
Abstract
OBJECTIVE:
We conducted ultrasonography (US) examination for asymptomatic elbow injuries in judo athletes to confirm availability of US screening for elbow.
MATERIALS AND METHODS:
One hundred and thirty-two black belts in judo (85 males and 47 females; mean age, 20.0 ± 1.6 years) participated in this screening. Forty-eight participants had a history of elbow injury (elbow-injury group), and 84 did not (no-elbow-injury group). All participants completed a survey in the form of a questionnaire. Subsequently, US scanning of both elbows was performed.
RESULTS:
The maximal thickness of the medial collateral ligament of both elbows was significantly larger in the elbow-injury group than in the no-elbow-injury group. The width of the joint space was significantly larger in the right radiohumeral joint in the elbow-injury group than in the no-elbow-injury group. Combination injuries involving ligament and bone and those involving both the medial and lateral collateral ligaments were most commonly seen in both elbows in the elbow-injury group; however, these combined lesions of both elbows were also found in the no-elbow-injury group.
CONCLUSIONS:
Because US screening can reveal abnormalities of the asymptomatic elbow, US is recommended as a complementary imaging modality that is useful for evaluation of elbow injuries in athletes.
Introduction
With recent developments in ultrasonography (US), ligamentous injuries, fractures of ligament origins or insertions, and arthritis can be visualized easily anywhere. Although acute ruptures of ligaments can be visualized circumstantially with magnetic resonance imaging (MRI) [1], there are limitations to MRI, such as expense and time. Advantages of US compared with MRI include lower cost, greater availability, better spatial resolution, noninvasiveness, and the ability to perform dynamic studies. Although there is already a large amount of literature about US findings in baseball elbow, there are very few studies on elbow injuries in judo athletes.
The anterior bundle of the medial collateral ligament (MCL) is the strongest component that predominantly resists valgus stress to the elbow [2–4]. It arises from the medial epicondyle and inserts on the medial aspect of the base of the coronoid process of the ulna. In contrast to this, the lateral ulnar collateral ligament (LUCL) of the lateral compartment serves as the main stabilizer of the elbow against varus stress [5]. It arises proximally from the lateral epicondyle and attaches distally to the supinator crest of the ulna. The MCL, which is the major stabilizer of the elbow joint against valgus stress, is most commonly injured in pitching elbows. Little leaguer’s elbow involves MCL injuries, common flexor tendon origin injuries and ulnar neuritis [6,7]. Elbow injuries in judo occur during arm lock maneuvers that enforce valgus stress and result in significant injury to the medial compartment; however, combinations of medial and lateral ligament injuries that result in joint laxity can occur. Therefore, we screened judo black belts with US for elbow injuries at a stage at which the athletes were not yet symptomatic but at which abnormal findings were detectable with US. Thus, the purpose of this study was to test the hypothesis that US screening can reveal abnormalities of the asymptomatic elbow in judo athletes.
Materials and methods
One hundred and thirty-two black belts in judo belonging to the judo club at our university (85 males and 47 females; mean age, 20.0 ± 1.6 years) participated in this screening. Any athletes who were under medical treatment for elbow injury were not included in this observational study. This clinical study was approved by the institutional ethics review board prior to its commencement and was conducted in accordance with the ethical tenets outlined in the 1964 Declaration of Helsinki for research involving human subjects. Written informed consent was obtained from all patients after a detailed explanation of the method of examination was provided to them.
All participants completed a survey in the form of a questionnaire. The questionnaire items included age, gender, body weight, years of experience in judo, etiology of the elbow injury, grappling hand and dominant hand as baseline data. In addition, any history of elbow pain or numbness of the ulnar hand due to ulnar nerve irritation or entrapment was explored. Subsequently, US scanning (Noblus, Hitachi Co., Ltd., Tokyo, Japan) of both elbows of each participant was performed by an experienced professional instructor. The anterior bundle of the MCL and the LUCL of the lateral collateral ligament (LCL) are the primary stabilizers of the elbow joint. Due to the chronic nature of the injuries evaluated in this research, hypertrophy of the involved ligaments may have occurred after the injuries, resulting in joint laxity. Therefore, the maximal thickness of both the anterior bundle of the MCL and LUCL of the LCL and the width of the ulnohumeral and radiohumeral joint spaces were measured. Furthermore, lesions of the coronoid and olecranon fossae, including effusion and loose bodies, lesions of the trochlea, capitellum, olecranon cartilage, subchondral bone, common flexor and extensor origins, and the tricipital tendon were observed. After US examination, the range of motion (ROM) of the elbow, including extension and flexion, was measured.
The participants were divided into two groups: those with and those without a history of elbow injury. For the statistical comparison of the baseline data, such as age, body weight and number of years of experience in judo, between the two groups, the Mann-Whitney U-test was used. The gender, grappling hand, dominant hand, elbow pain and numbness of the ulnar hand in the two groups were compared using the Chi-squared test of independence. For comparison of US measurements of the maximal thickness of the anterior bundle of the MCL and the LUCL, the width of the ulnohumeral and radiohumeral joint space, and the ROM of both elbows, the Mann-Whitney U test was used. Furthermore, the number of lesions of the coronoid and olecranon fossae, trochlea, capitellum, radial head, olecranon, common flexor and extensor origins, and tricipital tendon observed by US were compared using the Chi-squared test of independence. A p value of <0.05 was considered statistically significant.
Results
Of the 132 judo athletes, 48 participants had a history of elbow injury (28 males and 20 females; mean age, 20.0 ± 1.5 years), and 84 did not (57 males and 27 females; mean age, 20.0 ± 1.7 years). There was no significant difference in the baseline data, including age, gender, number of years of experience in judo, body weight, grappling hand or dominant hand (Tables 1–3). The etiology of the elbow injuries is summarized in Table 4. Ligamentous injuries were common on both sides of the elbow; however, bone and joint injuries were also evenly distributed across the elbow. Elbow pain and numbness of the ulnar hand are summarized in Tables 5 and 6, respectively. The ulnar hand numbness is suspected due to ulnar nerve entrapment or irritation. Both symptoms were significantly more common in the group with a history of elbow injury than in the group without a history of elbow injury.
The baseline data of judo athletes
The baseline data of judo athletes
With elbow injury: the group with a history of elbow injury. Without elbow injury: the group without a history of elbow injury. Average ± SD.
The grappling hand of judo athletes
Rt: right, Lt left.
The dominant hand of judo athletes
The etiology of elbow injury
OCD: osteochondritis dissecans.
The elbow pain
Flx: flexion, Ext: extension. ∗∗ p < 0.01.
The ulnar hand numbness in association with the elbow pain
∗ p < 0.05.
The maximal thickness of the anterior bundle of the MCL and the LUCL of the LCL and the width of the ulnohumeral and radiohumeral joint space measured by US are summarized in Table 7. The maximal thickness of the MCL of both elbows was significantly larger in the group with a history of elbow injury than in the group without a history of elbow injury. However, there was no significant difference in the maximal thickness of the LCL in both groups. The width of the joint space was significantly larger in the right radiohumeral joint in only the group with a history of elbow injury. US findings of lesions of the MCL and LCL, the ulnohumeral joint (UHJ) and radiohumeral joint (RHJ), and the coronoid and olecranon fossae are summarized in Table 8. No hydroarthrosis was found in either group. There were significant differences in the number of lesions of the left LCL and RHJ and the left olecranon fossa in both groups. Combination injuries involving ligament and bone and those involving both the MCL and LCL (Fig. 1) were most commonly seen in the group with a history of elbow injury, and there was no significant difference between groups. In addition irregularity of the common flexor and extensor muscle origin, which was occasionally accompanied by avulsed fragments from the origin, was seen. Of the six cases that showed symptoms of both elbow pain and numbness of the ulnar hand, two cases of ulnar nerve dislocation (Fig. 2) and two cases of ulnar nerve entrapment (Fig. 3) were detected with US. In other cases the ulnar nerve could not be traced in the hyperechoic cubital tunnel. As a pathognomonic finding of the elbow injury in judo, irregularity of the proximal posterior capitellum was seen in some cases (Fig. 4). ROM of the elbow, including flexion and extension, is summarized in Table 13. Flexion of both elbows was limited in both groups, and there was no significant difference in the ROM of the elbow between the groups.
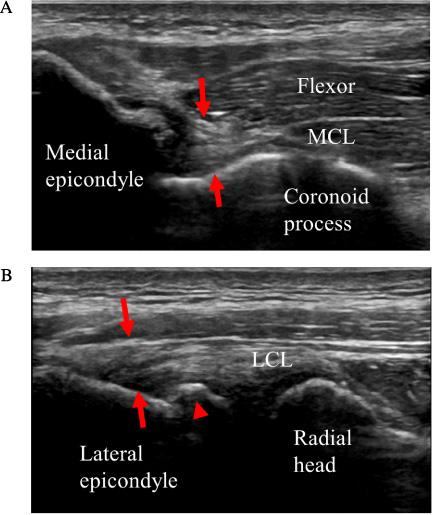
US findings of combination injuries involving ligament and bone and those involving both the MCL and LCL in the group with a history of elbow injury. (A) Hypertrophy of the MCL origin (arrow) suspected due to scar formation after the ligamentous injury. (B) Hypertrophy of the LCL origin (arrow) suspected due to scar formation after the ligamentous injury. Bony protrusion of the lateral epicondyle (arrow head) suspected due to avulsion fracture is also seen. MCL: medial collateral ligament, LCL: lateral collateral ligament.
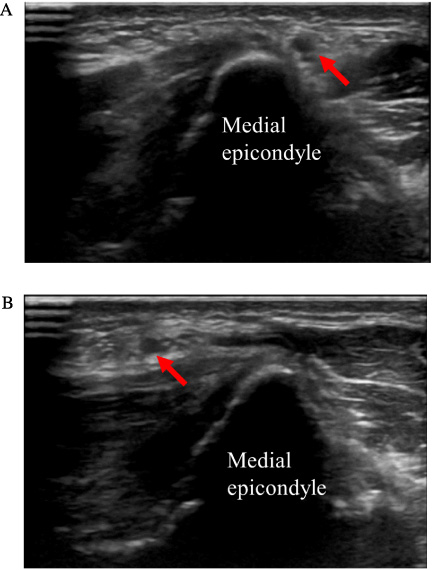
US finding of ulnar nerve dislocation in the case that showed symptoms of both pain and numbness of the ulnar hand. (A) The ulnar nerve is located on the distal side of medial epicondyle (arrow) when the elbow is extended. (B) The ulnar nerve transfers to the proximal side of medial epicondyle (arrow) when the elbow is flexed.
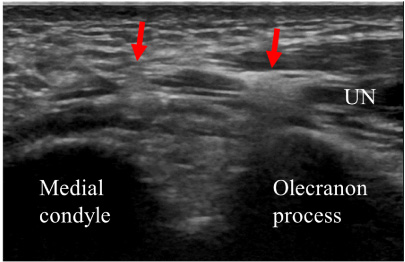
US finding of ulnar nerve entrapment in the case that showed symptoms of both pain and numbness of the ulnar hand. The ulnar nerve is compressed at two points in the cubital tunnel (arrow).
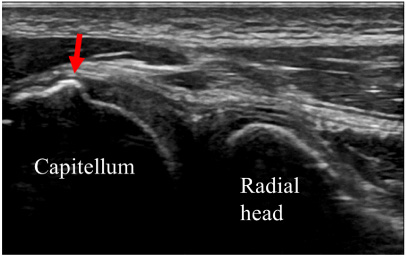
Bony protrusion of the posterior capitellum (arrow) suspected due to old fracture.
The maximal thickness of the anterior bundle of the medial collateral ligament and the lateral ulnar collateral ligament of the lateral collateral ligament, and the width of the ulnohumeral and radiohumeral joint space
MCL: the anterior bundle of the medial collateral ligament, LCL: the lateral ulnar collateral ligament of the lateral collateral ligament, UHJ: ulnohumeral joint space, RHJ: radiohumeral joint space. Average ± SD. ∗ p < 0.05, ∗∗ p < 0.01.
Medial sweeping. The medial elbow is evaluated with the patient’s forearm placed in forceful external rotation and extension or slight flexion
MCL: the anterior bundle of the medial collateral ligament, UHJ: ulnohumeral joint space.
Lateral sweeping. The lateral elbow is evaluated by placing the elbow in flexion with the arm internally rotated
LCL: the lateral ulnar collateral ligament of the lateral collateral ligament, RHJ: radiohumeral joint space.
Combined lesions observed by both medial and lateral sweeping
Posterior sweeping. The posterior elbow is evaluated with the joint positioned in 90 degree of flexion, the forearm fully pronated, and the palm resting on a table. To evaluate the ulnar nerve, the patient is prone with the arm adducted by the side and internally rotated
∗ p < 0.05.
Anterior sweeping. The anterior elbow is evaluated with the joint extended and the forearm is supinated
OCD: osteochondritis dissecans of the capitellum.
ROM of the elbow
Average ± SD.
Chronic injuries to the MCL and LCL due to repetitive microtrauma that have an insidious onset may be more common in judo athletes, similar to baseball pitchers [8], and the ligaments undergo degeneration, calcification and low-grade tears, which will eventually lead to elbow joint instability [8–10]. In this research, almost all cases with cubitalgia belonged to the group with a history of elbow injury. The maximal thickness of the MCL of both elbows was significantly larger in the group with a history of elbow injury than in the group without a history of elbow injury, which suggests a previous history of unconscious MCL injury in the dominant or grappling hand. There was no significant difference in the maximal thickness of LCL between groups; however, the width of the joint space of the right RHJ was significantly larger in the group with a history of elbow injury than in the group without a history of elbow injury. These results suggest the possibility of a previous history of LCL injury in the dominant hand. Combination injuries involving ligament and bone and those involving both the MCL and LCL were most commonly seen in both elbows in the group with a history of elbow injury; however, these combined lesions of both elbows were also prominent in the group without a history of elbow injury. These results suggest that numerous judo athletes may unknowingly sustain serious elbow injuries and that US screening is effective for detection of such ligamentous and bony lesions. Significant trauma to the elbow that is associated with high-grade injuries to the MCL often causes rupture of the roof of the cubital tunnel, formed by Osborne’s ligament, and results in displacement of the ulnar nerve. In these cases, numbness of the ulnar hand that is often accompanied by pain may occur due to ulnar nerve irritation, and in some cases, ulnar nerve palsy progresses. In this study, eight cases in the group with a history of elbow injury showed symptoms of elbow pain and numbness of the ulnar hand, and only two cases showed symptoms of numbness of the ulnar hand in the group without a history of elbow injury. Of these cases in the group with a history of elbow injury, two cases of ulnar nerve dislocation and two cases of ulnar nerve entrapment were detected with US. In other cases, the ulnar nerve could not be traced in the hyperechoic cubital tunnel. These findings suggest that the ulnar nerve can be clearly identified on US when fluid, such as synovial fluid or a hematoma, surrounds the nerve and its branches; however, identification of the ulnar nerve becomes difficult when adhesions of the nerve to the surrounding tissue exist.
The advantages of US over radiography and MRI include its portability, lack of radiation, and ability to image the anterior bundle of the MCL and the LUCL of the LCL directly to visualize degeneration, hypertrophy and calcification of the ligament. US can also depict other abnormalities, including medial or lateral epicondylitis, flexor or extensor muscle injuries and ulnar neuropathy. We examined the maximal thickness of the anterior bundle of the MCL and the LUCL of the LCL and the width of the UHJ and RHJ joint space at rest. The maximal thickness of the MCL of both elbows was significantly larger in the group with a history of elbow injury than in the group without a history of elbow injury. However, the width of the joint space was significantly larger in the right RHJ only in the group with a history of elbow injury. Considering that stress US examination can detect a significant difference in the width of the UHJ in pitching and nonpitching arms [9], dynamic US with valgus and varus stress may be a useful procedure that provides a rapid means of evaluating elbow laxity due to ligament injuries in judo athletes. Given how common elbow problems are in judo athletes, it is reasonable to combine dynamic US with US at rest for screening to detect chronic repetitive elbow injury. Commercial devices exist that can standardize the amount of valgus stress applied to each elbow. However, Sasaki et al. successfully showed that the medial joint space was significantly wider on the throwing side than on the contralateral side and showed that there was more laxity with valgus stress without these devices [12]. These authors used a 10-MHz transducer with the elbow in 90° of flexion and used gravity stress. Because of strict time constraints, we were unable to perform this test in this study. We would like to address this limitation in the next screening of the elbows of judo athletes.
Conclusion
We screened for elbow injuries in judo athletes with US at a stage at which the athletes were not yet symptomatic but at which findings were detectable with US. Combination injuries involving ligament and bone and those involving both the MCL and LCL were most commonly seen in both elbows in the group with a history of elbow injury; however, these combined lesions of both elbows were also prominent in the group without a history of elbow injury. These results suggest that numerous judo athletes have unknowingly suffered from elbow injuries to varying degrees and that US screening can reveal abnormalities of the asymptomatic elbow in athletes. US is recommended as a complementary imaging modality that contributes substantially to screening athletes for elbow injuries.
Ethical approval
This study was approved by the Teikyo University of Science Review Boards (no. #16024) prior to its commencement and was conducted in accordance with the ethical tenets outlined in the 1964 Declaration of Helsinki for research involving human subjects.
Conflict of interest
The authors declare that no biases exist for any author.