiting period until surgery, timing of pin removal, duration of cast immobilization, time needed for callus appearance and bone union, and observation period after surgery, as well as a percentage of ROM in the four groups, both radius and ulna diaphysis or metaphysis fracture group treated with and without LIPUS stimulation, were compared using the Bonferroni/Dunn test. The number of patients classified according to gender and injured site were compared using the chi-square test. The differences were considered statistically significant when
Results
There were no significant differences between the baseline data including age, number of patients classified according to gender, injured site and waiting period until surgery in each group (Table 1). There were no patients lost to follow up in the groups. Complete bone union was obtained in all patients and no major complications, including pseudarthrosis, delayed union, infection and skin necrosis, as well as peripheral nerve, vascular and tendon injuries, were observed.
The baseline data including age, number of patients classified according to gender, injured site and waiting period of the groups
The baseline data including age, number of patients classified according to gender, injured site and waiting period of the groups
mid-R&U, LIPUS (−): both radius and ulna diaphysis fracture group without LIPUS treatment.
dist-R&U, LIPUS (−): both radius and ulna metaphysis fracture group without LIPUS treatment.
mid-R&U, LIPUS (+): both radius and ulna diaphysis fracture group treated with LIPUS stimulation.
dist-R&U, LIPUS (+): both radius and ulna metaphysis fracture group treated with LIPUS stimulation.
Rt: right, Lt: left.
Average ± SD.
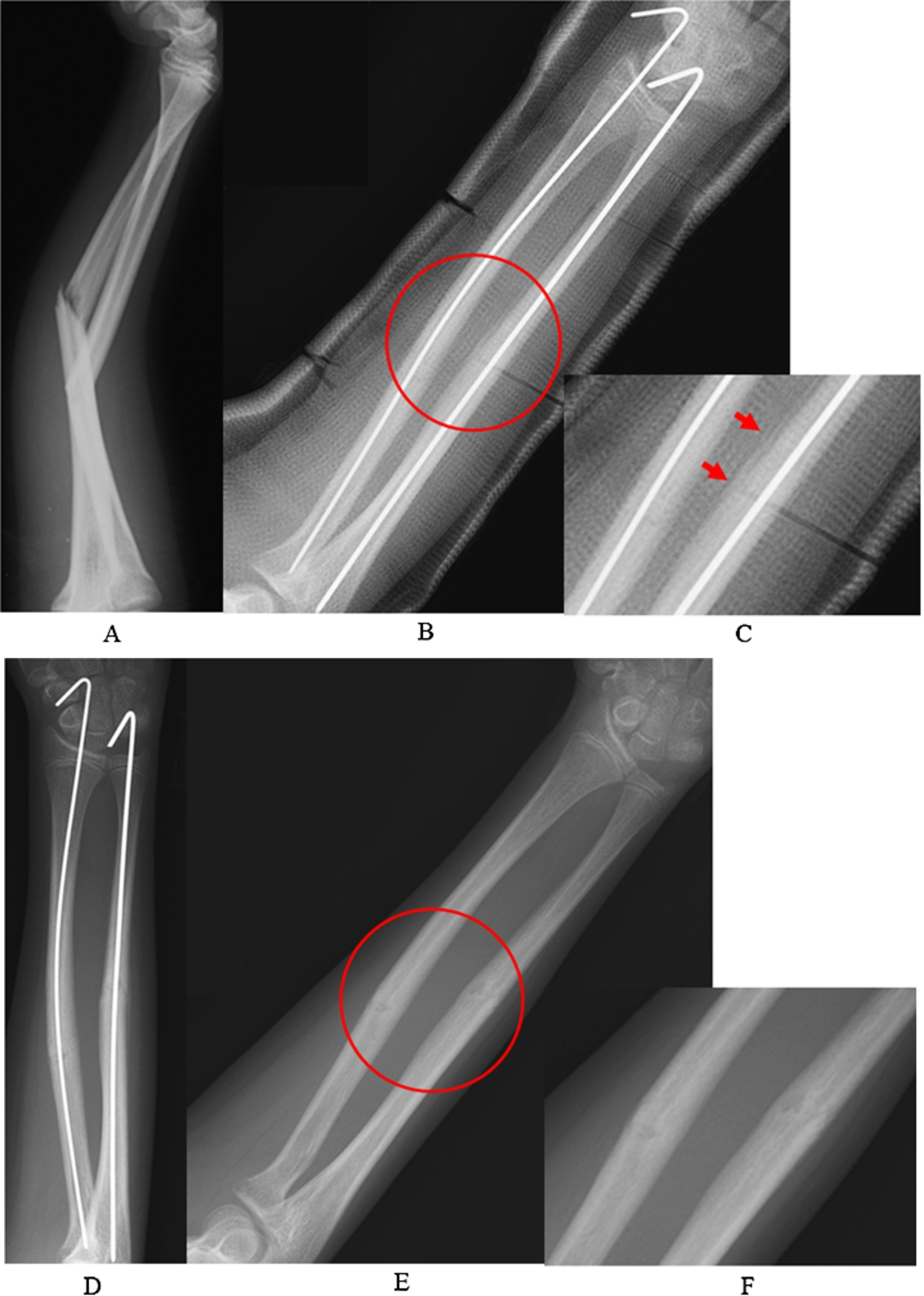
Radiographs from a patient in the radius and ulna diaphysis fracture group with LIPUS stimulation group. (A) A case of a 10-year-old male who suffered both radius and ulna diaphysis fractures. (B) A radiograph taken at 2 weeks after operation. (C) Enlargement of the Fig. 1(B). Periosteal calluses bridging over the ulna fracture site is observed in the cast (arrows). (D) Bridging callus over the fractured cortices has matured as early as 4 weeks after operation and pins are removed. (E) Bridging bone over the fractured cortices has matured at 6 weeks without angulation. (F) Enlargement of Fig. 1(E). This case is considered as complete bone union.
Periosteal callus appeared as early as 1–2 weeks after surgery in the LIPUS stimulation groups, which was confirmed even in the cast, and it had matured early to form bone bridging over the fractured cortices (Fig. 1). Conversely, callus formation and maturation delayed in the groups without LIPUS treatment, resulting in retardation of bone union (Fig. 2). Periosteal callus formation was observed significantly earlier after surgery in the LIPUS stimulation groups than in the groups without LIPUS treatment (Table 2). There was a tendency that the timing of K-wire removal and duration of cast and splint immobilization in the groups with LIPUS stimulation groups were shorter than those in the groups without LIPUS treatment. Moreover, the duration of external fixation was significantly shorter in the radius and ulna metaphysis fracture group treated with LIPUS stimulation compared with that in the radius and ulna diaphysis fracture group without LIPUS treatment. Furthermore, the time span needed for bone union in the groups with LIPUS stimulation was significantly shorter than that in the groups without LIPUS stimulation, and that in the radius and ulna metaphysis fracture group without LIPUS treatment was significantly shorter than in the radius and ulna diaphysis fracture group without LIPUS treatment, in which group 3 cases of malunion occurred. This malunion included 2 cases of angulation of ulna toward radius and one case of converse pattern within the range impingement did not occur.
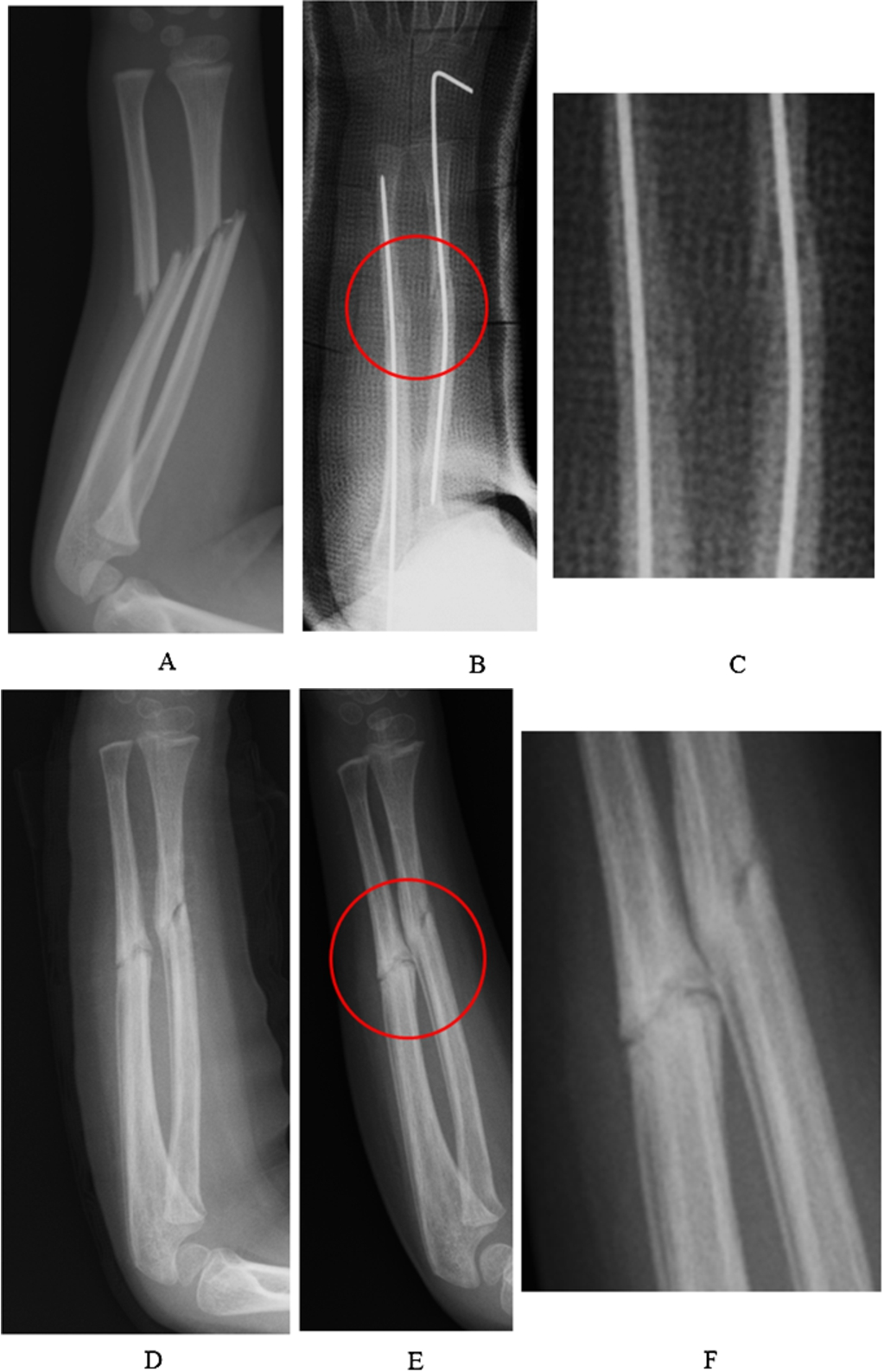
Radiographs from a patient in the radius and ulna diaphysis fracture group without LIPUS stimulation. (A) A case of a 4-year-old male who suffered both radius and ulna fractures at the diaphysis. (B) A radiograph taken at 4 weeks after operation. (C) Enlargement of Fig. 2(B). Periosteal callus formation in the fracture site is not clear yet. (D) Bridging bones over the fractured cortices are immature at 8 weeks after operation. (E) Maturation of bridging bone over the fracture site especially in ulna has delayed even after 12 weeks. (F) Enlargement of Fig. 2(E). Fracture line is confirmed clearly through the diaphysis of ulna.
When the percentages of ROM in the fracture site compared with that in the uninjured site are compared, there was a tendency that recovery of wrist extension and flexion was slightly limited in the radius and ulna metaphysis fracture groups, and that recovery of forearm pronation and supination was slightly limited in the radius and ulna diaphysis fracture groups regardless of LIPUS treatment. However, useful functional recovery was obtained in each fracture group, and there were no significant differences between the patients with and without LIPUS stimulation (Table 3).
The timing of pin removal, duration of external fixation including cast and splint immobilization, time needed for callus appearance and bone union, number of malunion and observation period after surgery

The percentages of ROM in the fracture site compared with that in the uninjured site, including wrist Ext and Flex as well as forearm Pro and Sup, when ROM improvement plateaued
mid-R&U, LIPUS (−): both radius and ulna diaphysis fracture group without LIPUS treatment.
dist-R&U, LIPUS (−): both radius and ulna metaphysis fracture group without LIPUS treatment.
mid-R&U, LIPUS (+): both radius and ulna diaphysis fracture group treated with LIPUS stimulation.
dist-R&U, LIPUS (+): both radius and ulna metaphysis fracture group treated with LIPUS stimulation.
Flex: flexion, Ext: extension, Pro: pronation, Sup: supination.
Average ± SD.
Previous studies showed that LIPUS treatment can facilitate bone healing during the early stage, callus formation and new bone formation, through the promoted cell proliferation and enhanced activities of osteogenic cells [15–20], as well as enhancement of angiogenesis [21–24]. In this study, callus formation was observed to occur faster in the groups with LIPUS treatment than in the groups without LIPUS treatment. Furthermore, the time needed for bone union in the LIPUS-treated group was significantly shorter than that in the group without LIPUS therapy. These results suggest that LIPUS stimulation can successfully facilitate the fracture healing process even in the children’s forearm fracture in the period of growth through a mechanism that involves manipulation of the expression and function of variety cells.
Prospective randomized controlled studies showed accelerated distal radius fracture healing in adults using LIPUS treatment [25,26], where more rapid bone union could decrease the chance of angulation. However, there is little evidence that it can decrease healing time and time spans needed for callus appearance and bone union in operatively treated fractures, especially in children. Because fracture healing of the radius and ulna metaphysis is easily attainable with intramedullary nailing and cast immobilization in children, combined application of LIPUS treatment may not be needed post-operatively. However, poor intraosseous blood circulation in the mid-diaphysis of ulna, termed the “watershed-zone” in a previous study [8], can be easily disturbed. Furthermore, treatment period of the unstable fracture including both radius and ulna can take a long time and re-displacement occur in the cast. Therefore, intramedullary nailing with a K-wire followed by application of LIPUS therapy in the fracture of both radius and ulna especially at the diaphysis is expected to be beneficial for facilitating callus formation and maturation to form new bone, resulting in prevention of malunion.
In this study, the early callus appearance with LIPUS stimulation resulted in early bone union compared with the group without LIPUS stimulation. Furthermore, the time until K-wire removal and the period of cast and splint immobilization were tended to be shorter, and the number of malunion was slightly smaller in the LIPUS-treated group than in the non-LIPUS-therapy group. These results support the hypothesis that LIPUS stimulation can lead to a reduction of treatment periods of unstable forearm fractures postoperatively even in children. Meanwhile, the duration of external fixation in the radius and ulna metaphysis fracture group treated with LIPUS stimulation was shorter than in the radius and ulna diaphysis fracture group without LIPUS treatment. Moreover, the time span needed for bone union in the groups without LIPUS treatment was shorter in the metaphysis fracture group than in the diaphysis fracture group. These results suggest that the healing time after operation in both radius and ulna fracture at diaphysis takes longer than at metaphysis, however, the duration of treatment can be shortened by the combined use of LIPUS therapy. Although slight limitation of ROM remained, useful functional recovery was definitely obtained in each fracture group, with and without LIPUS therapy. These findings can be explained by the fact that the large tolerability of joint contracture in children due to their prominent joint plasticity.
Major limitations of the present study are described as below; it is a retrospective single-institution study and not randomized, the timing of K-wire removal or duration of cast immobilization decision may be biased by each operator and the presence of growth disturbance is not evaluated. Long-term multicenter clinical trial should be organized to solve these issues and confirm such a hypothesis that intramedullary nailing combined with LIPUS stimulation may be recommended as a reliable and safe method for the treatment of unstable forearm fractures in children.
Conclusions
LIPUS stimulation was applied after intramedullary nailing for both radius and ulna diaphysis or metaphysis fracture in children, and the efficacy and safety of combination therapy of LIPUS treatment on such unstable fracture healing were evaluated. It is suggested that LIPUS stimulation can lead to a reduction of treatment periods of unstable forearm fractures safely after operation even in children.
Conflict of interest
The authors have no conflict of interest to report.