
Abstract
BACKGROUND:
Lumbar lordosis is required for bipedalism.
OBJECTIVES:
To investigate age-related changes in lumbar lordosis and to clarify the relationships between lumbar lordosis and vertebral wedging and disc degeneration.
METHODS:
A total of 300 women were included in this retrospective study, 50 in each of six age groups (20-, 30-, 40-, 50-, 60- and 70-year-olds). Patients with vertebral collapse, instable fracture or disc sequestration were excluded. In each patient, lumbar lordosis angle, posterior vertebral wedging, L5-S1 intervertebral disc angle, L5/L1 vertebral height ratio and L5-S1 intervertebral disc/L1-L2 intervertebral disc height ratio were examined. Significance level was set at
RESULTS:
Significant differences were found in lumbar lordosis according to age group (
CONCLUSION:
In this cohort, strong spinal structure was maintained during physiological aging from 20 to 40 years of age; lumbar lordosis increased by 50 years of age. Increased lordosis correlated with increased posterior vertebral wedging and loss of posterior disc height.
Introduction
Lumbar lordosis is specific to human who stands for his life. Bipedalism is only possible with sagittal balance, the most important component of which is lumbar lordosis [1]. Lumbar lordosis is poorly developed or even totally absent in infants [2]. Development of lordosis increases in conjunction with bipedalism during early childhood [3]. The most frequently encountered problems in sagittal balance involve lumbar lordosis. In their study of different spine types, Roussouly et al. [4] defined harmony between spine and pelvis and described sagittal balance as that spinal alignment requiring the least amount of energy consumption during standing. Lumbar lordosis mainly results from the conformation of the L4-L5 and L5-S1 segments. In the hypolordotic spine, the load on the spine is increased and early degeneration and disc herniation may be seen. The thoracic region bends to the front in patients with lumbar flatness deformity, resulting in sagittal imbalance [4]. In the hyperlordotic spine, the load on the posterior elements is increased, increasing the risk of facet joint hypertrophy and spondylolisthesis [4]. Some previous studies have reported that lumbar lordosis decreases in old age, whereas others have reported that lordosis increases with age [5, 6].
Vertebral height increases towards the coccyx in the vertebral column; however the posterior height of the lumbar vertebrae is shorter than the anterior height, contributing to the development of lumbar lordosis [7]. The height of the anterior vertebrae is especially greater than the posterior height at L5 and L4. Therefore, posterior wedging is seen in the lumbar vertebrae. The prevalence of physiological posterior vertebral wedging increases towards the inferior lumbar region [8]. However, in osteoporotic compression fractures, anterior wedging is often seen [9].
Previous studies have investigated age-related degeneration of the facet joints, discs and end plates [10]; others have described multifidus muscle atrophy associated with aging [11]. Our primary objective in the present study was to clarify the normal aging process by evaluating age-related changes in the lumbar lordosis angle and the prevalence of posterior vertebral wedging. Our secondary purpose was to investigate the comorbidity of increased lumbar lordosis and posterior vertebral wedging and the relationship with disc degeneration.
Methods
Following approval of the ethics committee at our institution, power analysis was performed to determine the number of patients to include in our retrospective study. When alpha error and beta error are both considered as 0.05, a minimum of 23 cases are needed within each group in order to state that there is a statistically significant difference for a common variance of 86 and 10 units of difference between decades, according to pilot studies.
Patient population
A retrospective study of MRIs of 300 female patients, 50from each age group, was done between January 2015 and December 2015. Only patients aged 20, 30, 40, 50, 60, or 70 years were included, to minimize the overlap of parameters during decade transitions.
Exclusion criteria:
Men were excluded to eliminate the effects of gender. According to the Arbeitsgemeinschaftfür Osteosynthesefragen classification [12], patientswith (A.1.1) impaction of endplates and (A.1.2) wedge impaction fracture subgroups were included. However, those with (A.1.3) vertebral body collapse and instable fractures were excluded, because these could affect the lumbar lordosis angle. Patients with transitional vertebrae, sequestrated disc herniation, rotoscoliosis, vertebral or paravertebral mass, spinal mass, and patients with previous spinal operation or infiltrative disease of the bone marrow were excluded.
A 1.5-T MR Unit (Signa HDxt; GE, USA) and body surface coil were used. Sagittal T1-weighted fast spin-echo (FSE), sagittal T2-weighted FSE and axial T2-weighted FSE (3680/128 repetition time/echo time, 180
Visual evaluation
A radiologist with 10 years of experience in evaluating the musculoskeletal system performed all MRI evaluations. All measurements were made on T1- and T2-weighted mid-sagittal plane images. The following parameters were measured:
Lumbar lordosis angle: The angle between the line passing along the superior plateau of L1 on a mid-sagittal section and the line passing along the superior plateau of S1.
Posterior vertebral wedge: L1, L4 and L5 were individually evaluated. Anterior and posterior heights of the vertebrae, including the cortex, were measured. The ratio of anterior height/posterior height was calculated (Fig. 1a).
(a) L5 posterior vertebral wedging: Anterior and posterior vertebral heights were measured including the cortex and their ratio was calculated. (b) L5-S1 intervertebral disc angle (D-Cobb): Angle between the inferior plateau of L5 and superior plateau of S1 was measured. (c) Height ratio of L5/L1 vertebra: Central height of each vertebra was measured and their ratio was calculated.
L5-S1 intervertebral disc angle (D-Cobb): The angle between lines passing along the inferior plateau of L5 and the superior plateau of S1 (Fig. 1b).
Ratio of L5/L1 vertebral height: The average height of both vertebrae was measured and their ratio was calculated (Fig. 1c).
Height ratio of L5-S1 intervertebral disc/L1-L2 intervertebral disc: The average height of both discs was measured and their ratio was calculated.
Normality was determined with Shapiro-Wilk and single sample Kolmogorov-Smirnov tests, histogram, box-plot and Q-Q graphs. Variables without normal distribution were compared with one-way Kruskal-Wallis variance analysis. Post hoc comparisons were performed with Dunn’s test. Data are expressed as mean, standard deviation, median, minimum and maximum. Variability in lumbar lordosis angle according to age category was assessed with one-way variance analysis (one-way ANOVA). Variance homogeneity was evaluated with Levene’s test. Post hoc (multiple) comparisons were performed with Tukey’s HSD test as group variances were homogenous. Correlations between lumbar lordosis angle and other variables were analyzed with Pearson’s correlation for variables with normal distribution and with Spearman’s correlation test for others. Significance level was set at
Results
The lumbar lordosis angle, assessed with one-way variance analysis, ranged from 42.24
Lumbar lordosis angle was analyzed with one-way variance analysis (one-way ANOVA) (SD: standard deviation)
Lumbar lordosis angle was analyzed with one-way variance analysis (one-way ANOVA) (SD: standard deviation)
Significant differences were found in lumbar lordosis angle according to age group (
Differences in lumbar lordosis angle between age groups (
Homogeneous distribution of lumbar lordosis according to age (Tukey’s HSD test
Lumbar lordosis angle (L-Cobb) independent from age variable, L5-S1 disc angle (D-Cobb), L5 vertebral wedging (L5 wedge), L4 vertebral wedging (L4 wedge), L5 vertebra height/L1 vertebra height (L5/L1 vertebra) and L5-S1 disc height /L1-L2 disc height (L5/L1 disc). Mean
Correlations between lumbar lordosis and other variables were assessed with Pearson’s correlation test. Lumbar lordosis correlated most strongly with L4 posterior vertebral wedging (
Spearman’s correlation test revealed no association between lumbar lordosis and L1 wedging (
Mean
The distribution of L1, L4 and L5 vertebral wedging was examined according to age group (Table 5). Post hoc comparisons were performed with the Kruskal–Wallis multiple-comparison z-value test (Table 5). Z-values
Distribution of L5 vertebral wedging and L4 vertebral wedging according to age (Dunn’s test)
There were no differences in the prevalence of L5 vertebral wedging between participants 20 years of age versus those 30 or 40 years of age (z-values 0.94 and 0.43, respectively). At 50 years of age, the prevalence of L5 vertebral wedging was significantly higher than among younger patients (z-value
There were no differences in L4 vertebral wedging prevalence between participants 20 years of age versus those 30 or 40 years of age (z-values 0.49 and 1.23, respectively). At 50 years of age, the prevalence of L4 vertebral wedging was significantly higher than at 20, 30 or 40 years of age (z-value
For L1 vertebral wedging the only significant difference was between participants 70 years of age and those 20, 50 or 60 years of age (z-value
Examples of lumbar lordosis angle measurement on T2-weighted midsagittal MRI are shown for (a) 20-year-old, (b) 30-year-old, (c) 40-year-old, (d) 50-year-old, (e) 60-year-old and (f) 70-year-old.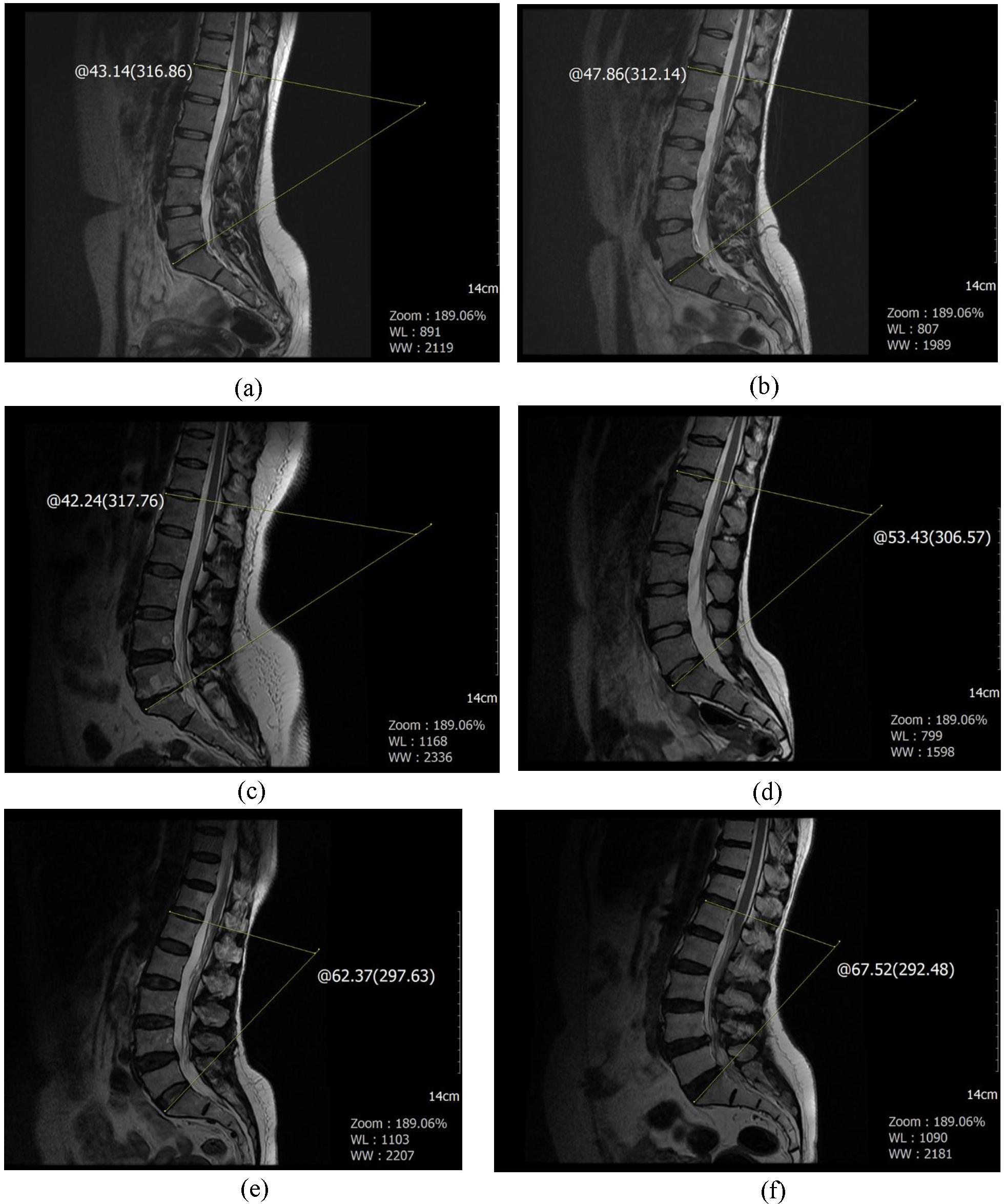
T2-weighted midsagittal MRI: L3-L4 and L4-L5 intervertebral disc sequestrations are seen. Lumbar lordosis is flattened (lordosis angle 31.3
During physiological aging, significant changes of lumbar lordosis were not present in women 20 to 40 years old. Similarly, no significant difference was found in the prevalence of posterior vertebral wedging at L4 or L5 among these age groups. In addition, 40-year-olds in this study had a mean lumbar lordosis angle smaller than those of 20- and 30-year-old. Why do we see changes at 50 years of age despite a young and strong lumbar spine up to 40 years of age? Paravertebral muscles provide spine stabilization; obesity and dehydration leading to loss of disc height increase the load on the lumbar vertebrae and are considered to be important factors in spine aging. In our previous study on atrophy of the multifidus muscle, which is a significant stabilizer of the lower lumbar vertebrae, muscular atrophy began at 40 years of age [11]. The partial loss of stabilization resulting from multifidus muscle atrophy, along with obesity, may increase lordosis. There is a recognized correlation between obesity and increased lordosis [13]. In their study of middle-age and elderly women, Guo et al. [14] detected increased lumbar lordosis in obese individuals. However, obesity was not assessed in the present retrospective study. Fifty years of age was a significant cut-off point for lumbar lordosis and increased posterior vertebral wedging; both of these gradually increased after 50 years of age. L1 wedging was seen at about 70 years of age and was not observed at younger ages. Accordingly, aging in the lumbar spine, which is defined as young at 20 years of age, starts at 50 years of age. Can development of hyperlordosis be prevented by maintaining paravertebral muscle strength and preventing abdominal fat increase?
Sparrey et al. [6] studied lumbar lordosis development, sagittal balance and lumbar lordosis in aging and reported that flattened lumbar deformity occurred in elderly people because of disc degeneration and vertebral osteoporotic compression fractures. This result conflicts with ours, likely for two reasons. In our study, we excluded patients with sequestrated disc herniation and vertebral collapse. Therefore our findings did not reveal loss of lumbar lordosis; on the contrary, lordosis increased during normal aging beginning at 50 years of age. Thus, vertebral collapse and severe loss of disc height may be considered the main pathologies responsible for flattened lumbar deformity (Fig. 3). Furthermore, our study included only women and we know that lumbar lordosis is 28% more frequent in women [15, 16].
The L5-S1 segment is the main site of lumbar lordosis and the most common region for degenerative changes [17]. Thus in our study the L5-S1 intervertebral disc was analyzed in detail. At this level, lumbar lordosis correlated with D-Cobb. The disc angle is formed by posterior height loss of the disc. Increased lordosis is associated with posterior height loss of the disc. Disc dehydration seen with advancing age becomes more prominent in the posterior disc, mainly due to center of gravity. Posterior vertebral wedging and increased D-Cobb may result from similar physical effects. However, no significant correlation was found between lumbar lordosis and L5-S1 or L1-L2 disc height. Because disc height was measured at mid disc, there was less effect resulting from dehydration than at the posterior disc. Lack of significant correlation between the ratio of L5/L1 vertebral height and lumbar lordosis can be explained with a similar theory to the disc height ratio. Increased lordosis was correlated with the height of the posterior vertebra and posterior disc, whereas loss of mid-level height was independent of lordosis.
One limitation of the present study is that lumbar MRI was performed with patients in the supine position; standing X-rays are more suitable for assessment of lumbar lordosis. However, when all assessed parameters are considered, MRI is a superior diagnostic tool. A second limitation is that our study included only patients with back pain.
In conclusion, strong spinal structure is maintained in women during physiological aging from 20 to 40 years of age; lumbar lordosis increases after 50 years of age. Lumbar lordosis is most strongly correlated with increased prevalence of L4 and L5 posterior vertebral wedging and loss of posterior height of the L5-S1 intervertebral disc. Multifidus muscle atrophy, which increases after 40 years of age, and obesity may play important roles in the pathophysiological process of increased lumbar lordosis. Vertebral compression fractures and severe loss of disc height may lead to hypolordosis.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
Thanks to Dr. Sevim Purisa for statistical evaluation.