
Abstract
BACKGROUND:
After total knee arthroplasty (TKA), the femur tends to be located posteriorly under weight-bearing (WB) conditions, and a paradoxical femoral anterior motion occurs, leading to joint instability.
OBJECTIVE:
We aimed to clarify factors which affect the postoperative femoral anteroposterior position relative to the tibia under WB conditions (A-P position) in medial pivot (MP) TKA.
METHODS:
Among 126 knees (81 women) with primary TKA using MP prosthesis for varus osteoarthritic knees, 70 knees had cruciate-retaining inserts (CR) with the reduced conformity and 56 knees had cruciate-substituting inserts (CS) with the full conformity. Using the three-dimensional (3D) assessment system, the associations between the A-P position and the factors including pre- and postoperative lower extremity alignment, component positions, and posterior femoral condylar offset (PCO), were assessed regarding the type of inserts.
RESULTS:
Significant correlations were seen between the A-P position and posterior tibial slope (PTS), medial PCO, and lateral PCO. Regarding the difference between the two inserts, the PTS, medial PCO, and lateral PCO significantly correlated with the A-P position in the CR, but only the PTS correlated in the CS.
CONCLUSIONS:
The increased PTS and decreased PCO were the dominant factors for the A-P position in MP TKA.
Keywords
Introduction
In a routine total knee arthroplasty (TKA), since the anterior cruciate ligament (ACL) is cut, the anteroposterior stability of the joint depends on the implant and insert shapes, and the tension in the soft tissue, such as the collateral ligaments, posterior cruciate ligament (PCL), and capsule, which surround the knee joint [1].
It has been reported that in ACL-deficient knees, during nearly full extension the femoral condyle was located significantly more posteriorly than in the contralateral uninjured knees, and the range of anteroposterior translation of the medial femoral condyle was greater than that of contralateral uninjured knees [2]. Similarly, in knees after TKA, theoretically, the femur tends to be positioned posteriorly under weight-bearing conditions, and a paradoxical femoral anterior motion from full extension to mid-range flexion occurs, leading to joint instability [3,4]. Therefore, it is crucial to prevent the femoral posterior location by substituting anteroposterior stability in modern TKA.
In knees after TKA, there have been few reports in terms of the postoperative femoral anteroposterior position relative to the tibia under weight-bearing conditions (A-P position) in a three-dimensional (3D) space, and it remains unknown what kind of factors, such as the component position and lower extremity alignment, affect the postoperative A-P position. Additionally, it is unknown how the different insert types (cruciate-retaining (CR) versus [vs.] cruciate-substituting [CS] inserts) in the medial pivot prosthesis (Fig. 1) affect the postoperative A-P position. The type of prothesis, absence of PCL, and posterior tibial slope have been reported as the factors affecting the tibiofemoral anteroposterior relationship in two-dimensional assessment using plain radiography or fluoroscopy in conventional TKA [3–8]. To our knowledge, this is the first study to investigate the factors affecting the postoperative A-P position in the medial pivot prosthesis based on the strict 3D measurement under weight-bearing conditions, considering the type of insert.

Configuration of the two types of inserts. Medial sagittal section of the cruciate-retaining (CR) insert and cruciate-substituting (CS) insert. The CS insert has a full conformity with higher posterior and anterior lips than the CR insert.
The postoperative evaluation of lower extremity alignment, such as the A-P position, by plain radiography or computed tomography (CT) remains challenging [9]. For an accurate evaluation, the pre- and postoperative lower extremity alignment should be three-dimensionally assessed under weight-bearing conditions and by identical coordinate system before and after TKA, which are, as yet, impossible to achieve by common modalities. This author group developed a 3D lower extremity alignment assessment system under weight-bearing conditions as per previous studies [10–12]. This system can automatically assess the lower extremity alignment under weight-bearing conditions, component position, and change of the femoral posterior condylar shape with high accuracy [10]. This method can identify problems previously undetected by conventional two-dimensional (2D) modalities such as X-ray, CT, or magnetic resonance imaging (MRI) under non-weight-bearing conditions.
The objective of this study was to prove the hypotheses that, in the medial pivot prosthesis, (1) the postoperative A-P position would correlate with several factors among the pre- and postoperative lower extremity alignment under weight-bearing conditions, component positions, and posterior femoral condylar shape, and (2) the former relations would differ according to the type of insert (CR vs CS inserts).
Study design, population, and prostheses
All study participants provided informed consent, and ethical approval was obtained from the relevant institutional review board. The inclusion criterion was primary TKAs for varus knee osteoarthritis (OA). The exclusion criteria were patients with valgus knee OA, secondary OA after trauma, rheumatoid arthritis, previous knee surgery (e.g., high tibial osteotomy), osteosynthesis, excessive joint laxity based on the New Knee Society Score (varus-valgus instability >5 mm and anteroposterior instability >5 mm) [13], hyperextension >10°, multidirectional instability, and an absence of a complete set of outcome data. In this study, 126 knees (81 women) with medial pivot implants were examined. The mean age of the patients was 75 ± 7 years, with a mean follow-up duration of 54 ± 35.9 months, and a mean body mass index of 26.5 ± 4.0 kg/m2 (Table 1). Twenty-nine knee replacements were performed with the Advance® Medial Pivot Knee system (MicroPort Orthopedics Inc., Arlington, TN, USA) and 97 with the Evolution® Medial Pivot Knee system (MicroPort Orthopedics Inc., Arlington, TN, USA). In terms of the differences of these two medial pivot protheses, although the shapes and conformity of the femoral component are slightly different only in the deep knee flexion range >90°, they are almost the same in the extension range. We investigated the A-P position in knee extension; therefore, we treated these two protheses as the same. These prostheses incorporate different insert types in the medial side, consisting of the CR insert, which has a high anterior lip and low posterior lip, and the full conformity CS insert, which has high posterior and anterior lips to restore medial pivot motion without compromising anteroposterior stability [14,15] (Fig. 1). CR inserts were used for 70 knee replacements and CS inserts for 56 knee replacements. The PCL was sacrificed with CS inserts when the intraoperative flexion gap was tight but preserved with CR inserts.
Demographic data
Demographic data
BMI, body mass index; CR, cruciate-retaining; CS, cruciate-sustaining; SD, standard deviation; HKA, hip-knee-ankle angle; Cor HKA, hip-knee-ankle angle in the coronal plane; Sag HKA, hip-knee-ankle angle in the sagittal plane; F-T rotation, femorotibial rotation; A-P position, standardized femorotibial anteroposterior position; MPCO, medial posterior condylar offset; LPCO, lateral posterior condylar offset; PCO, posterior condylar offset; vs., versus. ∗ p < 0.05.
The 3D preoperative planning software (JIGEN®, LEXI Inc., Tokyo, Japan) was used to simulate the size and setting position of the femoral and tibial components. This author group developed a method to control the component positions using several mechanical instruments to reproduce the 3D preoperative planning [10–12]. This method can be achieved by the accurate insertion of femoral and tibial intramedullary (IM) rods, thereby controlling the insertion point, depth, and direction three-dimensionally according to the preoperative planning. In the coronal plane, the distal cutting surface was perpendicular to the mechanical axis. The femoral component was slightly flexed by 2–3° in the sagittal plane to avoid anterior cortical notching. The rotational alignment of the femoral component was based on the surgical epicondylar axis (Fig. 2). The proximal tibia was resected at 90° to the longitudinal axis of the tibial shaft in the coronal plane using the intramedullary alignment rod. The rotational position of the tibial component was determined using the anteroposterior axis described by Akagi et al. [16]. The tibial posterior slope was parallel to the lateral tibial slope [17,18] in the former 71 knees, and was fixed at 3° in the latter 55 knees (Fig. 2). Based on our principle, valgus laxity was not permitted, but varus laxity <5° was permitted in both extension and at 90° in the intraoperative assessment. Minimal soft tissue releases were performed, and all peripheral osteophytes were removed. We utilized a spacer-block technique to obtain almost equal balance between the flexion and extension gaps.
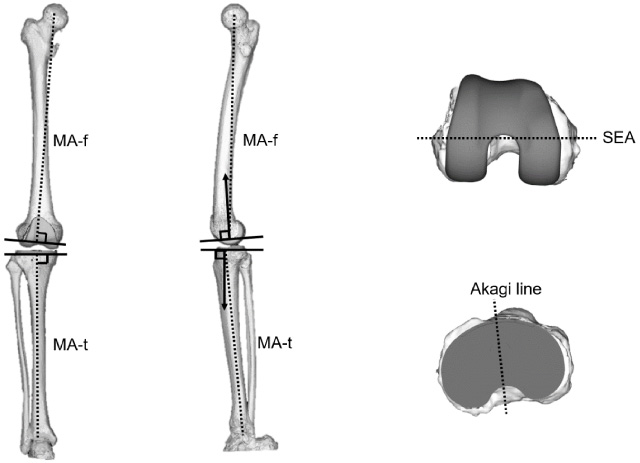
Surgical procedures. In the coronal plane, the distal femur and proximal tibia were resected at 90° to the mechanical axis. In the sagittal plane, the femoral component was sightly flexed by 2–3° to avoid anterior cortical notching. The tibial posterior slope was parallel to the lateral tibial slope in the former 71 knees, and was fixed at 3° in the latter 55 knees. The rotational alignment of the femoral component was parallel to the surgical epicondylar axis, and the rotational position of the tibial component was based on the anteroposterior axis described by Akagi. MA-f (dotted line): the line connecting the midpoint between the centers of the posterior condylar spheres and the center of the femoral head; MA-t (dotted line): the line connecting the midpoints of the eminences of the medial and lateral tibial spines with the center of the ankle joint; solid lines: the cutting surfaces of the distal femur and proximal tibia; arrows: sagittal implant alignment relative to the MA-f and MA-t; SEA: surgical epicondylar axis.
All quantitative parameters were evaluated by a 3D lower extremity alignment assessment system (KneeCAS, LEXI, Inc., Tokyo, Japan), applying a 3D-2D registration technique [9–12] in the biplanar computed radiography images under weight-bearing conditions. First, the 3D digital models of the femur and tibia were reconstructed from CT (Canon Medical Systems, Tochigi, Japan), and visualization and modeling software (Zedview; LEXI, Tokyo, Japan). The tibial and femoral anatomic coordinate and component coordinate systems were established according to the method prescribed by Sato et al. [11,12] (Fig. 3).
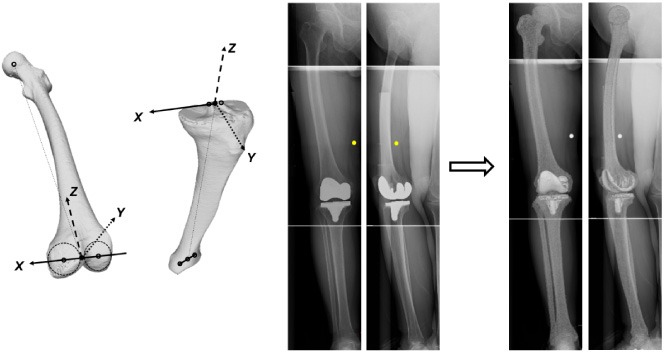
Three-dimensional (3D) to two-dimensional (2D) image registration technique on biplanar X-ray images of the entire lower extremity. The 3D digital models of the femur and tibia and the anatomic coordinate system. The 3D models were projected onto the biplanar computed radiography images obtained under weight-bearing conditions.
Biplanar computed radiography images of each subject’s lower extremity were obtained under weight-bearing conditions: standing with the knees fully extended and the toes in the neutral position. Using the camera calibration technique, the 3D digital bone models were then projected onto the biplanar computed radiography images by matching the silhouettes of the digital models to the contours of the respective computed radiography images via 3D rotations and translations (Fig. 3). Subsequently, all alignments, deformities, and component positions were automatically calculated. Using this method, lower extremity alignment and tibiofemoral position under weight-bearing and component positions and change of condylar offset were investigated. The accuracy of this 3D to 2D image-matching procedure has been previously reported with mean spatial errors of 0.5 mm in distance and 0.7° in rotation [10].
The evaluation parameters were (1) pre- and postoperative 3D hip-knee-ankle (3DHKA) alignment in the coronal plane (Cor HKA); (2) pre- and postoperative 3DHKA alignment in the sagittal plane (Sag HKA); (3) pre- and postoperative femorotibial (F-T) rotational alignment; (4) pre- and postoperative A-P position; (5) postoperative angle of the component position relative to the bone in each plane, consisting of the coronal (varus-valgus), sagittal (flexion-extension), and axial planes (internal–external rotation); and (6) changes in the medial posterior condylar offset (MPCO) and lateral posterior condylar offset (LPCO); and (7) thickness of the insert.
The evaluation parameters in 3D space, including Cor HKA, Sag HKA, and F-T rotation were defined as described in Fig. 4 [19–21]. The Cor HKA and Sag HKA were defined as the angles between the 3D mechanical axis of the femur and tibia projected onto the xz and yz planes of the femoral coordinate system, respectively. In the coronal plane, a larger value indicates varus alignment. In the sagittal plane, a larger value means more knee extension. The F-T rotation was defined as the angle between the surgical epicondylar axis and the tibial anteroposterior axis (Akagi’s line) [16] projected onto the xy plane of the femoral coordinate system. A larger value indicates internal rotation of the tibia relative to the femur [19–21].
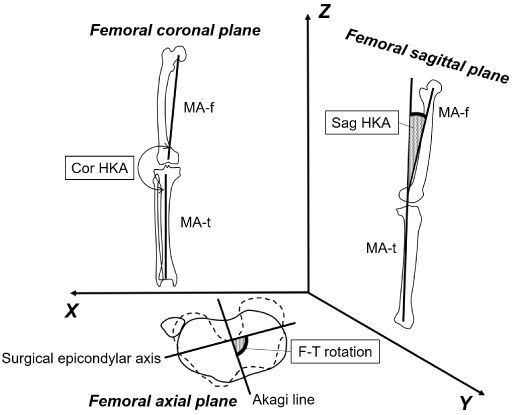
Femorotibial alignment in three-dimensional (3D) space. Preoperative and postoperative 3D hip-knee-ankle (HKA) alignment in the coronal plane (Cor HKA) and sagittal plane (Sag HKA) and femorotibial rotational alignment in the axial plane in the 3D space. MA-f: the line connecting the midpoint between the centers of the posterior condylar spheres and the center of the femoral head; MA-t: the line connecting the midpoints of the eminences of the medial and lateral tibial spines with the center of the ankle joint; Cor HKA and Sag HKA: the angles between the MA-f and the MA-t projected onto the xz and yz planes of the femoral coordinate systems, respectively; F-T rotation: the angle between the surgical epicondylar axis (SEA) and tibial anteroposterior axis (Akagi line) projected onto the xy plane of the femoral coordinate system.
The A-P position was defined as the y-value of the femoral origin evaluated in the tibial coordinate system, and it was standardized by the distance between the surgical epicondylar axis and the preoperative most posterior point of the posterior femoral condyle in the sagittal plane of the tibial coordinate system. A smaller value indicated a posterior position of the femur relative to the tibia (Fig. 5). To evaluate the changes in MPCO and LPCO, the joint lines after surgery were assessed from the spatial location of reference points on the 3D digital model complex according to the method of Sato et al. [12]. The change in the posterior femoral joint line was quantified by subtracting the femoral coordinates along the y-axis of the medial and lateral preoperative posterior joint lines, from the respective femoral coordinates along the y-axis of the medial and lateral postoperative posterior joint lines [12] (Fig. 6). A positive value meant a decrease in PCO from pre- to post-implantation. The component positions relative to the bones, in the spatial relationship between the anatomic and the component coordinate systems, were automatically calculated [9,11,21]. The axes of the femoral and tibial component coordinate systems were projected onto the planes of the respective coordinate systems. The component positions included the varus-valgus angulation, the flexion-extension angulation, and the internal–external rotation (Fig. 7).
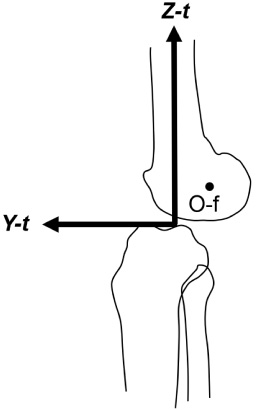
Anteroposterior position of femur relative to the tibia (A-P position). Anteroposterior position of the femur relative to the tibia based on the y-value of the origin of the femoral coordinate system (O-f) in the tibial coordinate system. Y-t and Z-t: y-axis and z-axis of the tibial coordinate system, respectively.
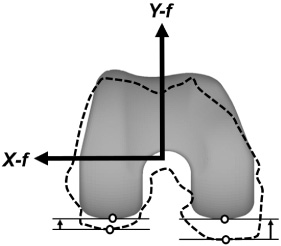
Changes in the medial and lateral posterior femoral condylar offset. The preoperative and postoperative differences in the femoral coordinates along the y-axis of the posterior joint lines. X-f and Y-f: x-axis and y-axis of the femoral coordinate system, respectively.

Definition of component positions relative to the bones. (a) Varus-valgus angulation: the angle between the 3D mechanical axis of the femur (MA-f) or the 3D mechanical axis of the tibia (MA-t) and the z-axis of the component coordinate system (Zc), projected onto the femoral or tibial xz plane, respectively (valgus: +). (b) Flexion-extension angulation: the angle between the MA-f or MA-t and the Zc, projected onto the femoral or tibial yz plane, respectively (extension: +). (c) Internal–external rotation of the femoral component: the angle in the x-axis of the component coordinate system (Xc) relative to a surgical epicondylar axis (SEA), projected onto the femoral xy plane (external rotation: +); Internal–external rotation of the tibial component: the angle in the y-axis of the component coordinate system (Yc) relative to the Akagi line, projected onto the tibial xy plane (external rotation: +).
The Forgotten Joint Score [22] was used as a postoperative patient-reported outcome measure at the last follow-up (minimum 1 year).
Normality of the data was examined by using the Shapiro-Wilk test. The differences in these parameters between the groups were statistically examined, using a two-sample t-test when the data had a normal distribution, or Mann-Whitney U test when the data did not have a normal distribution. For the univariate analysis, correlations between the selected parameters and other variables were analyzed by the Pearson’s product moment correlation coefficient when the data had a normal distribution, or Spearman’s rank correlation coefficient when the data did not have a normal distribution. The statistically significant parameters with a correlation coefficient over 0.2 were extracted. Subsequently, the multiple linear regression analysis was performed. The dependent variable was the postoperative A-P position, and the independent variables were the factors selected in former analysis. Additionally, for each insert, correlations between the postoperative A-P position and other variables were investigated, and multiple linear regression analysis was performed. In all tests, the level of statistical significance was set at a p value <0.05. Statistical analyses were performed using SPSS, version 26 (SPSS, Inc., Chicago, IL, USA).
Results
There were significant correlations between the postoperative A-P position and (1) the preoperative Sag HKA (correlation coefficient [CC] = −0.245, p = 0.006] (2) preoperative A-P position (CC = 0.263, p = 0.003), (3) tibial sagittal component angle (CC = 0.314, p < 0.001), (4) MPCO change (CC = −0.243, p = 0.006), and (5) LPCO change (CC = −0.211, p = 0.018) (Table 2).
Alignment data and correlations between the postoperative femorotibial anteroposterior position and other variables
Alignment data and correlations between the postoperative femorotibial anteroposterior position and other variables
HKA, hip-knee-ankle angle; Cor HKA, hip-knee-ankle angle in the coronal plane; Sag HKA, hip-knee-ankle angle in the sagittal plane; F-T rotation, femorotibial rotation; A-P position, standardized femorotibial anteroposterior position; MPCO, medial posterior condylar offset; LPCO, lateral posterior condylar offset. ∗ p < 0.05.
Among the significant factors in the correlation analysis, the surgically controllable factors – the tibial sagittal component angle, MPCO change, and LPCO change were determined. Multiple linear regression analysis with the dependent variable of the A-P position (R 2 = 0.232, p < 0.001) showed an association with the independent variables of the tibial sagittal component angle (𝛽 = 0.420, p < 0.001) and the MPCO change (𝛽 = −0.301, p < 0.001) (Table 3).
Multiple linear regression analysis with stepwise procedure using each dependent variable of the postoperative femorotibial anteroposterior position
VIF, variance inflation factor; MPCO, medial posterior condylar offset. ∗ p < 0.05.
Concerning the comparison of insert types (Table 4), in the group of CR inserts, (1) the preoperative A-P position (CC = 0.417, p < 0.001), (2) tibial sagittal component angle (CC = 0.247, p = 0.039), (3) MPCO change (CC = −0.294, p = 0.013), and (4) LPCO change (CC = −0.286, p = 0.016) significantly correlated with the postoperative A-P position. In the group of CS inserts, (1) the preoperative Sag HKA (CC = −0.337, p = 0.011) (2) tibial sagittal component angle (CC = 0.303, p = 0.023) significantly correlated with the postoperative A-P position.
Alignment data and correlations between the postoperative A-P position and other variables by each insert
HKA, hip-knee-ankle angle; Cor HKA, hip-knee-ankle angle in the coronal plane; Sag HKA, hip-knee-ankle angle in the sagittal plane; F-T rotation, femorotibial rotation; A-P position, standardized femorotibial anteroposterior position; MPCO, medial posterior condylar offset; LPCO, lateral posterior condylar offset; PCO, posterior condylar offset; CR, cruciate-retaining; CS, cruciate-sustaining; SD, standard deviation. ∗ p < 0.05.
In multiple linear regression analysis with the dependent variable of the postoperative A-P position in the group of CR inserts (R 2 = 0.368, p < 0.001), the independent variables of the tibial sagittal component angle (𝛽 = 0.450, p < 0.001), MPCO change (𝛽 = −0.270, p = 0.021), and LPCO change (𝛽 = −0.253, p = 0.031) showed a significant association, whereas only the tibial sagittal component angle (𝛽 = 0.348, p = 0.009) showed a significant association in the group of CS inserts (R 2 = 0.121, p < 0.001) (Table 5).
Multiple linear regression analysis with stepwise procedure using each dependent variable of the postoperative femorotibial anteroposterior position by each insert
CR, cruciate-retaining; CS, cruciate-sustaining; VIF, variance inflation factor; MPCO, medial posterior condylar offset; LPCO, lateral posterior condylar offset. ∗ p < 0.05.
The most important findings of this study, with respect to the medial pivot prosthesis, were that (1) the increased tibial sagittal component angle, i.e., the posterior tibial slope (PTS) and the decreased MPCO, as the surgical controllable factors, were the dominant factors for the postoperative A-P position, and (2) both the increased PTS and decreased posterior condylar offset (PCO) significantly correlated with the postoperative A-P position in CR inserts, while only increased PTS was correlated in CS inserts.
The increased PTS correlated with the postoperative A-P position in both CR and CS inserts. Though several reports have noted that the PTS <7° was the target as the specific appropriate angle for PTS in other implants [23,24], there were few reports in the medial pivot prosthesis. It has been reported that the CR type in the medial pivot prosthesis is located posteriorly depending on the steep PTS angle, and that the medial femoral condyles of those with a PTS >8° were positioned more posteriorly in the early flexion phase than those with a PTS <7° [6]. Regarding the CS insert, in theory, it can suppress the posterior position. However, this study revealed a correlation between the postoperative A-P position and the PTS in CS inserts, suggesting that the conformity of the CS insert alone cannot negate the influence of the steep inclination of the PTS. It is, therefore, suggested that the excessive PTS should be avoided, regardless of the insert type.
The decreased PCO significantly correlated with the postoperative A-P position in CR inserts but not in CS inserts. It has been reported that a decreased PCO indicates a loosened posterior capsule [25]. A change of PCO >2 mm (which causes a loose posterior capsule and leads to joint laxity) is associated with mid-flexion instability [25]. Anteroposterior stability in full conformity inserts was guaranteed by their conforming geometric articulation in association with a correct soft-tissue tension [26]. Because of its design, the CS insert may accommodate the postoperative A-P position by compensating for the looseness of the posterior capsule due to the decreased PCO, especially under weight-bearing conditions. In contrast, as the CR insert may not have the potential to compensate for the looseness of the posterior capsule, surgeons need to be careful not to decrease the PCO.
Although the factors affecting the postoperative A-P position differed by each insert, the present study exhibited, on average, no significant difference in the postoperative A-P position between the two inserts. The CS insert may be superior to the CR insert in terms of compensation for the decreased PCO, but high posterior lips of the CS insert alone could not completely control the postoperative A-P position. The A-P position is assumed to be caused by the complex relationship among the multi-factors.
This study comprised a group of patients without any evident errors of surgical techniques or problems that could be detected by common assessment modalities. In other words, before this study, the authors thought that their TKAs were successful. However, strict and meticulous measurements to detect deviations of mechanical factors could identify subtle differences. Even for TKAs as considered acceptable by the surgeons, this study revealed that the increased PTS and decreased MPCO were, in particular, the related factors for the postoperative A-P position. This will address those potential problems that cannot be detected by ordinary assessment procedures; and possibly improve the overall outcomes after TKA. The clinical relevance of these results is that surgeons may need to pay greater attention to the excessively increased PTS and decreased PCO to achieve an acceptable postoperative A-P position.
There were some limitations of this study. First, only female patients were investigated, and the differences of muscle strength, activity, and other factors between sexes should be considered. Therefore, the results may not necessarily be applicable to men. Second, the influence of the absence of the PCL should be also investigated. It is necessary to perform a comparative study of the presence of the PCL in a group with the same insert. Third, no analysis of dynamic knee motion was performed. The association between knee instability and femoral posterior position was assumed to be related to knee kinematics; therefore, motion analysis should be performed. Finally, a cut-off value of the PTS or MPCO was desired before the study, but could not be calculated because of the relatively small sample size. This will be addressed in future studies.
Conclusions
The increased PTS and decreased PCO were the dominant factors for the postoperative femoral anteroposterior position relative to the tibia under weight-bearing conditions. The increased PTS and decreased PCO correlated with the postoperative A-P position in CR inserts while only the increased PTS was correlated in CS inserts.
Footnotes
Acknowledgements
The authors would like to thank all staff members of the Department of Rehabilitation, Niigata Medical Center, Dr. Yamanaka K., Dr. Omori G., and Dr. Koga Y.
Conflict of interest
None of the contributing authors have any conflict of interest to declare.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.