
Abstract
BACKGROUND:
There are no reports to prove the repeatability of gastric transit time (GTT) and small bowel transit time (SBTT) in capsule endoscopy (CE).
OBJECTIVE:
To clarify the repeatability and factors that affect GTT/SBTT in CE.
METHODS:
We analyzed the data of 150 healthy subjects from our previous randomized controlled trial that compared small intestinal injuries between two 14-day treatment groups: 1) celecoxib and 2) loxoprofen + lansoprazole. Correlation of GTT/SBTT with pre- and post-treatment CE was analyzed. In addition, the associations of pre-treatment CE SBTT with physical factors, post-treatment CE SBTT and the presence of small intestinal mucosal injuries were analyzed.
RESULTS:
Analyses of 148 subjects pre-treatment CE and 146 subjects post-treatment CE were performed. There were no significant differences between mean GTT and SBTT before and after treatment. Both GTT (𝜌 = 0.22, p < 0.01) and SBTT (𝜌 = 0.47, p < 0.0001) showed positive correlations between pre- and post-treatment CE. In pre-treatment CE, physical factors and the presence of small intestinal mucosal injury had no associations with SBTT.
CONCLUSIONS:
Moderate correlation in SBTT and slight correlation in GTT were shown on repeated CE. The factors affecting SBTT were not clarified in this analysis.
Introduction
Capsule endoscopy (CE) is a minimally invasive examination tool for evaluation of the small intestine [1–7], esophagus [8], and colon [9,10]. CE is considered to be the first-line tool to examine the small intestine, with a reported diagnostic yield of 30–70% [2–7,11,12]. However, one limitation is that 10–30% of small intestinal CE examinations cannot evaluate the entire small intestine up to the terminal ileum because of limited battery life. It was reported that an increased completion rate of CE may increase diagnostic yield [13,14]. Many clinical trials have clarified methods for shortening gastric transit time (GTT) [15–17] and small bowel transit time (SBTT) [18–22] during CE.
Completion rates of CE may be increased with metoclopramide and mosapride by reducing GTT and with erythromycin by reducing GTT and/or SBTT [15–20]. Chewing gum is a unique method that may shorten SBTT, but it is still controversial [21,22]. Oral purgatives, such as polyethylene glycol and lubiprostone, may reduce SBTT and improve visualization of the small intestine [23–25], but they have not been fully reported. These trials compared GTT and/or SBTT before and after interventions, such as strengthening gastric and small intestinal movement by prokinetics. However, no studies have demonstrated the repeatability of GTT and SBTT in the same subjects. Before evaluating these reports, it would be necessary to clarify whether comparison of GTT and/or SBTT in the same subjects before and after treatment is reasonable. If GTT and/or SBTT were not repeatable, evaluation of reports that attempted to reduce GTT and/or SBTT would be questionable.
Furthermore, knowing the factors that affect SBTT is important [26–29]. Fireman et al. retrospectively analyzed 790 CE cases, including 87 healthy volunteers, and reported that SBTT was shorter in the younger (under 40 years old) group than in the elderly group. Papadopoulos et al. prospectively analyzed SBTT in 120 consecutive CE cases and reported that aging did not affect SBTT or completion rate of CE. Madsen et al. investigated the association between GTT/SBTT and physical factors using radiolabelled cellulose fiber and plastic particles and reported that sex, age, and body mass index (BMI) did not affect SBTT, but BMI was inversely associated with gastric emptying time. Another report showed that body weight did not affect the SBTT of CE in dogs.
A retrospective, case-control study by Endo et al. showed longer SBTT and lower cecal completion rate in patients with pre-abdominal surgery compared with patients without pre-abdominal surgery [30]. Shibuya et al. analyzed 76 CE cases and reported that lower physical activity was a risk factor that decreased completion rate of CE [31]. Overall, the association between physical factors and SBTT has not been fully studied and remains controversial.
The first aim of this study was to clarify the repeatability of GTT and SBTT of CE. The second aim was to clarify the factors that influence SBTT by analyzing data from a double-blinded randomized controlled trial (RCT) that we formally conducted to compare the number of small intestinal injuries caused by non-selective and selective non-steroidal anti-inflammatory drugs (NSAIDs).
Methods
We analyzed the data from an RCT that we previously conducted to compare the number of small intestinal mucosal injuries caused by non-selective and selective NSAIDs. The details and main outcome of the RCT were reported by Fujimori et al. [32], and are described briefly in our report.
Study subjects
Of 230 healthy candidates screened by a medical check, including physical examination, laboratory tests, and medical history from April 2012 to March 2013, a total of 150 subjects were eligible for this study. All subjects provided written informed consent for this study before undergoing baseline CE. This study was approved by the ethics committee of Nippon Medical School and Kyushu Clinical Pharmacology Research Clinic Institutional Review Board. The study was registered at UMIN registry, a numeric system for the identification of RCTs conducted worldwide (ID: 000007936).
Inclusion and exclusion criteria
Inclusion criteria: Study subjects were healthy Japanese volunteers whose age at the time of informed consent was 40–70 years old. “Healthy” was defined as 1) receiving no treatment; and 2) having no clinically relevant abnormalities as identified by a detailed medical history and full physical examination, including blood pressure, pulse rate, 12-lead electrocardiogram, laboratory tests, and screening fecal occult blood test.
Exclusion criteria: Subjects who had a history of gastrointestinal ulcer; gastrointestinal operation; malignancy; cardiac disease; cerebrovascular disease; diabetes; known hypersensitivity or allergic disease to celecoxib, aspirin, and other NSAIDs or lansoprazole; and gastrointestinal disease within one month or current gastrointestinal symptoms were excluded. Subjects who had been treated with NSAIDs including aspirin, anti-ulcer medication, antacids, steroids, or antibiotics within one month prior to the first day of administration of the study medication were excluded.
Study protocol
All eligible subjects were randomly assigned to two groups, the celecoxib group and the loxoprofen group. Age, sex, and positive Helicobacter pylori infection were equally distributed between the groups. After randomization, baseline CE was performed. After baseline CE, the celecoxib group was given celecoxib (100 mg) and lactose placebo capsules twice a day. The loxoprofen group was given loxoprofen capsule (60 mg) three times a day and lansoprazole capsule (15 mg) once a day. Small intestinal injuries were evaluated using a video capsule system (PillCam SB2, Given Imaging Ltd., Yoqneam, Israel). Baseline CE was performed on day 1, and post-treatment CE was performed within three days after completion of the drug regimen in all subjects who completed the study.
All video image files were anonymized and were evaluated by three skilled reviewers, who were blinded to information about the subjects. Mucosal injury was defined as mucosal breaks in the small intestine with slough and surrounding erythema. After analysis of the video files, the number of mucosal injuries in each anonymous data file was determined by consensus of the three reviewers. GTT was defined as the time from visualization of the first gastric CE image to visualization of the first duodenal CE image. SBTT was defined as the time from visualization of the first CE image of the duodenal mucosa after passing through the pylorus to the first CE image of the cecum. If the capsule did not reach the cecum, SBTT was calculated from the last picture recorded.
Analysis of GTT and SBTT repeatability
From the data of CE examination, the subjects who completed both baseline and post-treatment CEs were eligible for the first evaluation; the analysis of GTT and SBTT repeatability. First, the mean GTT/SBTT of baseline and post-treatment CEs were compared. Second, the correlation between GTT/SBTT of baseline and post-treatment CEs in whole subjects and the correlation between GTT/SBTT of baseline and post-treatment CEs in each treatment group were analyzed.
Investigating factors affecting SBTT
From the data of CE examination, the subjects who completed baseline CE were eligible for the second evaluation; the analysis of associations between SBTT and sex, age, height, body weight, BMI, pre-abdominal surgery, and blood sampling data. From the data of CE examination, the subjects who completed both baseline and post-treatment CEs were eligible for the third evaluation; the analysis of association between SBTT and the presence of small intestinal mucosal injury, except the case that CE does not reaching to the cecum.
Statistical analysis
The association between GTT/SBTT values of baseline and post-treatment CE (the first evaluation) was analyzed by paired t-test and Spearman’s rank correlation test. Of the second evaluation, the associations between baseline CE SBTT and age, height, body weight, BMI was analyzed by linear regression analysis, the associations between baseline CE SBTT and sex and pre-abdominal surgery were analyzed by the Wilcoxon rank-sum test. The association between post-treatment CE SBTT and the presence of small intestinal mucosal injury (the third evaluation) was analyzed by Wilcoxon rank-sum test. Data were expressed as mean ± SD; p-values < 0.05 were considered to be statistically significant. We calculated our results using STATA ver. 10 (College Station, TX, USA).
Results
Analysis of subjects
Among a total of 150 subjects who underwent baseline CE, the mean age was 48.8 ± 6.5 years, mean height was 164 ± 8.2 cm, mean body weight was 59.8 ± 11.0 kg, and mean BMI was 22.0 ± 3.0; sex distribution was equal. There were 74 patients in the celecoxib group and 76 patients in the loxoprofen group; there were no statistical differences between the two groups in baseline characteristics, and no statistical differences in characteristics between baseline and post-treatment CEs, except for the blood sampling data and the number of subjects who had small intestinal mucosal injuries (Table 1).
Comparison of subjects during baseline CE and post-treatment CE
Comparison of subjects during baseline CE and post-treatment CE
CE, capsule endoscopy; GTT, gastric transit time; SBTT, small bowel transit time SD, Standard Deviation. ∗Wilcoxon signed-rank test. †Paired t-test. N.A., not available; N.S., not significant.
In the baseline CE group, two subjects were excluded from the study because one CE did not reach the duodenum and one CE had technical failure. Therefore, 148 subjects remained as eligible subjects for the second evaluation. However, before post-treatment CE, two subjects were excluded from the study because of influenza and non-compliance to the protocol. Therefore, a total of 146 subjects (73 in the celecoxib group and 73 in the loxoprofen group) remained eligible for the first and the third evaluation. The capsule endoscope reached the cecum in 142 subjects of the post-treatment CE group. There was no adverse event in both groups throughout the study.
There was no difference between mean SBTTs of baseline CE and post-treatment CE (241 ± 15 vs. 244 ± 16, p = 0.75) as shown in Table 1. There was no significant difference between the celecoxib group and loxoprofen group in terms of SBTT of post-treatment CE (252 ± 108 vs. 236 ± 80, respectively; p = 0.3). In each group, there was no significant difference between SBTTs of baseline and post-treatment CEs. The SBTT plot for each subject is shown in Fig. 1. There was moderate positive correlation between baseline CE and post-treatment CE (𝜌 = 0.47, p < 0.001). There was positive correlation between baseline and post-treatment CE in both the celecoxib group (𝜌 = 0.40, p < 0.001) and the loxoprofen group (𝜌 = 0.57, p < 0.0001) (Fig. 1).

Correlation between small bowel transit time (SBTT) of baseline and post-treatment capsule endoscopies (CEs). Moderate positive correlation is shown between SBTTs of baseline and post-treatment CEs in the celecoxib group, in the loxoprofen group, and in all subjects. Regression lines: dash line, celecoxib group; long-dash line, loxoprofen group; solid line, all subjects.
There was no significant difference between the mean GTTs of baseline and post-treatment CEs (Table 1). In each group, there was no significant difference between the GTTs of baseline and post-treatment CEs. There was slight positive correlation between the GTTs of baseline CE and post-treatment CE (𝜌 = 0.22, p < 0.01, Fig. 2).
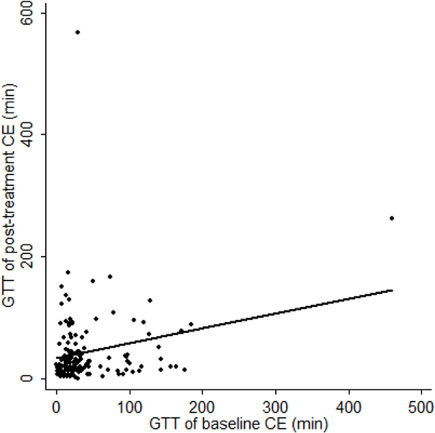
Correlation between gastric transit times (GTTs) of baseline and post-treatment CEs. Slight positive correlation is shown between GTTs of baseline and post-treatment CEs.
Age, height, body weight, and BMI had no association with SBTT (Table 2). Hemoglobin and serum blood urea nitrogen (BUN) showed mild association with SBTT (Table 3). Sex and history of abdominal surgery had no association with SBTT (Table 4). SBTT of post-treatment CE was not associated with the presence of small intestinal mucosal injury and treatment group (Table 5).
Association between physical factors and SBTT of baseline CE (n = 148)
Association between physical factors and SBTT of baseline CE (n = 148)
SBTT, small bowel transit time; BMI, body mass index.
Association between blood sampling data and SBTT of baseline CE (n = 148)
WBC, white blood cell; BUN, blood urea nitrogen.
Association of SBTT of post-treatment CE with sex and history of abdominal surgery (n = 148)
SBTT, small bowel transit time; CE, capsule endoscopy.
Association of SBTT of post-treatment CE with mucosal breaks and treatment group (n = 146)
SBTT, small bowel transit time; CE, capsule endoscopy; PPI, proton pomp inhibitor 1) In this evaluation, only the subjects in whom the entire small intestine were evaluated in both baseline and post treatment CEs were included.
In this study, SBTT of CE was clarified to be repeatable in the same subject regardless of prior NSAID treatment. Until recently, several studies reported that SBTT may be shortened by erythromycin [18–20], chewing gums [21,22], oral purgatives [23–25], and physical activity [31]. However, the reproducibility of SBTT in repeated CE has not been confirmed. If SBTT is not repeatable, the utility of the previous reports on shortening SBTT would be questionable. To our knowledge, this is the first report on SBTT repeatability using data from an RCT on healthy volunteers. The results of this study may enable more accurate evaluation of methods that can shorten SBTT, such as prokinetics.
Although there was reproducibility of GTT in repeated CE, correlation was poor in this study. GTT was within 45 min in 75% of subjects who underwent baseline CE, and within 50 min in 75% of subjects who underwent post-treatment CE. Usually, stagnation of a capsule in the stomach for more than 2 h during CE becomes problematic. Because CEs passed through the stomach in a relatively short time and post-treatment CEs were performed after NSAIDs administration in this study, it may be hard to show correlation by analyzing GTT. Unfortunately, our result did not represent a clear correlation between baseline and post-treatment CEs in terms of GTT. Inclusion of more subjects and performing a second CE in untreated patients is desired and may clarify the repeatability of GTT in CE.
In addition, the results of mean GTT and SBTT in both baseline and post-treatment CE in this study were quite similar as many previous reports [20–28] –showing mean GTT of CE as 30–50 minutes, especially 40 minutes in healthy volunteers, and mean SBTT of CE as 200–300 minutes, especially about 4h in healthy volunteers.
In this study, there was moderate correlation between the SBTTs of baseline and post-treatment CEs, but the mechanism of CE movement in the small intestine is still unclear. Recently, the migrating motor complex (MMC) was reported to be the mechanism for fasting gastrointestinal movement [33]. Phase III of intestinal MMC is related to fasting bowel movement and occurs every 90–120 min, but the mechanism of MMC regulation is unknown. SBTT during procedures may depend on MMC. If the repeatability of CE movement in the small intestine depends to a large extent on phase III of intestinal MMC, this phase may have a relatively accurate rhythm. Clarifying the mechanism of phase III MMC may contribute to the control of SBTT.
To our knowledge, this is the first report to analyze the factors that may affect SBTT in healthy subjects. In this study, age, sex, height, body weight, and BMI did not affect SBTT at all. Fireman et al. previously reported that aging affected SBTT; this study defined aging as over 40 years old and analyzed a large number of subjects, many of whom had small intestinal disease [26]. In contrast, Papadopoulos et al. reported that aging did not affect SBTT; in that report, sample size was small and included patients with small intestinal disease, not healthy subjects [27]. Our study analyzed healthy subjects, but the range age of the subjects was limited at 40–70 years. Further analysis of a large population with a wide age range is needed.
Body weight and BMI did not influence SBTT in this study. Boillat et al. reported a relationship between body weight and gastrointestinal transit time in six dogs of various sizes [29]. In contrast, Madsen et al. previously reported that BMI did not affect SBTT [28]. In conjunction with our results, physical factors, such as height, weight, and BMI may not affect SBTT of CE in adults. Endo et al. previously reported that history of abdominal surgery affected SBTT [30]; however, our results showed otherwise. This may be explained by the fact that the previous abdominal surgeries of our subjects, which included herniorrhaphy and acute appendicitis, may not be enough to evaluate the effects on SBTT.
Hemoglobin and BUN showed association with SBTT. Our study revealed that decreasing hemoglobin is associating with shorter SBTT, and increasing BUN is associating with longer SBTT. Those results might suggest insufficient renal function leads to reducing intestinal motility, but more large data of SBTT with renal dysfunction subjects is needed.
There have been no reports on the association between SBTT of CE and the presence of small intestinal mucosal injury. It was reported that NSAIDs cause intestinal hypermotility in rats [34], and shorten small intestinal transit time in dogs by accelerating myoelectrical activity [35]. But in contrast to those experimental data, in clinically, our results showed taking NSAIDs nor the presence of small intestinal injury does affect SBTT at all in healthy human subjects.
There were some limitations in this study. First, baseline and post-treatment CEs were not entirely performed under the same conditions. Nevertheless, there were no differences in SBTT between both the groups and between baseline and post-treatment CEs in each group. Therefore, as mentioned above, we consider that the effect of taking NSAIDs on the SBTT was small. A second limitation was the limited age range of the subjects, which may have affected the association of age and SBTT. The third limitation was the battery of the capsules. In the study, five CE examinations were unable to reach the cecum and may have confounded the results. In the celecoxib group, subjects were taking lactose as placebo, but its dose was very low and we consider it was not affecting our results.
Conclusion
During CE, repeatability was moderate for SBTT and low for GTT. The factors affecting SBTT remain to be clarified. Nevertheless, our results may be useful for investigators of methods to shorten GTT and/or SBTT. Further studies are desired to evaluate the repeatability of GTT and SBTT under similar conditions of the gastrointestinal tract.