
Abstract
BACKGROUND:
Bone defects arising from diverse causes, such as traffic accidents, contemporary weapon usage, and bone-related disorders, present significant challenges in clinical treatment. Prolonged treatment cycles for bone defects can result in complications, impacting patients’ overall quality of life. Efficient and timely repair of bone defects is thus a critical concern in clinical practice.
OBJECTIVE:
This study aims to assess the scientific progress and achievements of magnesium phosphate bone cement (MPC) as an artificial bone substitute material. Additionally, the research seeks to explore the future development path and clinical potential of MPC bone cement in addressing challenges associated with bone defects.
METHODS:
The study comprehensively reviews MPC’s performance, encompassing e.g. mechanical properties, biocompatibility, porosity, adhesion and injectability. Various modifiers are also considered to broaden MPC’s applications in bone tissue engineering, emphasizing drug-loading performance and antibacterial capabilities, which meet clinical diversification requirements.
RESULTS:
In comparison to alternatives such as autogenous bone transplantation, allograft, polymethyl methacrylate (PMMA), and calcium phosphate cement (CPC), MPC emerges as a promising solution for bone defects. It addresses limitations associated with these alternatives, such as immunological rejection and long-term harm to patients. MPC can control heat release during the curing process, exhibits superior mechanical strength, and has the capacity to stimulate new bone growth.
CONCLUSION:
MPC stands out as an artificial bone substitute with appropriate mechanical strength, rapid degradation, non-toxicity, and good biocompatibility, facilitating bone repair and regeneration. Modification agents can enhance its clinical versatility. Future research should delve into its mechanical properties and formulations, expanding clinical applications to create higher-performing and more medically valuable alternatives in bone defect repair.
Introduction
Injuries from severe trauma, car accidents, falls, bone tumor removal, and other diseases of the bone tissue frequently result in bone defects, which have a significant negative impact on patients’ quality of life, and place a significant cost on families, and society [1]. The bone defect has a high incidence, a protracted disease course, a challenging operation, a protracted course of therapy, and several complications [2]. Clinicians struggle greatly with how to expeditiously and efficiently encourage the healing of bone defects while also coordinating this process with the body’s own repair [3]. The source of autogenous bone is limited [4], and the acquisition process will result in secondary injury, which will increase the physical burden and financial burden on patients [5]. However, studies currently available indicate that autogenous bone is a perfect material for repairing bone defects and immune rejection will not occur [6,7]. Allogeneic bone transplantation can help to some extent with the issue of limited autogenous bone sources [8], but it carries the risk of rejection and disease transmission [9,10]. Artificial bone substitute materials have clear benefits over the first two, including abundant supplies, low cost, ease of production, and no further injury to the body [11,12].
Polymethyl methacrylate (PMMA) [13,14], which is utilized primarily in polymethyl methacrylate bone cement, is now the most often used bioactive bone repair material in clinical practice. While polymethyl methacrylate bone cement has some mechanical strength, a quick setting time, and other benefits [15], it also has a number of drawbacks, including the fact that its curing will release a lot of heat and harm nearby tissues, that its monomer is cytotoxic, and that PMMA bone cement is difficult to degrade [16–18]. To better biocompatibility and degradation performance, researchers created calcium phosphate bone cement (CPC), whose primary component is similar to natural bone inorganic and won’t harm surrounding tissues, to improve biocompatibility and degradation performance. CPC has excellent biocompatibility and degradability [19–26].
However, the inability of CPC to promote neurogenesis and its limited mechanical strength makes it difficult to replenish lost neurogenesis at the defect site [27,28]. To solve the existing problems in the CPC system, researchers created the derived magnesium phosphate bone cement (MPC) to address issues that were already present in the CPC system [29–34]. MPC has an adequate compressive strength in the early stage of hydration reaction [32–36], and a fast intraoperative setting rate [29,37]. Since magnesium phosphate is its main product, MPC has good biocompatibility and can be biodegraded in the internal environment [38–42]. Additionally, the compound MPC created by combining MPC with modified substances can meet the needs of clinical diversification [43–47]. This has helped the study on MPC for bone defect healing become steadily more well-known [48].
The purpose of the current study is to examine the scientific progress and accomplishments of MPC up to this point and analyze the future development direction and clinical prospects of MPC bone cement in order to help the majority of academics better comprehend this material.
Composition of MPC
As can be seen in Fig. 1, MPC typically consists of a liquid phase that contains phosphate and a solid phase that contains magnesium. An acid-base and hydration interaction of several components led to the creation of magnesium phosphate cement [49]. Han et al. [50] employed borax (Na2B4O7 ⋅10H2O) as a retarder, distilled water as the curing solution, potassium dihydrogen phosphate (KH2PO4) as the acidic component, and magnesium oxide (MgO) as the alkaline component. Additionally, to create potassium hydrogen phosphate bone cement (MKPC), a tiny quantity of hydroxyapatite (HA) was mixed with the cement. To create MPC, Gelli et al. [51] employed TMP(Mg3(PO4)2) as an alkaline component and DAHP((NH4)2HPO4) as an acidic component. At the same time, Sopcak, [52], and colleagues created a wollastonite/newberyite cement by combining crystalline -wollastonite (CaSiO3) with newberyite (MgHPO4 ⋅3H2O) powder and then adding MNaHP (NaH2PO4) solution. Although MPC incorporating ammonium salt also showed high biocompatibility and non-toxicity in the trial, the harm to the human body cannot be foreseen because ammonia gas will be produced during the production procedure [40]. Therefore, non-toxic processes, such as KH2PO4+MgO, should be selected as much as feasible when choosing the raw ingredients for MPC manufacturing.

Composition of magnesium phosphate bone cement.
Researchers examined the benefits of MPC bone cement as a bone defect repair material and evaluated its performance in a number of areas as shown in Fig. 2, including mechanical properties, biocompatibility, setting time, porosity, injectability, degradation and promoting growth. Table 1 shows the MPC formulation developed by some researchers in recent years, as well as the mechanical strength, setting time and porosity of cement.
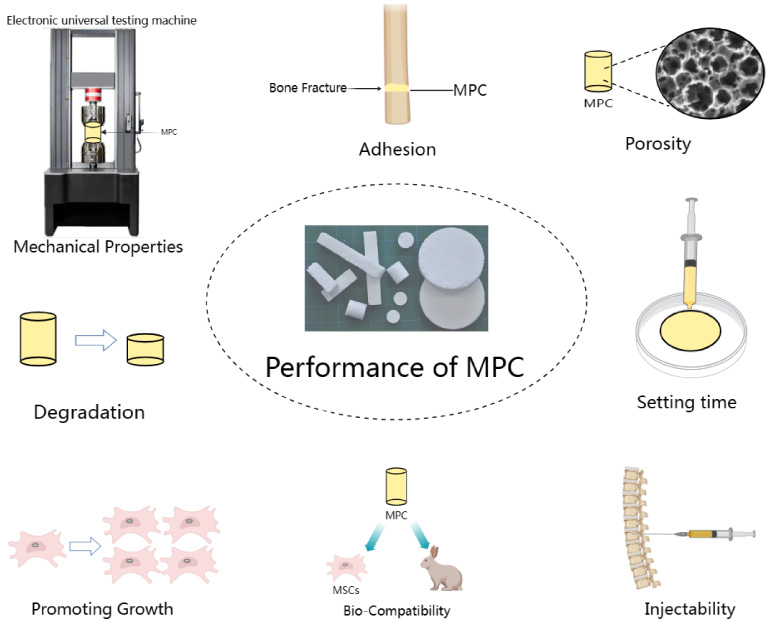
Performance of MPC.
MPC formulation, mechanical strength, setting time and porosity
Abbreviation: t 1 Initial setting time, t 2 Final setting time, TMP Mg3(PO4)2, O-CMC O-Carboxymethyl chitosan, DAHP (NH4)2HPO4, IP6 phytic acid, HA Hydroxyapatite, TTCP Ca4(PO4)2O, HPMC hydroxypropyl methylcellulose, CMC carboxymethyl chitosan, SA sodium alginate.
Mature bone is made up of two different types of tissue, one of which is cortical bone, which is relatively dense and has a mechanical strength of 133–193 MPa, and the other which is trabecular or cancellous bone, which is made up of a network of pillars or trabecular interconnected or cancellous bone and has a mechanical strength of 3.6–9.3 MPa [53]. Appropriate strength is a crucial need for bone cement to be extensively produced and utilized in the clinic as a benchmark to test the loading capacity of MPCs after implantation [54,55]. The compressive strength of magnesium phosphate cement prepared by Gong et al. [39] with magnesium potassium phosphate cement (K-struvite) and oxygen-carboxymethyl chitosan (O-CMC) is 33.8 MPa (P < 0.05); Similar to this, Liu et al. [56] produced TTCP/KMPC, whose maximal mechanical strength may reach 69 ± 2.4 MPa, using TTCP, MgO, KH2PO4, Na2B4O7, and other minerals. He et al. [57] combined magnesium calcium phosphate and sodium alginate to manufacture innovative compound cement with high compressive strength (91.1 MPa), indicating that the mechanical strength of MPC is generally within 100 MPa. The repair of non-weight-bearing bone defects in humans is hence the primary use for MPC.
Bio-compatibility
The term “biocompatibility” describes a material’s ability to operate at desired performance when used on a particular area of the host. The so-called “desired performance” should take into account two factors: first, it means that the biological material used in the host does not cause adverse reactions to the organism’s tissues or organs (such as sensitization, mutagenicity, toxicity, hemolysis, irritation, carcinogenicity, or coagulation); second, it means that the host environment has no negative effects on the application material [58].
Bone cement made of magnesium phosphate has high biocompatibility. Degradable potassium MPC created by Bone Solutions Incorporated (BSI) was approved for use in the United States as a filler material for bone defects by the FDA (Food and Drug Administration) in 2009 [59]. This clearly demonstrates its strong biocompatibility. Additionally, utilizing X-ray diffraction analysis, histological staining, radiographic inspection, and EDX measurement to confirm its biocompatibility, Fuchs et al. [60] created a novel bone augmentation material in the form of spherical particles containing magnesium phosphate cement. According to the findings, this brand-new spherical MPC has high biocompatibility, doesnt cause any inflammation, and properly engages connective tissue in bone mending. Furthermore, it fully regenerates bone and demonstrates fast and prolonged deterioration. Moreover, an MC3T3-E1 cell culture experiment was also carried out by Wang et al. [32] to assess the cytocompatibility and bone inducibility of their citric acid-containing MPC using cell proliferation and morphology, alkaline phosphatase, alizarin red staining, and western blotting. According to the tensile morphology and MTT findings of the cells, none of the experimental group materials clearly exhibited cytotoxicity toward the cells or had a negative impact on cell survival or proliferation. All samples passed cytocompatibility tests with flying colors. Additionally, cells develop on biomaterial, demonstrating both the material’s biocompatibility and the survival of the cells after adhering to it.
It is clear that MPC has high biocompatibility and won't have any negative effects on the body, which paves the way for encouraging the formation and regeneration of bone tissue.
Setting time
One of the crucial aspects to take into account while designing is the bone cement’s setting time [61]. In order for clinicians to mix bone cement and create material patterns that satisfy various therapeutic objectives, the setting time of bone cement should be within an appropriate time limit [62]. A short setting time cannot allow clinicians enough time for manufacture and administration, while a long setting time might cause a significant inflammatory response [63].
The adaptability of the setting time of MPC is one of its advantages [40]. By e.g. adding material, changing the solid-to-liquid ratio and material size, the setting time may be changed. For instance, Esnaashary et al. [64] altered the powder-liquid ratio (PLR), raw material particle diameter, and calcination temperature of Mg3(PO4)2+Mg21Ca4Na4(PO4)18 to alter the setting time of cement. The setting time window, according to their modification, is 2 to 22 minutes, with the setting time at 22 MPa being 9 minutes with the proper mechanical strength. Meanwhile, Gelli et al. [51] used Tri-magnesium phosphate powder and a solution of di-ammonium to make MPC with hydrogen phosphate, struvite as the final product. As the powder-to-liquid ratio (P/LR) and DAHP concentration changed, they found that t 1 and t 2 decreased with the increase of the P/L ratio at a given DAHP concentration, while a higher DAHP concentration reduced the setting time at a given P/L ratio. Additionally, Klammert et al. [65] performed remarkable studies in which they examined the correlation between the time required for grinding and the time required for setting the precursor material for cement (Mg2.25Ca0.75(PO4)2). As the grinding time (min) increases [–, 30, 60, 90, 120, 150], its setting time (min) decreases [60, 32, 11, 10, 9, 8].
MPC’s application value is considerably increased by its ability to modify its setting time and associated qualities with the addition of changed materials and component content adjustments.
Porosity
The design of cement must take into account porosity. Too little porosity prevents bone cement from exerting its full biological potential, whereas too much porosity results in insufficient mechanical strength. Appropriate porosity can encourage the growth and development of bone defects and contribute to the antibacterial and drug-loading properties of bone cement [66].
The porosity of MPC has been the subject of several investigations by researchers. For instance, when Gelli et al. [51] tested the porosity of MPC with TMP+DAHP, they discovered that the porosity reduced as the P/L ratio increased at a certain DAHP concentration. The sample with a moderate concentration of DAHP had the greatest porosity at a constant P/L ratio. As a result, the P/L ratio and solution concentration have an impact on MPC’s porosity. Meanwhile, Schaufler et al. [67] created microporous calcium magnesium phosphate cement using 3D powder printing technology, which gave CMP the greatest fit and high porosity to accelerate bone development. They produce CMP with a porosity of 13–28%, and in an experiment using the human fetal osteoblast cell line hFOB 1.19, the CMP group demonstrated the best cell proliferation results. Additionally, Mestres et al. [59] discovered that the porosity of bone cement is larger than 5 um, which can have a stronger antibacterial impact in an experiment on the antibacterial effect of bone cement on osteomyelitis. This study further demonstrates that MPC bone cement has inherent antibacterial characteristics and that these qualities are comparable to those of large-porosity bone cement which contains doxycycline hypochlorite (CPFd).
Appropriate porosity is therefore crucial in the design of MPC since it can help to promote bone development and give bone cement antibacterial and drug-loading capabilities.
Adhesion
The fixing of shattered bones in comminuted fractures is a challenging issue that doctors must deal with. Steel plates and screws may not always be effective fixing tools [68]. In clinics, PMMA bone cement is frequently used as the adhesive between the prosthesis and bone interface. However, PMMA is not an ideal bone-bone interface adhesive material due to its poor biocompatibility and biodegradability, and its excessive exotherm will cause bone necrosis and surrounding tissue damage [69].
MPC is thought to be a possible bone-bone interface adhesive after the adhesion of MPC bone cement has been researched in recent years. For instance, Yu et al. [38] observed that compound MPC may increase osteoblast adhesion and attachment, stimulate bone differentiation, and accelerate bone growth and development. They did this by combining carboxymethyl chitosan-sodium alginate (CMCS/SA) with MPC. Meanwhile, MPBC (MgO, KH2PO4, Ca (H2PO4)2⋅H2O and Citric Acid) created by Yu et al. [40] has greater adhesion because it has lower phosphate solubility and weaker alkalinity than MPC. Likewise the experimental study by Brückner et al. [70] discovered that a compound MPC with 25% IP6 and a powder-liquid ratio (PLR) of 2.0 g/mL could still maintain a shear strength of 0.81 ± 0.12 Mpa between bone and bone after being submerged in water solution for 7 days, fully demonstrating the potential of MPC bone cement as a bone adhesive. Furthermore, MPC, a kind of bone glue created by Sehlke et al. [71], received FDA approval for therapeutic use in 2009 and shown excellent mending outcomes in both animal studies and human clinical trials.
In conclusion, MPC bone cement can function well as an adhesive in the healing of fractures.
Injectability
One of the key factors that need to be taken into consideration in design is the injectability of bone cement. In an attempt to enhance the strength and stability of the vertebral body, hinder collapse, alleviate low back pain, and even partially restore the height of the vertebral body, percutaneous vertebroplasty (PVP) uses a percutaneous puncture to inject bone cement through the pedicle or directly into the vertebral body. Cement viscosity and setting time have a direct relationship with injectability. The injectability of cement will be worse if the setting time is shorter and the viscosity is higher, which will prevent surgeons from having enough time to perform surgery [72].
Bone cement made of magnesium phosphate has a significant benefit in terms of injectability control. According to Yu et al. [73], the MPC’s 30-second setting time is insufficient for surgeons to carry out injection procedures. They gave MPC CMC (carboxymethyl chitosan), which made it wet and sticky and increased the amount of time it took for MPC to set. The setting time of MPC is extended and its injectability is enhanced by the addition of CMC to cement. Similar to this, Li et al. [61] prolonged the setting time of MPC by adding borosilicate bioglass (BG) to improve the injectability of cement. Their findings reveal that BG-doped MPC has great injectability and an appropriate setting time, and that it can be utilized to fill 3D models after printing to construct bone cement shapes that can fit a variety of therapeutic applications.
Therefore, by varying the cement’s setting time and adding modifying agents, MPC can adjust the cement’s injectability. Such adaptable MPC demonstrates its broad applicability in the medical industry.
Degradation and promoting growth performance
The degradation of bone cement in vivo is essential [74]. On the one hand, it will not have side effects on the body, on the other hand, it can also give space for bone and surrounding tissues to grow. Magnesium phosphate cement has an excellent performance in degradation degree, and its degradation can accelerate the growth of bone and surrounding tissues. In Kaiser et al.’s [75] experiment, K-struvite (MgKPO4⋅6H2O) bone cement was continuously degraded and new bone tissue was formed at the same time. Four months later, 63% of the K-struvite (MgKPO4⋅6H2O) had been degraded. This degradation rate is faster than calcium carbonate cement, and the rate of bone regeneration by MPC is also stronger than that of CPC [76]. At the same time, Wu et al.’s [77] experiment also proved the same result. Compared with CPC, the new calcium magnesium phosphate cement (CMPC) showed significantly improved degradability in simulated body fluids, and its biocompatibility was higher than CPC’s, which could support cell adhesion and proliferation and accelerate the formation of new bones.
In conclusion, magnesium phosphate cement has the advantages of a fast degradation rate and fast bone formation efficiency, which well supports its clinical application.
Modification
Due to its modification, MPC will change in features, enabling it to satisfy the demands of clinical diversification. In the past five years of research on MPC, scientists have made adjustments to the MPC by e.g. enhancing its mechanical properties, producing antibacterial capacity, increasing antimicrobial capacity, increasing drug load, improving injectability and enhancing biocompatibility, so that compound MPC can produce more potent and extensive effects, allowing it to be used and served by the clinic more effectively.
Stronger mechanical properties
Better mechanical properties translate into better bearing capacity, which can support the weight of bones without cracking or breaking because to insufficient bearing capacity. In terms of bettering mechanical qualities, Yu et al. [73] added CMC (carboxymethyl chitosan) to MPC to increase mechanical strength to 55.7 MPa. Additionally, the mechanical strength of CS-MPCs (bioactive chondroitin sulfate (CS)-MPC) produced by Shi et al. [78] are able to attain 29.67 ± 1.45 MPa. Furthermore, Gao et al. [38] displayed that the polymeric carboxymethyl chitosan-sodium alginate (CMCS/SA)+MPC may achieve a mechanical properties as high as 59.43 ± 8.31 MPa.
Although modified compound MPC now has a mechanical strength that is higher than MPC, it is still challenging to reach the load-bearing bone’s necessary strength. If the mechanical properties are excessively pursued at the expense of porosity, the bone repair and antibacterial properties of the material will be reduced, which will not be worth the loss [39].
In order to increase MPC’s load-bearing capacity without sacrificing other characteristics of the material, researchers are continuously looking into novel ways to improve its mechanical properties.
More appropriate setting time
Compound MPC makes the setting time of bone cement more suitable for the clinic. One of MPC’s greatest benefits is the ability to manage the setting time, which can be altered by modifying the raw material’s particle size, surface area, MgO percentage, and P/L ratio [72]. Additionally, researchers typically add modified substances to materials to change the setting time because doing so has a greater cost-benefit ratio and can improve other attributes without altering the material itself. For instance, research by Lv et al. [37] demonstrated that the MPC + Ca(H2PO4)2 + CMC setting time window is 8–25 min, matching the set period of standard surgical bone cement implantation of 8–20 min [61]. Additionally, ZnO-NPs were employed by Wang et al. [79] to improve the functionality of MPC, and the results revealed that MPC's setting time could be increased from 8.2 min to 25.3 min. Its retarding impact becomes increasingly apparent as ZnO-NPs content rises.
As a result, the compound form of magnesium phosphate cement allows for better control and flexibility over the cement’s setting time, allowing it to be widely employed in clinics to accomplish intended objectives under various surgical circumstances.
Better biocompatibility
By incorporating compound materials, MPC can increase its biocompatibility and lessen adverse body reactions as well as the body’s host anti-graft reaction.
For example, Ewald et al. [80] demonstrated the material’s enhanced biocompatibility via the use of oil-based calcium-doped magnesium phosphate (CaMgP). They implanted CaMgP into the distal femoral condyle drilling defect of New Zealand white rabbits, watched the body’s response after 6 and 12 weeks, and discovered that no soft connective tissue or inflammation symptoms developed. Similar to this, MPC compound bone cement exhibited superior biocompatibility, according to Gelli et al. [81]. In their experiment, citrate was incorporated into MPC, and the experiment demonstrated that it could be released from cement while also helping to alkalize the immediate environment. This demonstrated its significance in the cytotoxicity experiment with human fibroblasts and improved the biocompatibility of bone cement. Additionally, Liu et al. [82] developed a strontium-containing MPC, which will significantly enhance the biocompatibility of the bone cement and provide a favorable environment for cell development, calcium mineralization, and the formation of new bone.
Therefore, an obvious conclusion can be drawn from the aforementioned examples that MPC bone cement with modified substances has greater biocompatibility.
Drug loading performance and antibacterial performance
MPC’s antibacterial and drug-loading characteristics have recently attracted a lot of study attention. By incorporating modified substances, MPC bone cement can achieve drug-loading and antibacterial performance, considerably enhancing its medical value and enabling it to predict a wide range of future applications.
Drug loading performance
In terms of drug loading performance, Zhao et al. [83] created a drug carrier system and compounded it into calcium magnesium phosphate cement (MCPC). The cement contains gelatin coated hollow mesoporous silica nanoparticles (HMSNs/GM), which are loaded with promoting bone parathyroid glands (PTH) and anti-osteoclast alendronate (ALN). In addition to the role of MCPC itself, its drug loading system can also accelerate angiogenesis, promote osteogenic differentiation and mineralization, inhibit bone fragmentation and bone resorption, and enhance bone regeneration in ovariectomized osteoporosis rats.
Antibacterial performance
In terms of antimicrobial properties, Roller et al. [84] created antibiotic-loaded cement (MPC-vans) beads by mixing 5 ccs of MPC for 2 min, adding 1 g of vancomycin hydrochloride (Millipore Sigma, St. Louis, MO), mixing another 30 s, and spreading the putty mixture over a bead mat (Bone Solutions, Inc., Colleyville, TX). Compared to the control group, MPC-vans produced an inhibitory zone against Staphylococcus aureus, demonstrating its antibacterial properties. Meanwhile, the resazurin assay demonstrated that there were no significant differences between the fluorescence levels associated with cellular metabolism between the MPC-vac group and the MPC control group.
From the above examples, it can be proven that MPCs with drug loading and antibacterial properties are effective. The developed MPCs with drug loading and antibacterial properties can exert local anti-infection and treatment effects in the body, which has important positive significance for patient rehabilitation and infection prevention. If similar local anti-infection and local treatment effects can be produced in future Human subject research, then compound MPC will probably become a hot spot of continuous attention and research.
In conclusion, compound magnesium phosphate cement offers adjustable and adaptable performance compared to single-component magnesium phosphate cement, which may be recognized by academics and medical professionals. Future research should look more closely at compound MPC due to its wide component selectivity and diversified ratio, which has better medical significance for clinical healthcare.
Prospect of MPC
Bone tissue regeneration and repair can be aided by its appropriate mechanical strength, rapid degradation, non-toxicity, and good biocompatibility of MPC. The proliferation and differentiation of osteoblasts can be stimulated in vitro by MPC, and it has also been effectively demonstrated that bone growth processes at bone defects can be improved in vivo. Additionally, the properties of MPC can be altered by adding various compound materials, giving it better properties such as stronger mechanical strength and more suitable setting time. Additionally, by adding modified substances, the material can acquire unique qualities like antibacterial properties and drug-loading properties. Consequently, MPC is expected to be used as a potential bone repair material.
Despite the various benefits of magnesium phosphate cement, there is always an opportunity for advancement. The application scope of MPC bone cement is now restricted to non-load-bearing bone repair due to its relatively low mechanical strength. Besides, because MPC bone cement can improve the properties of cement by adding various modifying substances and adjusting the content of different components in bone cement, researchers have different research systems for MPC, which makes it slightly difficult to compare the advantages and disadvantages of various MPC bone cement formulas.
In the future development direction, researchers can continue to deepen their investigation into the mechanical characteristics of bone cement, expand the clinical application range of MPC bone cement, and continue to improve the formulation of MPC bone cement. Simultaneously, to be able to create MPC with improved performance and greater medical value in the field of bone defect repair, intensify research on MPC bone cement in various systems should be done, thoroughly understand the benefits and drawbacks of MPC in each formula, and strengthen the connections between various MPC formulas.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
The study was supported by the Special Project for Innovation and Generation of Military Medical Support Capabilities (Grant/Award number: 20QNPY069); the Gansu Provincial Youth Science and Technology Fund Program (Grant/Award number: 20JR5RA593); and the National Natural Science Foundation of China (Grant/Award number: 31800812).